Embed Size (px)
Citation preview

ORTHOPAEDICS PRESENTATION
M O H D A F I Q I F I K R IM M M C
M a l a y s i a
1

N A M E
A G E
A D D R E S S
O C C U P A T I O N
R E G I S T R A T I O N N U M B E R
D A T E O F A D M I S S I O N
D A T E O F E X A M I N A T I O N
PATIENT’S DETAILS
2
C H O N G S I U K A N G
6 7 Y / O
C H E N G M E L A K A
R E T I R E E
1 1 1 7 3 3 0
2 N D N O V E M B E R 2 0 1 6
4 T H N O V E M B E R 2 0 1 6

H I S T O RY

C H I E F C O M P L A I N T
Pain at left knee for 8 years

P A T I E N T ’ S
HISTORY OF PRESENTINGILLNESS
Patient was apparently well 8 years ago when he then develop pain on the left knee which is insidious in onset. The pain is pricking in nature, with pain score of 3/10, no radiation, which aggravated by walking and climbing stairs, and relieved by rest. However, the pain increases to the score of 7/10 for the past 2 months. This pain is associated with limited range of movement of the knee. Currently, pain is reduced to 2/10.
He also have similar complaint at her right knee, but it is milder compared to the left knee. Otherwise, he has no morning stiffness, no history of trauma or fall, no fever, no knee swelling, giving way, and locking.
5

P A T I E N T ’ S
HISTORY OF PRESENTINGILLNESSHe is able to ambulate without walking aid and use walking frame if there is pain.There’s no other joint involvement.
Intra-articular injection to the left knee was done one time in September 2015, the pain was partially relieved. However, the pain came back after 7 months.
He was currently admitted for left TKR surgery.
Upon admission, x-ray of the left knee was taken, analgesic was given.
6

PAST MEDICAL HISTORY
• Hypertension for 8 years • T. Amlodipine 10mg OD
• No Diabetes Mellitus, ischemic heart disease, tuberculosis, bronchial asthma
01.
FAMILY HISTORY
• His father has hypertension.• No family history of arthritis, malignancy, diabetes
mellitus, ischemic heart disease.
03.
PAST SURGICAL HISTORY
• No significant past surgical history02.
PERSONAL HISTORY
• Sleep does not disturbed• No loss of appetite and loss of weight• Normal bowel and bladder habit• Non smoker, non alcoholic• No known drug or food allergy
04.
7
SOCIOECONOMIC HISTORY
• married and blessed with 5 children• Live with his wife and son.• Previously work as a hard labor in construction yard
for 10 years• He is financially stable. – supported by his son
05.

P A T I E N T ’ S
PROVISIONALDIAGNOSIS PRIMARY OSTEOARTHRITIS OF THE LEFT
KNEE
• 67 years old obese patient• Pain at left knee for 8 years (long duration) with similar complaint at the
right knee• work as a hard labor in construction yard for 10 years• No history of trauma or fall• No fever, inflammation of the knee
8

PHYSICAL EXAMINATIONS
This includes general and local examination, of which consist of look, feel, move and measure and not forget the special tests.
P R I M A R Y O S T E O A R T H R I T I S O F T H E L E F T K N E E

P A T I E N T ’ S
GENERAL EXAMINATION
• Patient is lying comfortably in semi-recumbent position, alert and cooperative. She is moderately built and well nourished.
• BMI : 31.4 (Obese)• Vital signs were stable:
I. PR: 70 bpm, regular rhythm, normal volume and characterII. BP: 145/92 mmHgIII. RR: 18 breaths/minIV. Temperature : 37 ºC
• There is no pallor, no pedal edema.SYSTEMIC EXAMINATION
10
• Cardiovascular system, Respiratory system and Abdominal examination were all normal.

P A T I E N T ’ S
LOCAL EXAMINATION
STANDING POSITION• ANTERIOR
• Both hip extended and adducted, knee and ankle at neutral position.• There is genu varus deformity of the left leg• There is muscle wasting at the left thigh and left calf• There is apparent shortening of the left lower limb • There is no scars, no swelling
• LATERAL• There is no deformity, scars, swelling
• POSTERIOR• There is no swelling on the popliteal fossa, no scars.
• GAIT• Antalgic gait
LOOK
11

P A T I E N T ’ S
LOCAL EXAMINATION
SUPINE POSITION• ANTERIOR
• Attitude Hips: Both are flexed at 30˚ Knees: Both are flexed at 5º Ankles: Both are at neutral position.
• There is muscle wasting at the left thigh and left calf• There is apparent shortening of the left lower limb• There is no deformity of the left leg• There is no scars, no swelling
• LATERAL• There is no deformity, scars, swelling
LOOK
12

P A T I E N T ’ S
LOCAL EXAMINATION
• There’s local rise in temperature • There’s tenderness over the medial joint line of left knee• Crepitus is felt upon moving the left knee joint
FEEL
13

MOVEMENTKNEE JOINT RIGHT
LEFT
*Crepitus was felt and heard upon moving the left knee joint
Movement Right (active) Right (passive)Extension 0˚ 0˚
Flexion 0˚-110˚ 0˚-110˚
Movement Left (active) Active (passive)Extension 0˚ 0˚
Flexion 0˚-90˚ 0˚-90˚

MEASUREMENT
Measurement Right (cm) Left (cm)Apparent length
104 102
True length 85 84Segmental Length Above knee 44 44 Below knee 41 40

P A T I E N T ’ S
NEUROVASCULAR EXAMINATION
Peripheral pulse : CRT <2s, distal pulsations felt on both sides (dorsalis pedis artery and posterior tibial artery)
16
P A T I E N T ’ S
NEUROLOGICAL EXAMINATION
• Sensory examination is intact on both sides of the lower limb• Motor examination : Patient able to dorsiflexion and plantarflexion for left ankle joint.

P A T I E N T ’ S
SPECIAL TESTS
• Varus stress test : Positive• Valgus stress test : Negative• Patellar grinding test : Positive• Patellar tap: Negative • McMurray test: could not elicit due to pain
17

PAT I E N T ’ S
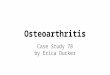
X-RAY
18
02/11/2016
AP VIEW• Narrowing of medial joint space• Subchondral sclerosis• Osteophytes
LATERAL VIEW • Narrowing of patellar space• Subchondral sclerosis

I N V E S T I G A T I O N S
FULL BLOOD COUNT
19
Hb 127 g/L 120.0-150.0
RBC 4.44 10^12/L 3.80-4.80
HCT 38.3 % 36.0-46.0
MCV 86 fL 83-101
MCH 28.7 pg 27.0-32.0
MCHC 33.2 g/dL 31.5-34.5
RDW-SD 40.3 fL 37.0-46.0
RDW-CV 13.2 % 11.6-14.0
Platelets 236 10^9/L 150-410

20
WBC 8.1 10^9/L 4.0-10.0
Lymphocytes # 2.8 10^3/uL 1.0-3.0
Neutrophil # 4.2 10^3/uL 2.0-7.0
Monocytes # 0.8 10^3/uL 0.2-1.0
Eosinophil # 0.2 10^3/uL 0.0-0.5
Basophil # 0.1 10^3/uL 0.0-0.1
Lymphocytes % 34.6 % 20.0-40.0
Neutrophil % 52.3 % 40.0-80.0
Monocytes % 10.4 % 2.0-10.0
Eosinophil % 1.9 % 1.0-6.0
Basophil % 0.8 % <1-2

21
ESR : 45 mm/hr (0-12)CRP : 7.2 mg/l (<5.0)

Primary osteoarthritis of left knee with genu varus deformity
DIAGNOSIS
22

T H U S FA R …
TREATMENT
TREATMENT IN HOSPITAL• Analgesics• Planned for left total knee replacement
23

DISCUSSIONo s t e o a r t h r i t i s

25
D I S C U S S I O N
OSTEOARTRITIS
DEFINITION Chronic disorder of synovial joints in which there is progressive softening and disintegration of articular cartilage and bone at the joint margins (osteophytes), cyst formation and subchondral sclerosis, mild synovitis and capsular fibrosis.

PRIMARY• Occurs in a joint de novo• Occurs in old age• Mainly in weight bearing joints (knee and hip)• More common than secondary OA
26
TYPES OF OSTEOARTHRITIS
D I S C U S S I O N
SECONDARY• There is underlying primary disease of the joint →
degeneration of the joint, often many years later• May occur at any age after adolescence• Commonly at the hip

O S T E O A R T H R I T I S
INVESTIGATIONSOA is typically diagnosed on the basis of clinical and radiographic evidence. No
specific lab abnormalities are associated with OA.
27
IMAGING• X-ray
I. Narrowing of the joint spaceII. Subchondral sclerosisIII. Marginal osteophytesIV. Subchondral cystV. Bone remodelling
RADIONUCLIDE SCANNING• Scanning with 99mTc-HDP
shows increased activity during the bone phase in the subchondral regions
CT and MRI
• To elucidate specific problem : bone edema, AVN

O S T E O A R T H R I T I S
INVESTIGATIONSOA is typically diagnosed on the basis of clinical and radiographic evidence. No
specific lab abnormalities are associated with OA.
28
Serological tests and ESR to rule out rheumatoid arthritis.
Serum uric acid to rule out gout.
Arthroscopy : if a loose body or frayed meniscus is suspected.

O S T E O A R T H R I T I S
TREATMENT
PRINCIPLES OF TREATMENT• Delay the occurrence• Stall progress of the disease and relieve the symptoms• To rehabilitate the patient

O S T E O A R T R I T I S
TREATMENTThe goals of osteoarthritis treatment include alleviation of pain and improvement of functional status. Optimally, pt should receive a combination on non-pharmacologic and pharmacologic treatment.
NON-PHARMACOLOGICAL• Patient education• Thermotherapy • Weight loss • Exercise• Physical therapy• Unloading in certain joints (eg, knee, hip)
30
PHARMACOLOGICAL• Acetaminophen• Oral NSAIDs• Topical NSAIDs• Tramadol• Intra articular injections

T R E A T M E N T
SURGICALAlthough osteoarthritis tends to be chronic, the symptoms are rarely progressive and rarely
require surgery on the painful spinal joints.
31
• Joint debridement• Osteotomy • Partial Knee Replacement Surgery
(Unicompartmental Knee Arthroplasty)• Total Knee Replacement Surgery (Total Knee
Arthroplasty)

32

INDICATIONS• relief of significant disabling pain caused
by severe arthritis• Correction of severe deformity
33
TOTAL KNEE REPLACEMENT SURGERY
S U R G E R Y

34
TOTAL KNEE REPLACEMENT SURGERY
S U R G E R Y
CONTRAINDICATIONS• Knee sepsis• A remote source of ongoing infection• Extensor mechanism dysfunction• Severe vascular disease• Recurvatum deformity secondary to muscular
weakness• Presence of a well-functioning knee arthrodesis
ABSOLUTE CONTRAINDICATIONS RELATIVE CONTRAINDICATIONS• Skin conditions within the field of surgery (eg,
psoriasis)• Past history of osteomyelitis around the knee• Neuropathic joint• Obesity

35

36
TOTAL KNEE REPLACEMENT SURGERY
S U R G E R Y
COMPLICATIONS OF TKR• Infection• Deep vein thrombosis• Common peroneal nerve palsy• Fractures• Extensor mechanism complications• Knee stiffness

REFERENCES
37
1) Apley’s System of Orthopaedics and Fractures 9th edition2) Maheshwari and Mhaskar Essential Orthopaedics 4th edition3) Raediopaedia.org4) Osteoarthritis: care and management. NICE guidelines Published
date: February 2014
T H A N K Y O U