Embed Size (px)
Citation preview

0022-5347/94/1524-1232$03.00/0THE JOURNAL OF UROLOGY
Copyright © 1994 by AMERICAN UROLOGICAL AsSOCIATION, INC.
Vol. 152, 1232-1237, October 1994Printed in U.8.A.
ONE-STAGE REPAIR OF HYPOSPADIAS: IS THERE NO SIMPLEMETHOD UNIVERSALLY APPLICABLE TO ALL TYPES OF
HYPO SPAD lAS?
TOMOHIKO KOYANAGI, KATSUYA NONOMURA, TETSUFUMI YAMASHITA, KOUICHI KANAGAWAAND HIDEHIRO KAKIZAKI
From the Department of Urology, Hokkaido Uniuersity School of Medicine, Sapporo, Japan
ABSTRACT
A simple method ofhypospadias repair is described. The operative technique consists of7 steps,including 1) outlining the skin incision and dartos mobilization; 2) artificial erection, harvestingparameatal foreskin flap and release of chordee as needed; 3) glans splitting and creation ofglanular wings; 4) l-stage urethroplasty with parameatal foreskin flap; 5) meatal glanuloplasty;6) creation of Byars' flaps of the skin, and 7) skin closure. Central to the technique is thefeasibility of the choice of l-stage urethroplasty with meatal based manta-wing flap or withparameatal based and fully extended circumferential foreskin flap even after the skin incision ismade, which enables its application to all types of hypospadias. Of 120 patients the l-stageurethroplasty was performed with meatal based manta-wing flap in 50, and with parameatalbased and fully extended circumferential foreskin flap in 70. Primary success was obtained in82% ofthe cases with meatal based manta-wing flap, and in 53% with parameatal based and fullyextended circumferential foreskin flap. Complications requiring secondary repair occurred in 42cases (9 with meatal based manta-wing flap, and 33 with parameatal based and fully extendedcircumferential foreskin flap) but repair was successful in 32. Thus, the overall success rate was91% (96% with meatal based manta-wing flap, and 87% with parameatal based and fullyextend d circumferential foreskin flap). Additional repair 10 secondary, 2 tertiary and 1 quaternary) is planned in 13 cases. The technique of l-stage urethroplasty with parameatal foreskinflap is recommended as a simple and reliable treatment for hypospadias with a reasonablesuccess rateo
KEy WORDS: hypospadias; penis; urethra; surgery, operative
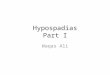
In step 2 artificial erection, harvesting parameatal foreskin flap(s) and correction of chordee are performed asneeded. After dartos mobilization and artificial erection aredone and if chordee is absent, as in most cases of distalhypospadias,7 an adequate length of flap is harvested fromeither side of the parameatal foreskin (figs. 2, e to F and 3).If chordee is present, as in most cases of proximal hypospadias, flaps are harvested from both sides of the parameatalforeskin and joined by transecting the urethral plate. Theurethra with bilateral parameatal foreskin flaps is detachedfrom the ventral corpora as in classic chordee correction untilthe shaft straightens (figs. 4, e to G and 5).
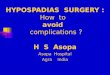
In step 3 the glans are split and glanular wings are created. When chordee is absent or released by dartos mobilization alone an incision parallel to both sides of the urethralgroove is made and the glans is split, thus preserving theurethral plate (figs. 2, F and G, and 3). When the urethra issevered the glans is split by a vertical midline incision. Theincision is deepened to the level of the corpora, and glanularwings are created by judicious lateralization of the glanularsubstance, literally splitting the glans (figs. 4, H to J and 5).8Because of the separate origin of the glans, urethra andcorporeal body,9 this dissection can usually be accomplishedanatomically without undue bleeding.
In step 4 the l-stage urethroplasty with parameatal foreskin flap is performed. When the urethral plate is preservedthe parameatal foreskin flap is simply onlayed to form theneourethra (figs. 2, H and 3).10 When the urethral plate istransected and severed the neourethra is formed by tubular-izing bilateral parameatal foreskin flaps, and is anchored tothe tip of the split glans.ll Due to urethral mobilization at
1232
Accepted for publication February 25, 1994.
Numerous operative techniques have been reported for therepair of hypospadias. Those who engage in the treatment ofthis difficult problem must be well acquainted with a varietyofthese techniques, which reportedly number more than 200.A l-stage repair has evolved in the last 2 decades and is nowthe standard treatment.1 In the majority of distal hypospadias cases a remarkably high success rate can be expectedwith a single stage repair.2 Nevertheless, in the repair ofproximal hypospadias in which the deformity is much moresevere the l-stage techniques have a limited role and only afew will correct all ofthe concurrent deformities (for examplehypospadiac urethra with severe chordee, ventrally tiltedglobular glans with dorsal skin hood and pro-penile bifidscrotum).3,4 Consequently a staged repair is still recommended for these difficult cases.5 However, if a simple singlestage method were universally applicable to all types of hypospadias, from mild (glanular and coronal) to moderate(penile and distal-to-penoscrotal) to more severe (scrotal andperineal) it would be of immense benefit. We believe that al-stage urethroplasty with parameatal foreskin flap is thetechnique that will meet this demand.6
OPERATIVE TECHNIQUE
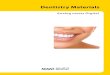
The steps of the procedure are outlined in figure 1. In step1 the skin incision and dartos mobilization are outlined.Regardless of the type of hypospadias a skin incision is madeencircling proximal to the meatus and extending dorsolaterally, including adequate parameatal foreskin (figs. 2, A andB, 3, 4, A and B, and 5).

ONE-STAGE REPAIR OF HYPOSPADIAS 1233
FIG. 1. Flowehart of operative teehnique. PF, parameatal flap.OUPF-II, l-stage urethroplasty with meatal based manta-wing foreskin flap. OUPF-N, l-stage urethroplasty with parameatal basedand fully extended eireumferential foreskin flap.
RESULTS
In the last 10 years 120 patients 2 to 12 years old (meanage 3.7 years) underwent this procedure, including 50treated with meatal based manta-wing flap and 70 treatedwith parameatal based and fully extended circumferentialforeskin flap. In a third of the procedures with parameatalbased and fully extended circumferential foreskin flap dartosmobilization alone was insufficient to release the chordee inwhat seemed to be distal hypospadias. Overall 70 cases werecured primarily without complications. Small fistulas occurred in 8 cases but they all healed within 2 months. Including these cases, primary success was accomplished in82% (41 of 50 cases) and in 53% (37 of 70 cases). Complications necessitated secondary repair in 42 cases, includingmea tal stricture requiring recession or glanular dehiscencewith meatal recession in 15 (3 with meatal based manta-wingflap, and 12 with parameatal based and fully extended circumferential foreskin flap), urethrocutaneous fistula in 21 (6
lar and frenal portions of the distal urethra. The rest of theslightly protruding urethral edge is everted and sutured tothe glanular edge in a semi-cufffashion. When complete, thevertically slit meatus opens at the most distal end of theglans, which was restored to a normal cone shape from asomewhat ventrally tilted and globular shape (figs. 2,1 and 3to 5).
In step 6 Byars' flaps are created with the dorsal foreskinand its subcutaneous tissue (figs. 2, J and 3 to 5). In step 7the skin is closed (figs. 2, K and 3 to 5). Steps 6 and 7 areessentially the same as reported previously.lO, 11However, inproximal hypospadias when a pro-penile bifid scrotum isoften a concurrent deformity, at step 1the scrotum must bemobilized extensively and at step 6 Byars' flaps must be createdwith enough subcutaneous tissue to reposition it ventral andposterior to the penile shaft.11 The specific details of eachstep have been described previously.1O-12
Postoperatively, all cases are managed with urethraldrainage using an indwelling 6F silicone catheter for 1weekin those with meatal based manta-wing flap and for 2 weeks inthose with parameatal based and fully extended circumferential foreskin flap. Wound dressing and treatment afterremoving the catheter have been reported previously.lO. 11
\Bilateral PF with
___ ehordee _(-) (+)
"" Harvesting PF /
/Unilateral PF
Outlining of skin incision snd dartos mobilization
Byarsization of dorsal foreskin sud subcutaneous tissue
Step l.
Step 2.
Step 3.
Step 4.
Step 7.
Step 6.
Step S.
correction of chordee (step 2) there should not be any tensionin anchoring the neourethra to the glans (figs. 4, K to Mand 5).
In step 5 the glans wings are approximated over the neourethra as well as paraglanular foreskin to cover the glanu-
D!§
FIG. 2. Sehematie of l-stage urethroplasty with meatal based manta-wing foreskin flap

1234 ONE-STAGE REPAIR OF HYPOSPADIAS
FIG. 3. Photographof l-stage urethroplastywith meatal basedmanta-wingforeskinflap
with meatal based manta-wing flap, and 15 with parameatalbased and fully extended circumferential foreskin flap) andurethral stricture in 6 with parameatal based and fully extended circumferential foreskin flap. Secondary proceduresin 32 cases (extension urethroplasty in 15 and fistula closure in17) provided satisfactory results in 29. Thus, the overall
success rate was 91% (96% with meatal based manta-wingflap, and 87% with parameatal based and fully extendedcircumferential foreskin flap). Functional and cosmetic outcome was satisfactory with both techniques (fig. 6). Additional repair is planned in 13 cases (10 secondary, 2 tertiaryand 1 quaternary).

ONE-STAGE REPAIR OF HYPOSPADIAS
H
i~ n
FIG. 4. Sehematie of l-stage urethroplasty with parameatal based and fully extended eireumferential foreskin flap
e A \ B
Step 7FIG. 5. Photograph of l-stage urethroplasty with parameatal based and fully extended eireumferential foreskin flap
o
1235

1236 ONE-STAGE REPAIR OF HYPOSPADIAS
A advancement and glanuloplasty or the flip-flap technique isprobably indicated.
With our procedure the neourethra is in natural continuitywith the old urethra, allowing less chance of complication atthe junction. Urethras thus formed continue to grow, asillustrated by our 13-year-old patients. Compared to theglans piercing technique, our meatal glanuloplasty seems tobe embryologically as well as anatomically more sound,9 andit provides cosmetically and functionally satisfactory results.Moreover, the skin closure allows a pro-penile scrotum to berepositioned ventral and posterior to the penile shaft, whichenables substantial correction of concurrent deformities evenin the severest form ofhypospadias, all in a single stage. Werecommend that the l-stage urethroplasty with parameatalforeskin flap be added to the armamentarium as a simple andreliable l-stage method for all types of hypospadias with areasonable rate of success.
FIG. 6. Outcome of l-stage urethroplasty with meatal basedmanta-wing foreskin flap (A), and parameatal based and fully extended circumferential foreskin flap (E).
DISCUSSION
Although it is an established fact that chordee is sometimes absent or is relieved by dartos mobilization alone, it isdifficult to predict the severity of chordee preoperatively. Inglanular or coronal hypospadias it is absent in most cases,thus enabling repair with meatal advancement and glanuloplasty, and/or the flip-flap technique.2 In other distal-topenoscrotal hypospadias dartos mobilization alone is oftenadequate to relieve chordee,7 allowing various l-stage repairs with preservation of the urethral plate.13.14Artificialerection with the patient under anesthesia before skin incision may be helpful in selecting the operation of choice but itseems cumbersome. Furthermore, in what appears to be distal-to-penoscrotal hypospadias dartos mobilization alonefails to relieve chordee in a third of the cases.6 Althoughurethral mobilization may help, 15-17if it does not the urethra must be transected before undergoing l-stage repair, ofwhich the currently most reliable is the transverse preputialisland flap (the Duckett procedure).18 This technique hasbeen used in the severest form ofhypospadias, combining theThiersch-Duplay urethroplasty of the proximal urethra.3 Asimple method applicable to all types of hypospadias is desired because of such unexpected situations.
The l-stage urethroplasty with parameatal foreskin flaptechnique as described is unique in this regard. It requires noplanned skin incision, as in most repairs, except the initialincision (step 1), which is essentially the same regardless ofthe type ofhypospadias. The technique differs only at step 4.After dartos mobilization there are just 2 ways to form theneourethra (with meatal based manta-wing flap, and withparameatal based and fully extended circumferential foreskin flap), the choice ofwhich is made at the time of artificialerection. Allowing this intraoperative choice depending onthe degree of remaining chordee considerably simplifies theprocedure.
Viability of the parameatal foreskin flap even in casestreated with parameatal based and fully extended circumferential foreskin flap is well established.19 When blood flowmeasured on laser Doppler was compared at the tip of theparameatal flap before and after harvesting there was onlyan 18% reduction with parameatal based and fully extendedcircumferential foreskin flap. In comparison to the meatalbased ventral midline flap, the parameatal flap also hasconsiderably better microcirculatory parameters (for example flow reduction rates with the flip-flap and with meatalbased manta-wing flap were 73% and 33%, respectively)/9which is why we prefer the latter procedure when meatal
REFERENCES
1. Duckett, J. W.: Hypospadias. In: Campbell's Urology, 6th ed.Edited by P. C. Walsh, A. B. Retik, T. A. Stamey and E. D.Vaughan, Jr. Philadelphia: W. B. Saunders Co., vol. 2, chapt.50, p. 1897, 1992.
2. Wacksman, J., Sheldon, C. and King, L. R: Distal hypospadiasrepair. In: Reconstructive Urology. Edited by G. Webster, R.Kirby, L. King and B. Goldwasser. Boston: Blackwell Scientific, vol. 2, chapt. 53, pp. 749-762, 1993.
3. Ehrlich, R. M. and Scardino, P. T.: Surgical correction ofscrotaltransposition and perineal hypospadias. J. PedoSurg., 17: 175,1982.
4. Woodard, J. R and Parrott, T. S.: Management of severe perineal hypospadias with bifid scrotum. J. Urol., part 2, 145:245A, abstract 132, 1991.
5. Duckett, J. W.: Hypospadias. In: Reconstructive Urology. Editedby G. Webster, R Kirby, L. King and B. Goldwasser. Boston:Blackwell Scientific, vol. 2, chapt. 54, pp. 763-780, 1993.
6. Koyanagi, T., Nonomura, K and Asano, Y.: One stage urethroplasty with parameatal foreskin-flap (OUPF): simple methoduniversally applicable to all types of hypospadias repair. J.Urol., part 2,147: 317A, abstract 419,1992.
7. Marshall, M., Jr., Beh, W. P., Johnson, S. H., III, Price, S. E., Jr.and Barnhouse, D. H.: Etiologic consideration in penoscrotalhypospadias repair. J. Urol., 120: 229, 1978.
8. Turner-Warwick, R: Hypospadiac and epispadiac retrievoplasty. In: Reconstructive Urology. Edited by G. Webster, RKirby, L. King and B. Goldwasser. Boston: Blackwell Scientific, vol. 2, chapt. 55, pp. 781-794, 1993.
9. Altemus, A. R and Hutchins, G. M.: Development ofthe humananterior urethra. J. Urol., 146: 1085, 1991.
10. Koyanagi, T., Nonomura, K, Asano, Y., Gotoh, T. and Togashi,M.: Onlay urethroplasty with parameatal foreskin flap fordistal hypospadias. Eur. Urol., 19: 221, 1991. _
11. Koyanagi, T., Nonomura, K, Kakizaki, H., Takeuchi, 1. andYamashita, T.: Experience with one-stage repair of severeproximal hypospadias: operative technique and results. Eur.Urol., 24: 106, 1993.
12. Nonomura, K, Koyanagi, T., Kakizaki, H., Takeuchi, 1. andMoriya, K: One-stage repair with parameatal foreskin flap forall types ofhypospadias. J. Urol., part 2,147: 188A,videotapeV-1,1992.
13. King, L. R: Hypospadias-a one-stage repair without skin graftbased on a new principIe: chordee is sometimes produced bythe skin alone. J. Urol., 103: 660, 1970.
14. Elder, J. S., Duckett, J. W. and Snyder, H. M.: Onlay island flapin the repair ofmid and distal hypospadias without chordee. J.Urol., 138: 376, 1987.
15. Koyanagi, T., Matsuno, T., Nonomura, K and Sakakibara, N.:Complete repair of severe penoscrotal hypospadias in 1 stage:experience with urethral mobilization, wing flap-flipping urethroplasty and "glanulomeatoplasty." J. Urol., 130: 1150,1983.
16. Mollard, P., Mouriquand, P. and Felfela, T.: Application of theonlay island flap urethroplasty to penile hypospadias withsevere chordee. Brit. J. Urol., 68: 317,1991.
17. Monfort, G., Bretheau, D., di Benedetto, V. and Bankole, R:

ONE-STAGE REPAIR OF HYPOSPADIAS 1237
Posterior hypospadias repair: a new technical approach. Mobilization ofthe urethral plate and Duplay urethroplasty. Eur.Urol., 22: 137, 1992.
18. Duckett, J. W.: The island flap technique for hypospadias repair.Urol. Clin. N. Amer., 8: 503, 1981.
19. Nonomura, K, Koyanagi, T., Imanaka, K and Asano, Y: Measurement of blood flow in the parameatal foreskin flap forurethroplasty in hypospadias repair. Eur. Urol., 21: 155, 1992.
EDITORIAL COMMENT
The authors present their extensive ongoing experience with whatI perceive as a complex hypospadias repair. They are to be complimented on their perseverance and on the illustrations, which finallyclarifYtheir technique for me. However, even with their vast experience the complication rate is higher with their procedure than thatcurrently achieved with other l-stage techniques. For hypospadiaswithout chordee they report an 18% complication rate (with meatalbased manta-wing flap). This group is amenable to a meatal basedflap (Mathieu) or the currently popular onlay repair. Complicationsnecessitating reoperation should be less than 5% and reoperationsare being performed by most on an outpatient basis, some withoutthe use of stents (the authors report 1 week of urethral stenting inthis group).
The authors also report a 47% complication rate (1 applaud theirhonesty) with parameatal based and fully extended circumferential foreskin flap repair. They state that vascularity of thepara meatal foreskin has been proved to be excellent on laserDoppler. In my experience mea tal stenosis (and stricture?) is aconsequence of diminished vascularity. Judging from their resultsI suspect that vascularity is not as excellent as they believe.Reoperation rate, even for those with severe hypospadias, shouldnot exceed 15%.In our experience using a de-epithelialized flap ortunica vaginalis to cover the transverse island tube fewer than10% of cases require a secondary procedure. I agree with theircomment that the currently most reliable repair is the transversepreputial island flap.
The argument that they advance (that the initial skin incision issimilar for all degrees of hypospadias) to justify their assertion thatthe repair is applicable generally confuses me. Other than withmeatal based repairs the skin incision for all others is basically thesame, subcoronal and proximal to the hypospadiac meatus. If anonlay is used the urethral plate is spared. The erection test can thenbe performed after the skin is dissected toward the penile base, if thesurgeon prefers.
The authors ask a question in the title: "Is there no simple methoduniversally applicable to all types of hypospadias?" Clearly, theanswer is, "No."
A. B. BelmanDepartment of UrologyChildren's Hospital National Medical CenterWashington, D. C.
Reply by Authors. In our earlier series in which only 1 of us (T. K)performed the operation the complication rate associated with asecondary operation was 8%(2 of25 cases) with meatal based mantawing foreskin flap (reference 10 in article) and 33% (6 of 18 cases)with parameatal based and fully extended circumferential foreskinflap. During the ensuing years a number of junior surgeons performed the repair, which may explain the relatively higher complication rate in the present series. Others have reported an evenhigher incidence (50%) of secondary operations with pedicle tubeurethroplasty and other techniques (reference 4 in article).2 Underour current national health program under which every citizen isentitled to uniform access to health care provided by the governmentor an insurance company there is no urgency or impetus in promoting short hospital stay or outpatient surgery. Rather the providersprefer inpatient care until the wound heals, which may explain thelonger urethral catheter drainage and which we plan to shorten inthe future. There might have been a few cases in which the pedicleflap was harvested poorly, compromising its vasculature and contributing to complications. That the flap was harvested adequatelywas confirmed by the laser Doppler data. Consequently, the cause ofcomplication must lie elsewhere. Inadequate coverage of the neourethra with Byars' foreskin flaps can result in fistula, as can inadequate splitting and tight reapproximation of the glans over theneourethra with glanular deshiscence and meatal recession. Theanswer to the question in the title is "No," when one considers thecomplexity of the deformity and enormous task demanded for itsrepair but "Yes,"when it comes to the choice ofthe repair applicableto all types of hypospadias.
1. Nonomura, K, Koyanagi, T., Imanaka, K, Togashi, M., Asano,Y and Tanda, K: One-stage total repair of severe hypospadiaswith scrotal transposition: experience in 18 cases. J. PedoSurg., 23: 177, 1988.
2. Dewan, P. A., Dineen, M. D., Winkle, D., DuflY, P. G. andRansley, P. G.: Hypospadias: Duckett pedicle tube urethroplasty. Eur. Urol., 20: 39, 1991.