Embed Size (px)
DESCRIPTION
OHSS: Prediction and prevention in non IVF cycles
Citation preview

OHSS: Prediction and prevention in non IVF cycles
Aboubakr ElnasharBenha university, Egypt

Types of ovarian Types of ovarian stimulationstimulation
Induction of ovulation
Superovulation
Controlled ovarian stimulation
Patient Anovulatory Anovulatory or ovulatory
Objective One mature follicle
> 1 >3
Example IUIUnexp inf
IVF
Method Stimulation Stimulation Down regulation StimulationPrevent premature LH surge
Aboubakr Elnashar

DefineSystemic synd resulting from vasoactive products released by hyperstimulated ovaries.
An iatrogenic complication of COS.
Life threatening
Aboubakr Elnashar

Mild Moderate Severe Critical
Cl •Ab bloating•Mild ab pain
•Mod ab pain•N± V
• Ascites•Oliguria
•Tense ascites•Oligo/anuria•Thromboembolism•ARDS
US Ov: ‹8 cm* •Ascites•Ov: 8–12 cm*
•±hydrothorax•Ov›12 cm*
•large hydrothorax
Lab •Hct ›45%•Hypoproteinaemia
•Hct›55%•WCC›25 000/ml
TT Out pt Out pt, In pt: unable tocontrol pain, Nwith oral tt,Difficulties inmonitoring
•In pt •ICU
Degrees: Mathur, 2oo5
Aboubakr Elnashar

Non IVF IVF
Mild 8.0-23% 100%
Moderate 0.005-7% 21- 44%
Severe 0.008 -10% 1- 10%
Incidence Varies:1.Protocol of ovarian stimulation2. Patient3. Classification schemesAn increase in the incidence of Severe forms of OHSSPatients hospitalized (Abramov et al., 1999; Cunha-Filho et al., 2003).
Elenany, 2013:
Aboubakr Elnashar

True incidence: unk Worldwide: Far greater Underestimated (Bewley et al 2011)
Causes 1. ARDS2. Cerebral infarction3. Hepatorenal failure Mortality from OHSS: unacceptable.
Aboubakr Elnashar

PredictionI.Before stimulationThe most important: PCOS & history of OHSS
1. OHSS in a previous cycle2. PCOS (Met or LOD)3. Young patient: ≤30 y4. BMI: ≤205. Basal investigations (NICE, 2013)
Total AFC > 16 AMH>3.5 ng/ml (25.0 pmol/l) FSH<4 IU/l
Aboubakr Elnashar

Aboubakr Elnashar

II. During stimulation1. US : Number of the immature follicles is more important than the number of mature follicles in predicting OHSS. >4 follicles ≥ 14 mm (Kamrava et al., 1982; Hugues et al., 2006).
Doppler: low intraovarian vascular resistance
Combination of E2 & US: best chance for prediction
Aboubakr Elnashar

2. E2 High E2<1000 pg/ml: No OHSS1500-2000risk of OHSS is significant
>2000 pg./ml: hCG is not given Cases with severe OHSS are seen with E2
<1500 pg/ml. Slope rise of E2 value is doubledMore accurate
Aboubakr Elnashar

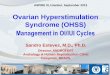
Moderate OHSS. Both ovaries are enlarged and are observed in the posterior cul-de-sac. The ovaries are in close contact and displace the uterus anteriorly. Both ovaries contain several large unruptured follicles.Aboubakr Elnashar

Aboubakr Elnashar

PreventionOHSS must be prevented rather than treated
I. Modified stimulation protocols1.HMG a.Lower dosesb. Chronic low dose step up protocol 2. HCGa.HCG Withholding b.Decrease HCG dosec.Replacing3. Progesterone for LPS not HCG.
Aboubakr Elnashar

II. Close Monitoring1.US2.E2
III. Modification of technique Convert to IVF
IV. Adjuvant1. IV albumin 2. 6% Hydroxyethyl starch3. Metformin 4. Dopamin agonist5. Ca gluconate
Aboubakr Elnashar

I. Modification of Protocols1. HMGI. Step-up:1. Low dose
2. Chronic low dose
II. Step-down
Aboubakr Elnashar

The starting dose of Gnt Depend on: 1. The intended goal: unifollicular ovulation or superovulation 2. Age3. BMI4. PCOS5. Ovarian reserve: baseline FSH, ACF, AMH6. Previous response.
Aboubakr Elnashar

low-dose •Stating dose: 75 IU/d (White et al., 1996; Hayden et al., 1999; Balasch et al., 2000; Calaf et al., 2003).
•Duration of starting dose: 5-7 d-No follicle development: increase the dose by 100% -Follicle growth: maintain same dose until follicular selection is achieved. -Mono-ovulation: 69% - MP: 5.7%- OHSS: 0.14% (Homburg & Howles, 1999. Hum. Reprod. Update 5:493-499).
Aboubakr Elnashar

Starting dose:75 IU/d
IfIf
Follicle Follicle >> 12 mm 12 mmE2 E2 >> 400 400
ContinueContinue11 FSH/dFSH/d
No response →150 FSH/d for 1 more w (max. 3 amp.(
Endocrine Rev. 1997; 18: 71Endocrine Rev. 1997; 18: 71
75 FSH/hMG/day
Day 3 Day 75 days
Aboubakr Elnashar

Chronic low-dose•Starting dose: 37.5-75 IU•Duration of starting dose:14 d•The weekly dose increment: reduced from 100% to 50% or 37.5 IU(Seibel et al., 1984; Polson et al., 1987; Sagle et al., 1991; Dale et al., 1993).
:Markedly ↓excessive ov stimulation Marked ↓OHSS.
Aboubakr Elnashar

0 14 21 28 35
75 iu112.5 iu
150 iu187.5 iu
225 iu
Days
7
37.5 iu
½ Amp.
One Amp.
42 49
2 Amp.
3 Amp.
White et al. J Clin Endocrinol Metab 1996;81:3821–4Aboubakr Elnashar

2. Step down protocol in PCOS (2nd line) • Mimics hormonal pattern in natural cycle. • Starting dose: once dominant follicle of 12 mm• Reduce dose by 37.5 IU sequentially • Not preferred
Aboubakr Elnashar

2. HCGa. HCG Withholding: Rationale: hCG is the main triggering cause of OHSSCycle cancellationfinancial and emotional implications, frustrates both patient and physicianCycle cancellation before administration of HCG is an effective strategy for the prevention of OHSS, but the emotional and financial burden it imposes on patients should be considered before the cycle is cancelled. (III-C)
Aboubakr Elnashar

b. Decrease HCG dose: As low as 3300 IU 2000 IU: ineffective, lower successful oocyte recovery(Kashyab et al, 2010).
does not prevent OHSS (Kol, Dor, 2009)
There is no clear evidence that lowering HCG dose will result in a decrease in the rate of OHSS. (III)
Aboubakr Elnashar

d. Replacement of hCG a.HP HCG (Choriomon): No difference b.Rec HCG: (Ovitrell) No difference d. Rec LH (Luveris)safer than hCGtoo expensiveDosage:15,000–30,000 IUThe use of either LH or HCG for final oocyte maturation does not influence the incidence of OHSS. (I)
Aboubakr Elnashar

d. GnRHaNo cases of moderate/severe OHSS in 1,152 cycles Requires use of GnRHan in COS
GnRHa short half-life (3-5 h) eliminates the risk of OHSS in nonconception cycles.PR: 17%, with a low rate of multiple pregnancy.
Aboubakr Elnashar

3. Progesterone for LPS not HCG.
Progesterone, rather than HCG, should be used for LPS. (I-A)
Aboubakr Elnashar

II. Monitoring in superovulationI. US• Assessing the follicular maturity • Growth rate: 2- 3 mm/d in a stimulated cycle. • Follicle 18—20 mm: contain a mature oocyte.SerialD5-7 of stimulation. D4: PCOS Repeat /2-3 d depending on the size of leading follicle,
until it is 18 mm
Aboubakr Elnashar

a. Follicles:number & sizeDocumentation of all follicles >10 mm {predict the
risk of multiple pregnancies}. 1 or 2 follicles 18-20 mm: HCG >4 follicles ≥ 14 mm: stop HCG (Kamrava et al., 1982; Hugues et al., 2006).
Aboubakr Elnashar

II. E2• Correlates closely with the stage of development of the dominant follicle • D8 stimulation E2 >200 pg / ml indicates adequate dose of Gnt (Speroff et al, 2006).
E2 on day of HCG
<200pg./ml
500-1500 1500-2000 >2000
pregnancies are rare
optimal risk of OHSS is significant
HCG is not givenCycle is cancelled
Aboubakr Elnashar

III. Modification of techniqueRescue IVF
If we convert to IVF + freeze all embryos and then ET in next cycle (as cases with very high E2 levels are not only at high risk for OHSS but also lead to “out of phase endometrium” with lower implantation rates).
Aboubakr Elnashar

IV. Adjuvant1 - IV albumin: Immediately on the day of hCG Effectiveness:IV albumin does not reduce severe OHSS.(Youssef, Al-Inany et al, Cochrane Database Syst Rev 2011; Venetis : a systematic review and metaanalysis.2011)Albumin or other plasma expanders at the time of egg retrieval are not recommended for the prevention of OHSS. (I-E)
Aboubakr Elnashar

2. 6% HES slow infusion of 500 mL of 6% HES on day of
HCG significantly reduced the incidence of moderate-
severe OHSS
HAES Sterile= HES (6%) in isotonic saline or
Voluven= 500 ml (68 EP)
Aboubakr Elnashar

HES Vs Albumin
Much cheaper
More effective
No anaphylactic reaction(Abramov et al,2001; Chen et al, 2003)
HES markedly decreases the incidence of severe OHSS.
(Youssef, Al-Inany et al, Cochrane Database SR 2011; Venetis : SR and MA. 2011)
Aboubakr Elnashar

3. Dopamin agonist (cabergoline)0.5 mg daily for 8 days from day of hCG (Seow et al, 2013)
Type 2 receptors for VEGF are believed to be involved in the pathophysiology of OHSSEffective for the prevention of OHSS. without sacrificing PR (Esinler et al, 2013).
Reduces the incidence, but not severity of OHSS, without compromising pregnancy outcomes.(Yousef et al, 2010, SR and MA)
Aboubakr Elnashar

less effective for tt of OHSS. (S R and MA., Baumgarten et al, 2013)
Cabergolin VS IV albuminmore effective and less costly(Tehraninezad et al, 2012)
Cabergoline starting from the day of HCG reduces the incidence of OHSS in patients at higher risk and does not appear to lower PR. (II-2)
Aboubakr Elnashar

4. Metformin in PCOSMechanism: reduction of intraovarian androgen by reducing hyperinsulinism: reduction in E2 and favours orderly follicular growth in response to exogenous GnT reduction of AMH and a reduced insulne dependent VEGE (Tang et al 2006)
reduces the risk of OHSSno effect on CPR or LBRimproves the rates of miscarriage and implantation (Palomba et al, 2013).
The addition of metformin should be considered in patients with PCOS because it may reduce the incidence of OHSS. (I-A)given 2 months before starting stimulation (Castello et al 2006)
Aboubakr Elnashar

5. Calcium gluconate 10 ml of 10% solution in 200 ml NS within 40 min of
OR and continued on day 1, day 2 and day 3.prevent severe OHSS and decreases OHSS
occurrence ratesCa gluconate Vs Cb2 comparable success rates(Naredi et al, 2013).
Aboubakr Elnashar

Key Take home Messages(Rizk B., 2010)
Primary prevention1. Prediction of OHSS from history, exam, and US2. LOD in PCOS 3. Metformin in PCOS 5. Close monitoring during stimulation6. Low-dose gonadotropins6. Chronic low dose protocol
Aboubakr Elnashar

2ndry prevention1. Withholding hCG if S/S of mild OHSS or E2: 1500 2. Rescue IVF3. GnRHa or Rec LH to trigger ovulation4. Progesterone for LPS5. Dopamine agonist6. HES 6%
Aboubakr Elnashar

Thank youFacebook
https://www.facebook.com/groups/227744884091351/
Aboubakr Elnashar




![Whether Letrozole could reduce the incidence of early ......OHSS, so prevention seems very important [10]. For the women at high-risk of OHSS, an important means to prevent OHSS is](https://img.pdfslide.net/doc/110x75/61353f3fdfd10f4dd73c4021/whether-letrozole-could-reduce-the-incidence-of-early-ohss-so-prevention.jpg)