Embed Size (px)
Citation preview

OPPORTUNISTIC MYCOSESCLASSIFICATION ORGANISMS
Yeast CandidaCryptococcusTorulopsisTrichosporonRhodotorulaGeotrichium
Molds AspergillusPseudoallescheriaZygomycetes (Rhizopus, Mucor, and Absidia
Monday, January 16, 2012

OPPORTUNISTIC MYCOSES
True Pathogenic Fungi Opportunistic Fungi
Diseases HistoplasmosisBlastomycosisParacoccidioidomycosisCoccidioidomycosis
AspergillosisCandidiasisMucormycosisCryptococcosis
Host Normal Abrogated/Compromised
Portal of Entry
Primary infection is pulmonary
Various
Monday, January 16, 2012

OPPORTUNISTIC MYCOSESTrue Pathogenic Fungi Opportunistic Fungi
Prognosis 99% spontaneous resolution Recovery depends on the severity of impairment of host defenses
Immunity Resolution results to strong specific immunity
No specific resistance to infection
Host Response Tuberculoid granuloma, mixed pyogenic
Depends on degree of impairment necrosis to pyogenic to granulomatous
Morphology in Tissue
All agents showed dimorphism to a tissue form
No change in morphology
Distribution Geographically restricted Ubiquitous
Monday, January 16, 2012

CANDIDIASIS
C. albicans is the most common (4-6 um; budding)
Multiplication: blastospore formation producing either pseudohyphae or septate hyphae
Identification: assimilation and fermentation of CHOs; physiologic and morphologic responses they exhibit when grown under controlled nutritional conditions “germ tubes”
Monday, January 16, 2012

CANDIDIASIS
“chlamydoconidia”
Monday, January 16, 2012

FACTORS THAT AFFECT CANDIDA NORMAL POPULATION
poor oral hygiene
use of antibiotics
use of oral contraceptives
diet
presence of antagonistic inhibitory bacteria
Monday, January 16, 2012

Candida albicans is a resident flora of the skin, mouth, vagina and stool!
Imbalance will lead to infection....HOW?
Changes in the Physiology: e.g. pregnancy, use of steroids and diabetes
Prolonged administration of antibiotics
Immunocompromised patients
Monday, January 16, 2012

MUCOCUTANEOUS CANDIDIASIS (MC)
a condition caused by a fungus from the candida family (lives on the surface of skin) that develops a diffuse and persistent type of infection of the mouth, nails, skin, and at times other organs
affects infants (starts before age 3) and young adults, is rarely seen in adults with other diseases
including chronic mucocutaneous candidaisis or CMCC
Monday, January 16, 2012

SYMPTOMS: ORAL
“thrush” “glossitis” “stomatitis”
“cheilitis” “perleche”
Monday, January 16, 2012

SYMPTOMS: VAGINITIS & BALANITIS
“VAGINITIS = female”
“BALANITIS = male”
Monday, January 16, 2012

“Esophageal growth”
OTHERS: gastritis, peritonitis, enteric and perianal disease
SYMPTOMS: ALIMENTARY
Monday, January 16, 2012

CANDIDIASIS IN NAILS
Monday, January 16, 2012

CANDIDIASIS IN DIAPER RASH
“Candida may come from fecal origin”
Monday, January 16, 2012

SYSTEMIC INVOLVEMENT
Urinary tract
Endocarditis
Meningitis
Septicemia
Latrogenic candidemia
Dissemination to other organ systems
Monday, January 16, 2012

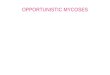
DISSEMINATED CANDIDIASIS
originate at a gastrointestinal site
CA enters epithelial microvilli through persorption of yeast cells or by germination (a,c)
In both cases, organisms enter the vasculature (b,d) for dissemination into tissues such as the kidney (e)
localizes in the cortex (f) where it grows as hyphae/pseudohyphae
A vigorous host response occurs at this site consisting of both mononuclear and polymorphonuclear leukocytes
Virulence factors (adhesins, morphogenesis, switch phenotypes, antioxidant proteins and invasive enzymes) promote the invasion of the organism
Monday, January 16, 2012

ALLERGIC CANDIDIASIS
Eczema
Asthma
Gastritis
Monday, January 16, 2012

LABORATORY DIAGNOSIS: CADIDIASIS
Direct microscopic examination
Specimen for examination can be sputum, skin scrapings, vaginal swabs, biopsy material, from any types of organs or even in blood.
The specimen is treated with 1-2 drops of 10-20% KOH.
Monday, January 16, 2012

LABORATORY DIAGNOSIS: CADIDIASIS
The presence of the capsule and budding yeast cells are considered as the positive results.
Aside from KOH, other stains can be used such as India ink and Papanicolaou stain.
Monday, January 16, 2012

GERM TUBE TEST
Most isolates of C. albicans produce a hyphal growth from blastospores when they are suspended in serum at 37°C for 2-3 hours.
Monday, January 16, 2012

IN CULTURE...
SDA at either room temperature or at 37°C
Colonies: usually develop in 2-3 days as white, typical yeast colonies
In vitro: monomorphic, growing as non encapsulated yeast cells at any temperature
Monday, January 16, 2012

IN CULTURE...
Monday, January 16, 2012

FROM CORN MEAL AGAR
Monday, January 16, 2012

TREATMENT OF CANDIDIASIS
Most localized, cutaneous, candidiasis infections may be treated with any number of topical antifungal agents (eg, clotrimazole, econazole, ciclopirox, miconazole, ketoconazole, nystatin).
For Candida onychomycosis, oral itraconazole (Sporanox)
For Genitourinary tract candidiasis, VVC can be managed with either topical antifungal agents or
Monday, January 16, 2012

TREATMENT OF CANDIDIASIS
Caspofungin acetate (Cancidas) as a 70-mg loading dose is followed by 50 mg/d IV for a minimum of 2 weeks after improvement or after blood cultures have cleared.
Chronic mucocutaneous candidiasis is treated with oral azoles, either fluconazole (Diflucan)
Monday, January 16, 2012

ASPERGILLOSIS
One of the largest of the fungal genera
Hundred of species have been recorded
The most important species:
A. fumigatus
A. flavus
A. niger
Monday, January 16, 2012

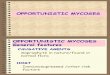
ASPERGILLUS FUMIGATUS
Aspergillus fumigatus
identified according to the pattern of conidiophore development, morphologic features and color of the conidia
Monday, January 16, 2012

IMPORTANT PARTS
Monday, January 16, 2012

SPECTRA OF ASPERGILLOSIS
Toxicity due to ingestion of contaminated foods
Allergy and sequelae to the presence of conidia or transient growth of the organism in body orifices
Colonization without extension in preformed cavities and debilitated tissues
Invasive, inflammatory, granulomatous, necrotizing disease of lungs and other organs
Systemic and fatal disseminated disease
Monday, January 16, 2012

ALLERGIC ASPERILLOSIS
Allergic aspergillosis maybe benign early on and severe as the patient grows older
In secondary colonization, a chronic clinical situation may exist with little distress except occasional bout of hemoptysis and some pathological changes in the lungs that may lead to the formation of fungus ball.
Monday, January 16, 2012

ALLERGIC ASPERILLOSIS
SKIN FUNGAL SPECIMEN IN THE TISSUE
Monday, January 16, 2012

SYSTEMIC ASPERGILLOSIS
An extreme serious disorder that is usually rapidly fatal unless diagnosed early and treated aggressively
The status of the host’s immune system contributes to the prognosis of the patient
Monday, January 16, 2012

SYSTEMIC ASPERGILLOSIS
FUNGUS BALL/ ASPERGILLOMA
Monday, January 16, 2012

Disease Etiologic Factors
Mycotoxicoses Ingestion of contaminated food products
Hypersensitivity peumonitis
Allergic bronchopulmonary disease
Secondary colonization
Colonization of preexisting cavity (pulmonary abscess) without invasion into contiguous tissue
Systemic disease Invasive disease involving multiple organs
Monday, January 16, 2012

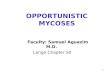
DISSEMINATED ASPERGILLOSIS
Aerosols of Aspergillus fumigatus conidia are inhaled and travel to the alveoli
In the healthy host, alveolar macrophages (AM) phagocytose and kill the organism after swelling of the conidium, an essential pre-germination stage
The production of reactive oxygen intermediates by AM is required to eliminate the organism, but polymorphonuclear cells (PMNs) also contribute
In the immunosuppressed patient, reduced numbers of PMNs and inefficient AM allow growth of the fungus
Consequently, the conidia germinate and escape from the AM
Monday, January 16, 2012

LABORATORY DIAGNOSIS
Aspergillosis is easy to isolate and identify....BUT!
also important to distinguish a true pathogen from a contaminant
If sputum sample is to be collected, it is expected to be thick and gelatinous
In invasive sampling, lung aspirates or tissue biopsy is used
Monday, January 16, 2012

LABORATORY DIAGNOSIS
Direct microscopic examination will show hyaline, dichotomously branched and septate hyphae
Occasionally in sputum, in cases of pulmonary aspergillosis, one may also sees very small, rough walled spores (3-4 um in diameter).
Monday, January 16, 2012

PULMONARY ASPERGILLOSIS
Monday, January 16, 2012

TREATMENT
Amphotericin B was used for many years BUT!!! with disappointing results
In 1990 itraconazole was introduced as a new broad spectrum anti-fungal agent.
Monday, January 16, 2012

ZYGOMYCOSIS/PHYCOMYSIS
Class Phycomycetes
Rhizopus
Absidia
Mucor
They formed coenocytic hyphae and reproduce asexually by producing sporangiosphores within which develops sporangiospores
Monday, January 16, 2012

ZYGOMYCOSIS/PHYCOMYSIS
Repeated isolation of the organisms from consecutive specimens provides strong evidence that the organisms may be relevant, even though coenocytic hyphal elements are not seen in histopathologic examination of tissue.
Monday, January 16, 2012

MUCORMYCOSIS (ORAL CAVITY)
Monday, January 16, 2012

CATEGORIES COMMENTS
Rhinocerebral It is the most frequent presentation overall and classically affects diabetics with ketoacidosis.
Usually presents with facial and/or eye pain, proptosis and progressive signs of involvement of orbital structures (muscles, nerves and vessels).
Common complications include cavernous sinus and internal carotid artery thrombosis.
Pulmonary It occurs most frequently among neutropenic patients.
It presents with nonspecific symptoms such as fever, cough and dyspnea; hemoptysis may occur with vascular invasion.
Radiological presentation includes segmental consolidation that progresses to contiguous areas of the lung, with occasional cavitation.
Gastrointestinal Usually affects patients with severe malnutrition
May involve the stomach, ileum, and colon
Clinical picture mimics intra-abdominal abscess. The diagnosis is often made at autopsy.
Cutaneous It has been reported with minor trauma, insect bites, no sterile dressing, wounds, and burns.
The necrotic lesions progressively evolve from the epidermis into dermis and even muscle.
Others Heart, bone, kidneys, bladder, trachea, and mediastinum
Monday, January 16, 2012

DIRECT EXAMINATION: ZYGOMYCOSIS
A rapid diagnosis is critical
Fungal elements are usually not numerous in discharges
Scrapings from the upper turbinates, aspirated material from sinuses, sputum in pulmonary disease, and biopsy material mounted in 10% KOH typically contain thick-walled, refractile hyphae 6-15 um in diameter
Swollen cells (up to 50 um) and distorted hyphae may be present
Monday, January 16, 2012

IN CULTURE...
Sabouraud dextrose agar: Incubate at 30°C
DON’T: cycloheximide = sensitive
Sterile bread:
for recovery of Zygomycetes when other media fail
WHY bread??? Monday, January 16, 2012

TREATMENT
Control of the diabetes
Aggressive surgical debridement of involved tissue
High doses of amphotericin B are recommended
Monday, January 16, 2012