Embed Size (px)
Citation preview

Patent Foramen Ovale management in Cryptogenic stroke -
Update on REDUCE and CLOSE trials
Naresh Mullaguri MDVascular Neurology Fellow
Cleveland Clinic Foundation
Cerebrovascular management conference
09282017
DISCLOSURES
NONE
OBJECTIVES1Case discussion
2 PFO and other types of Atrial septal defects
3 Relationship between PFO and cryptogenic stroke
4 RoPE score
5 Different Closure devices
6 Previous RCTs on PFO closure vs medical management
7 Current Guidelines from American societies regarding PFO
and cryptogenic stroke
8 Recent PFO closure trials and evidence
9 Perspectives
CASE SCENARIO
75 year old female with DM HTN had a fall and broke her right ankle sp ORIF 2
days later in OSH
Day 4 Acute SOB on the floor with some chest pain and hypoxemia Found to
have saddle PE and was started on IV Heparin She had an ECHO which showed
Right heart strain + PFO + Atrial septal aneurysm No intracardiac thrombus
Day 5 left sided hemiparesis and profound sensory loss NIH 7 CT head is
normal CTA of the Head and Neck showed acute right carotid artery occlusion with
saddle embolus at the bifurcation extending into the ECA Transferred to CCF main
campus
Her platelets were low at presentation and HIT was suspected by vascular
medicine
Hyperacute MRI showed posterior division diffusion restriction with large penumbra
and she was taken for thrombectomy
Post procedure TICI 3 Procedure was done under Bivalirudin due to suspicion of
HIT
Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
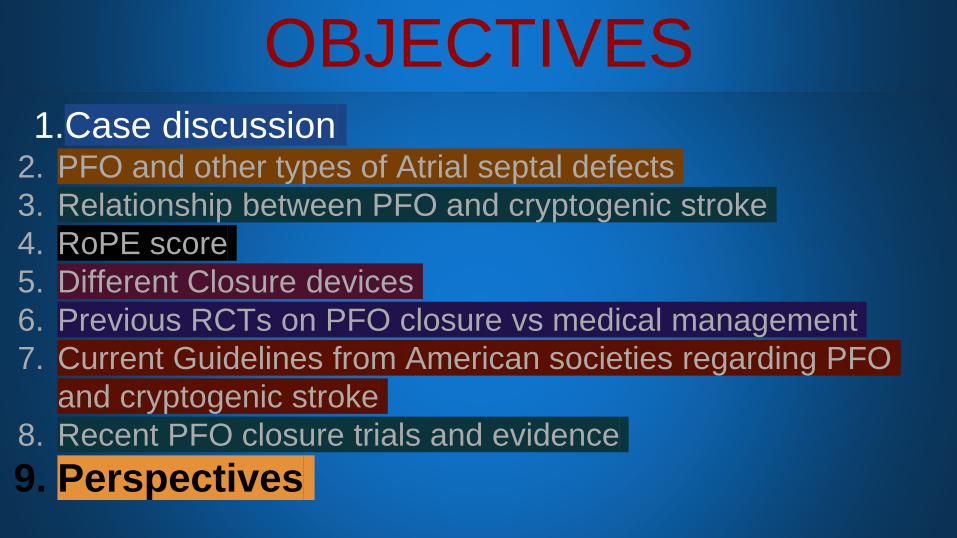
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
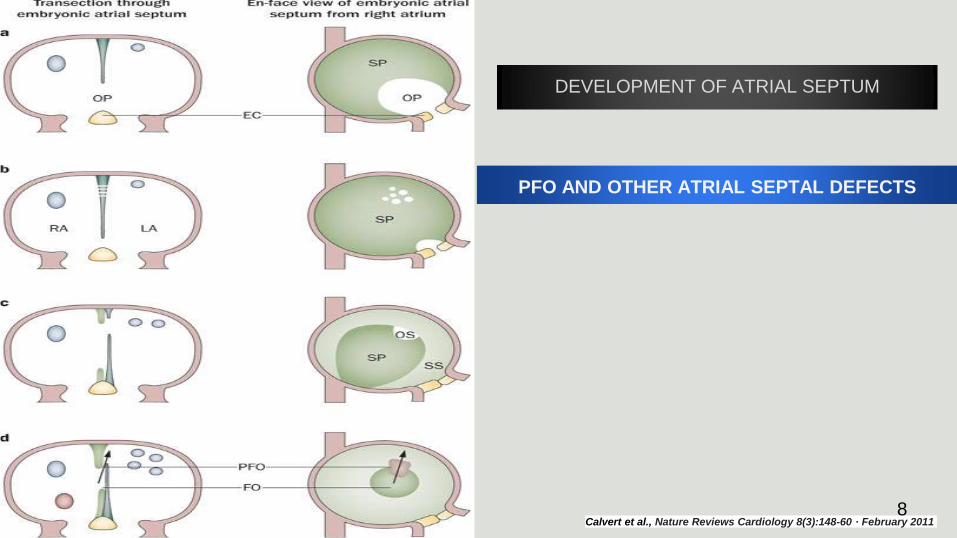
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

DISCLOSURES
NONE
OBJECTIVES1Case discussion
2 PFO and other types of Atrial septal defects
3 Relationship between PFO and cryptogenic stroke
4 RoPE score
5 Different Closure devices
6 Previous RCTs on PFO closure vs medical management
7 Current Guidelines from American societies regarding PFO
and cryptogenic stroke
8 Recent PFO closure trials and evidence
9 Perspectives
CASE SCENARIO
75 year old female with DM HTN had a fall and broke her right ankle sp ORIF 2
days later in OSH
Day 4 Acute SOB on the floor with some chest pain and hypoxemia Found to
have saddle PE and was started on IV Heparin She had an ECHO which showed
Right heart strain + PFO + Atrial septal aneurysm No intracardiac thrombus
Day 5 left sided hemiparesis and profound sensory loss NIH 7 CT head is
normal CTA of the Head and Neck showed acute right carotid artery occlusion with
saddle embolus at the bifurcation extending into the ECA Transferred to CCF main
campus
Her platelets were low at presentation and HIT was suspected by vascular
medicine
Hyperacute MRI showed posterior division diffusion restriction with large penumbra
and she was taken for thrombectomy
Post procedure TICI 3 Procedure was done under Bivalirudin due to suspicion of
HIT
Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
OBJECTIVES1Case discussion
2 PFO and other types of Atrial septal defects
3 Relationship between PFO and cryptogenic stroke
4 RoPE score
5 Different Closure devices
6 Previous RCTs on PFO closure vs medical management
7 Current Guidelines from American societies regarding PFO
and cryptogenic stroke
8 Recent PFO closure trials and evidence
9 Perspectives
CASE SCENARIO
75 year old female with DM HTN had a fall and broke her right ankle sp ORIF 2
days later in OSH
Day 4 Acute SOB on the floor with some chest pain and hypoxemia Found to
have saddle PE and was started on IV Heparin She had an ECHO which showed
Right heart strain + PFO + Atrial septal aneurysm No intracardiac thrombus
Day 5 left sided hemiparesis and profound sensory loss NIH 7 CT head is
normal CTA of the Head and Neck showed acute right carotid artery occlusion with
saddle embolus at the bifurcation extending into the ECA Transferred to CCF main
campus
Her platelets were low at presentation and HIT was suspected by vascular
medicine
Hyperacute MRI showed posterior division diffusion restriction with large penumbra
and she was taken for thrombectomy
Post procedure TICI 3 Procedure was done under Bivalirudin due to suspicion of
HIT
Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

CASE SCENARIO
75 year old female with DM HTN had a fall and broke her right ankle sp ORIF 2
days later in OSH
Day 4 Acute SOB on the floor with some chest pain and hypoxemia Found to
have saddle PE and was started on IV Heparin She had an ECHO which showed
Right heart strain + PFO + Atrial septal aneurysm No intracardiac thrombus
Day 5 left sided hemiparesis and profound sensory loss NIH 7 CT head is
normal CTA of the Head and Neck showed acute right carotid artery occlusion with
saddle embolus at the bifurcation extending into the ECA Transferred to CCF main
campus
Her platelets were low at presentation and HIT was suspected by vascular
medicine
Hyperacute MRI showed posterior division diffusion restriction with large penumbra
and she was taken for thrombectomy
Post procedure TICI 3 Procedure was done under Bivalirudin due to suspicion of
HIT
Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Day 5 left sided hemiparesis and profound sensory loss NIH 7 CT head is
normal CTA of the Head and Neck showed acute right carotid artery occlusion with
saddle embolus at the bifurcation extending into the ECA Transferred to CCF main
campus
Her platelets were low at presentation and HIT was suspected by vascular
medicine
Hyperacute MRI showed posterior division diffusion restriction with large penumbra
and she was taken for thrombectomy
Post procedure TICI 3 Procedure was done under Bivalirudin due to suspicion of
HIT
Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Hyperacute MRI
CTA Neck
MRI post IR
Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Stroke Mechanism paradoxical embolism secondary to pulmonary
hypertension with right to left shunt via PFO + Atrial septal aneurysm andor
hypercoagulable state from HIT Later her PF-4 antibodies came back
positive
Day 7 She underwent pulmonary embolectomy a day later with placement of
IVC filter as she couldnrsquot be anticoagulated due to recent stroke Still
recovering
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
PFO AND OTHER ATRIAL SEPTAL DEFECTS
DEVELOPMENT OF ATRIAL SEPTUM
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 20118
Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Mechanism - Paradoxical
embolism 9
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
TWO DIMENSIONAL TEE WITH BUBBLE CONTRAST
RA
LA
Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Calvert et al Nature Reviews Cardiology 8(3)148-60 middot February 2011
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
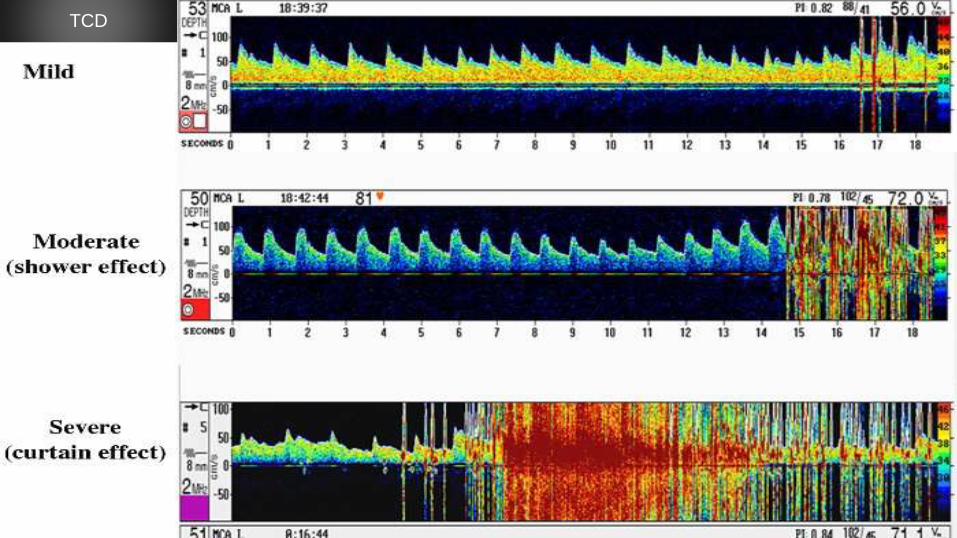
TCD
20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

20-30 of healthy
population has PFO
20-40 of acute ischemic
strokes are cryptogenic
Prevalence of PFO in
cryptogenic stroke is
around 5013
Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Risk of Paradoxical Embolism score
RoPE score
14Kent DM1 Thaler DE RoPE Study Investigators2011
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
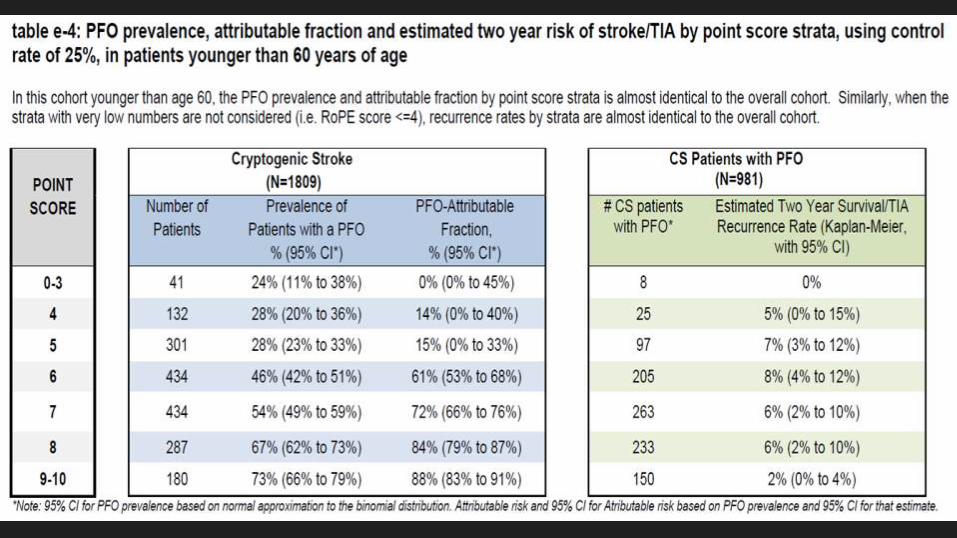
15
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
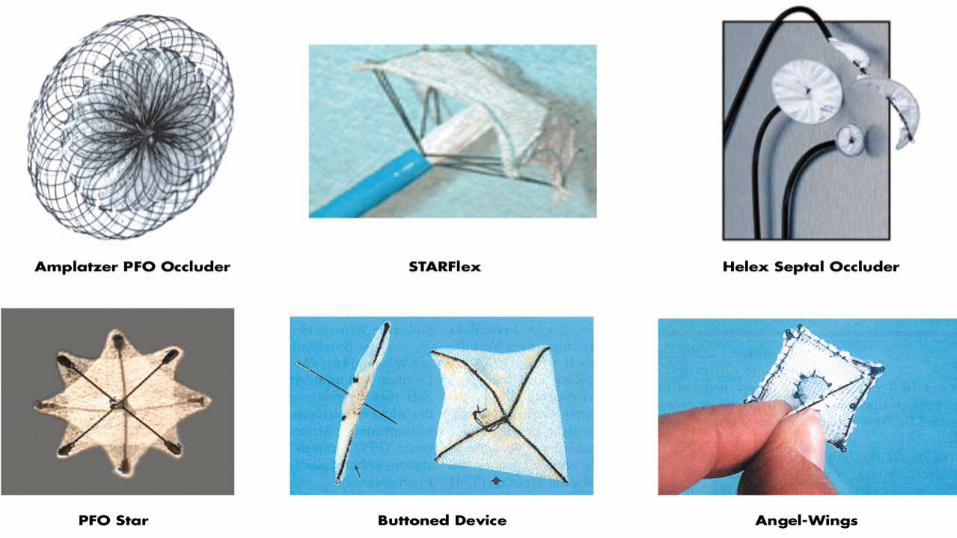
Complications
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
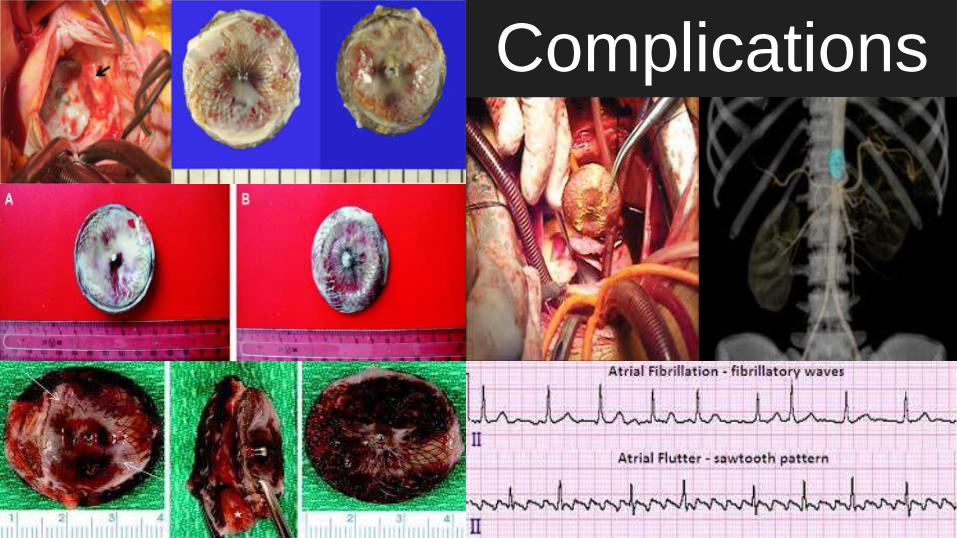
Synopsis of previous Randomized controlled trials
CLOSURE 1 (2012)Design Multicenter randomized open label trial comparing percutaneous PFO
closure Vs medical therapy alone n=909(447 vs 462) StarFLEX septal occluder
device
Follow up period 2 years
Primary Endpoints composite of Stroke TIA Death from any cause in 30 days and
death from neurological disease from 30 days to 24 months
Cumulative incidence of endpoint 55 vs 64 (adjusted hazard ratio 078 95
confidence interval 045 to 135 P=037) The respective rates were 29 and 31
for stroke (P=079) and 31 and 41 for TIA (P=044)
Conclusion In patients with cryptogenic stroke or TIA who had a patent foramen
ovale closure with a device did not offer a greater benefit than medical therapy alone
for the prevention of recurrent stroke or TIA
Anthony j Furlan et al NEJM 2012
LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

LIMITATIONS
1 Inclusion of TIA patients which is a less
precise end point
2 Very low event rates in both cohorts
3 Short follow up period
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
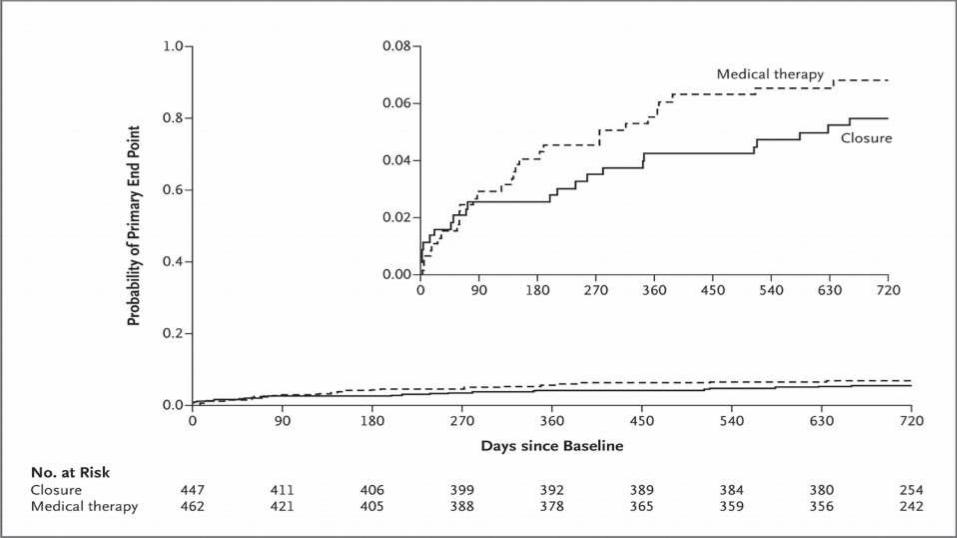
RESPECT trial 2015
Design prospective multi-center randomized event-driven trial n=980 (11
randomization 499 Vs 488) St Jude Amplatzer septal occluder device PFO closure
vs medical therapy Age range 18-60 years TIAs were excluded
Follow up period 21 years
Primary Endpoints target of 25 primary end-point events had been observed and
adjudicated Composite of nonfatal and fatal ischemic stroke early death after
randomization
Secondary efficacy endpoints complete closure of the patent foramen ovale on the
6-month follow-up TEE the absence of recurrent symptomatic nonfatal ischemic stroke
or cardiovascular death or TIA
Cumulative incidence of endpoint 9 in the closure group and 16 in the medical-
therapy group the rate of the primary end point was 066 events per 100 patient-years
in the closure group as compared with 138 events per 100 patient-years in the
medical-therapy group (hazard ratio with closure 049 95 confidence interval [CI]
022 to 111 P=008)John D Carroll MD NEJM 2013
LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

LIMITATIONS
1Differential drop out rate - inadequate exposure
to risk especially in the medical group
2Entry and retention bias in the medical group
3Duration of follow up
439 events happened in closure group occurred
after randomization and before the closure device
was placed
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
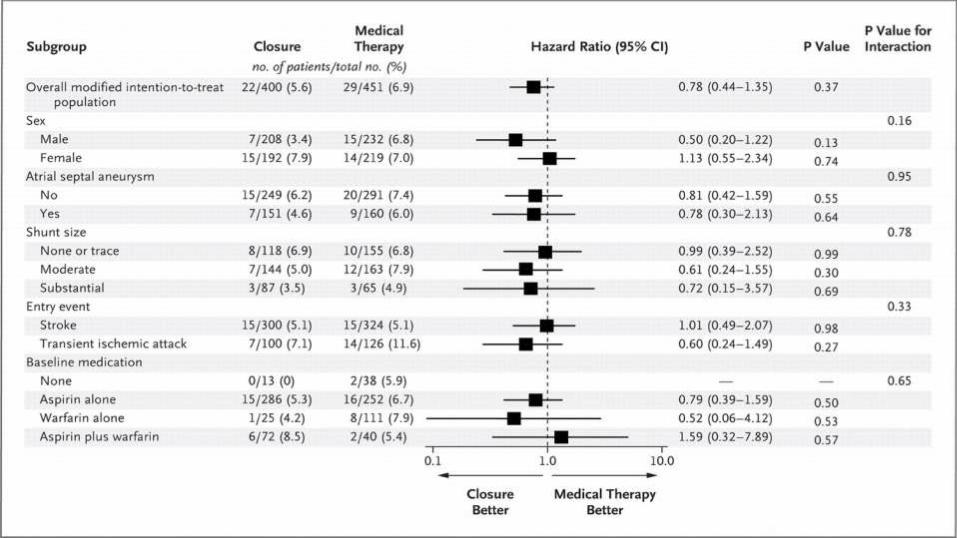
Conclusion
1 In the primary intention-to-treat analysis there was no significant benefit
associated with closure of a patent foramen ovale in adults who had had a
cryptogenic ischemic stroke
1 However closure was superior to medical therapy alone in the
prespecified per-protocol and as-treated analyses with a low rate of
associated risks
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
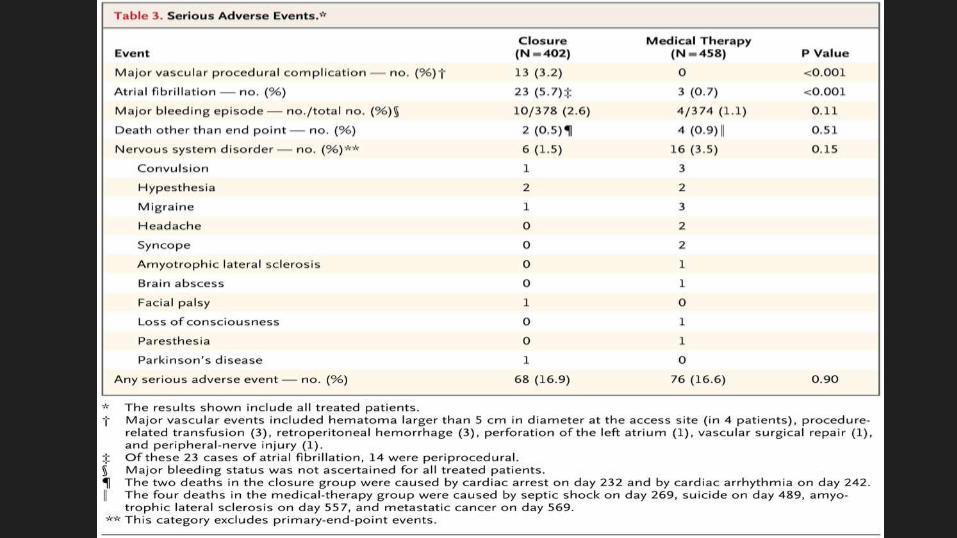
Evidence from Randomized controlled trials until 092017
Closure of PFO is not superior to antiplatelet or anticoagulation in preventing
recurrent strokeTIAPeripheral embolismDeath
CLOSURE-1 PC RESPECT trials
Guidelines from International Societies regarding cryptogenic stroke and PFO
2012 ACCP guidelines for ischemic stroke recommend antiplatelet therapy for patients with cryptogenic ischemic
stroke and a PFO and state that anticoagulation is not indicated In patients with cryptogenic stroke and DVT and a PFO these
guidelines recommend vitamin K antagonist therapy for three months
2014 AHAASA guidelines recommend antiplatelet therapy for patients with PFO and ischemic stroke or TIA who
are not undergoing anticoagulation and state that anticoagulation is indicated for patients with both a PFO and a venous
source of embolismThese guidelines conclude that available data do not support a benefit of PFO closure for patients with a
cryptogenic ischemic stroke or TIA and a PFO without evidence for DVT
2016 AAN practice advisory states that clinicians should not routinely offer percutaneous PFO closure to patients with
cryptogenic ischemic stroke outside of a research setting but may offer antiplatelet therapy instead of anticoagulation The
advisory notes that in rare circumstances such as recurrent cryptogenic stroke despite adequate medical therapy clinicians
may offer the Amplatzer PFO Occluder where available
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
New trials
30
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
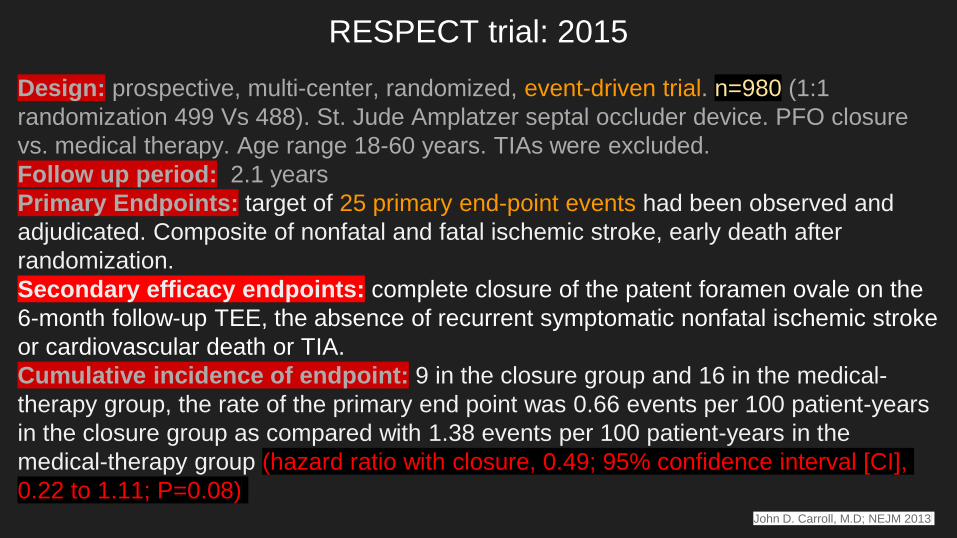
PFO CLOSURE OR ANTIPLATELET THERAPY FOR CRYPTOGENIC STROKE
Gore-REDUCE trial
Type of study multinational prospective randomized controlled open label trial
with blinded adjudication of outcome events
Period of enrollment 122008 - 022015
Total number of patients 664 (simple non stratified 21 ratio randomization into
PFO closure+APT vs APT only)
Trial endpoints 1 Freedom from clinical evidence of an ischemic stroke in 24
months(rate of recurrence of stroke)
2 Incidence of new brain infarction(Clinical and
silent)32
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
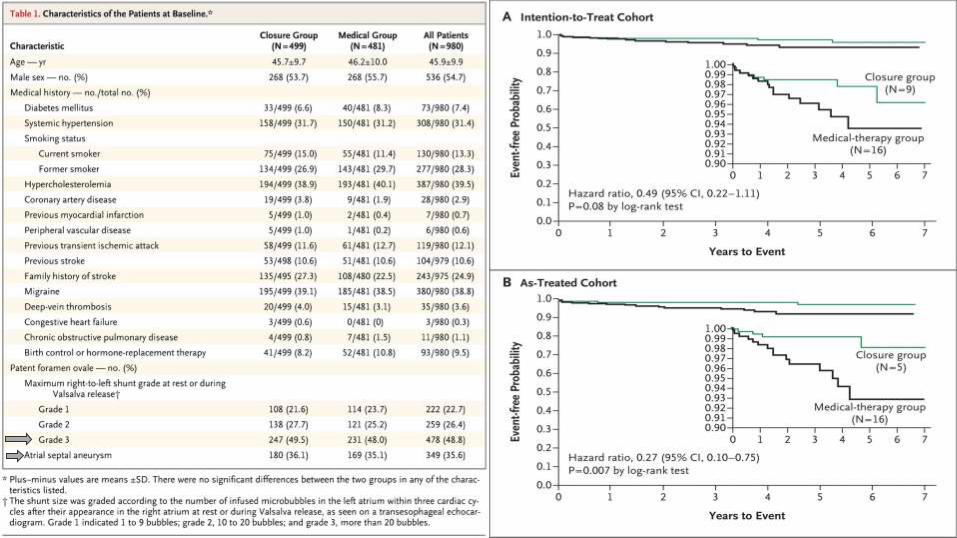
Baseline
characteristics
of patients
Not statistically different
33
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
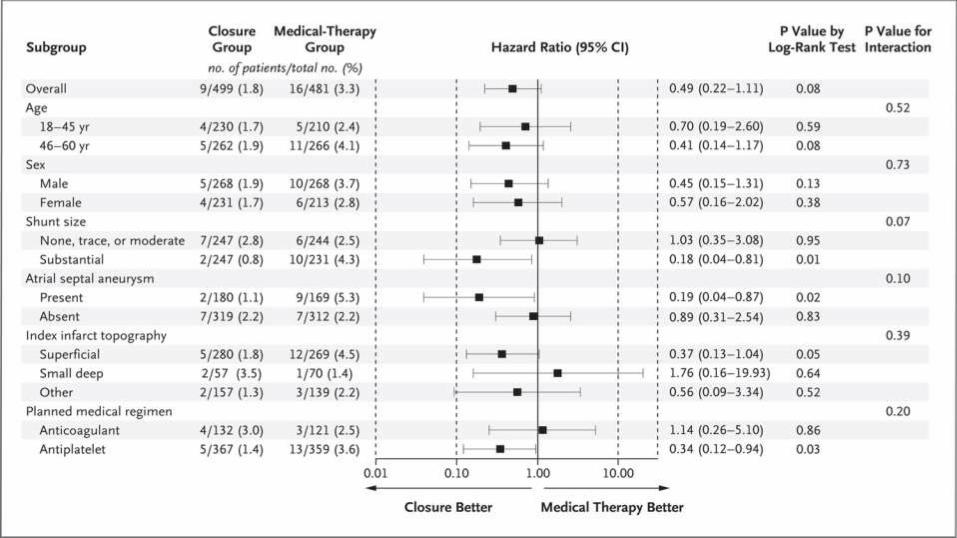
34
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
35
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
36
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
37
LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

LIMITATIONS
1 Differential dropout rates in the study groups leads to misclassification bias
2 14 patients in the medical arm underwent PFO closure outside of the trial
3 Low event rates in the two groups hampers subgroup analysis
38
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
CONCLUSIONS
Among patients with a PFO who had had a cryptogenic stroke
The risk of subsequent ischemic stroke was lower among those assigned to
PFO closure combined with antiplatelet therapy than among those assigned
to antiplatelet therapy alone however
PFO closure was associated with higher rates of device complications and
atrial fibrillation
39
40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

40
SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

SUMMARY OF CLOSE STUDY
Type of study multinational randomized open label trial 111 ratio Moderate to
large PFO with shunt +- Atrial septal aneurysm n=663
Age group 16-60
Follow up 53 +- 2
Trial endpoints 1 Occurrence of stroke
Results In the intention-to-treat cohort 0 patients in the PFO closure group Vs
14 patients in the antiplatelet-only group (hazard ratio 003 95 confidence
interval [CI] 0 to 026 Plt0001)
41
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
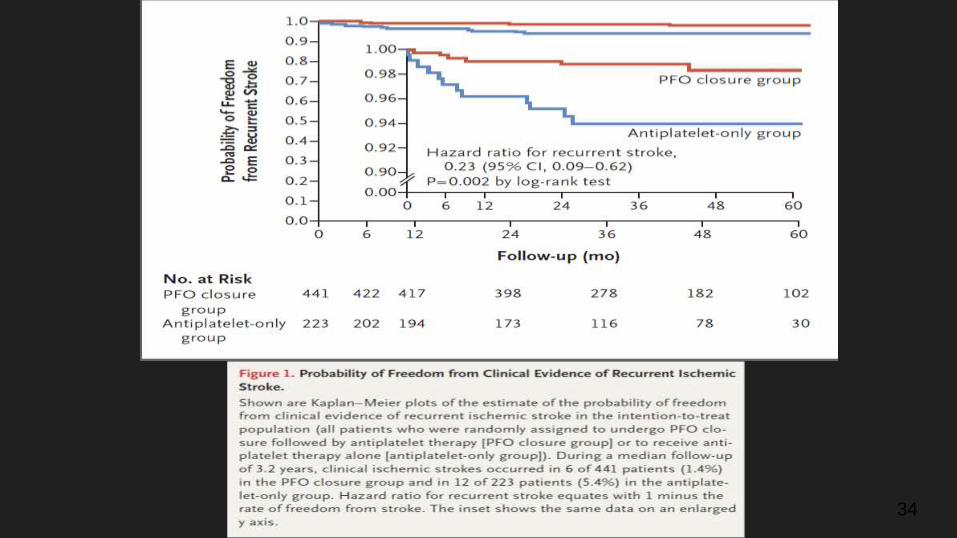
42
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
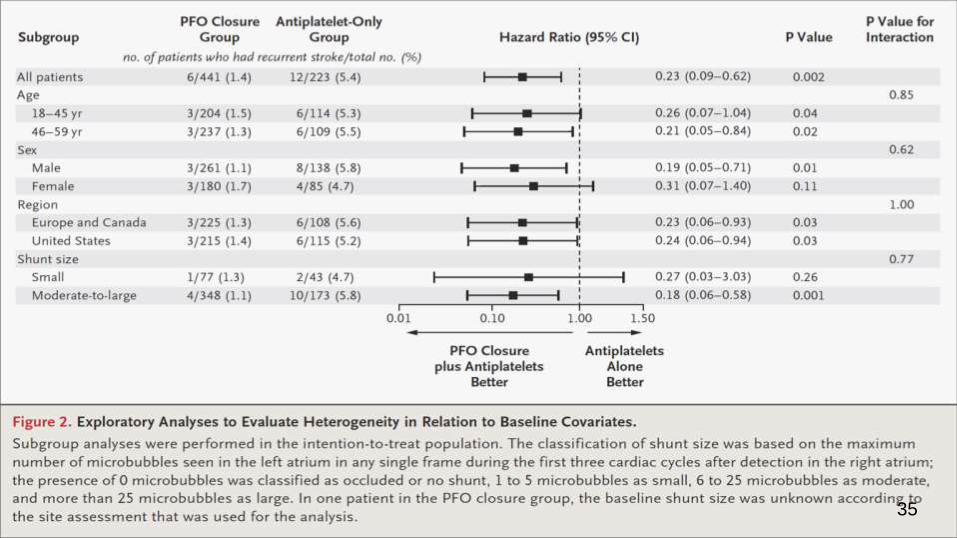
PATIENT CHARACTERISTICS
43
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
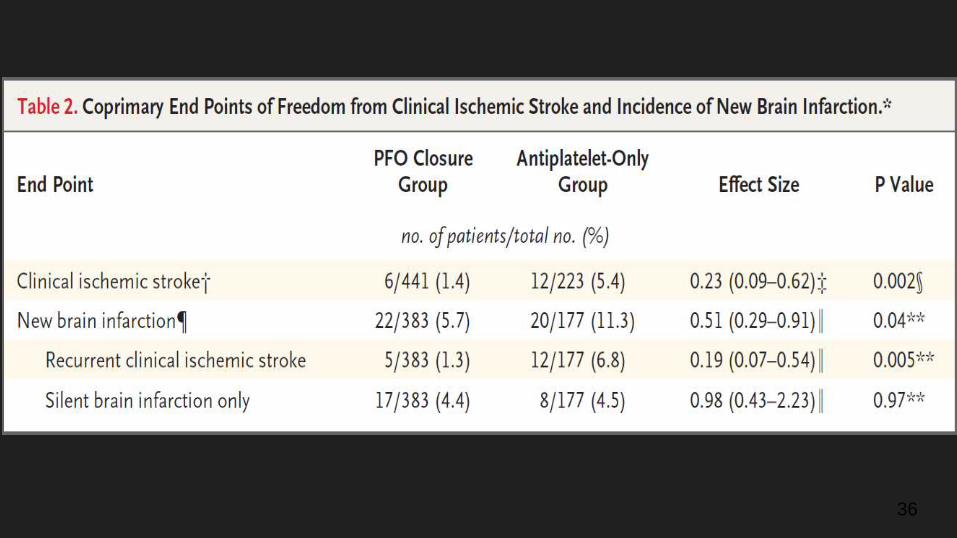
44
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
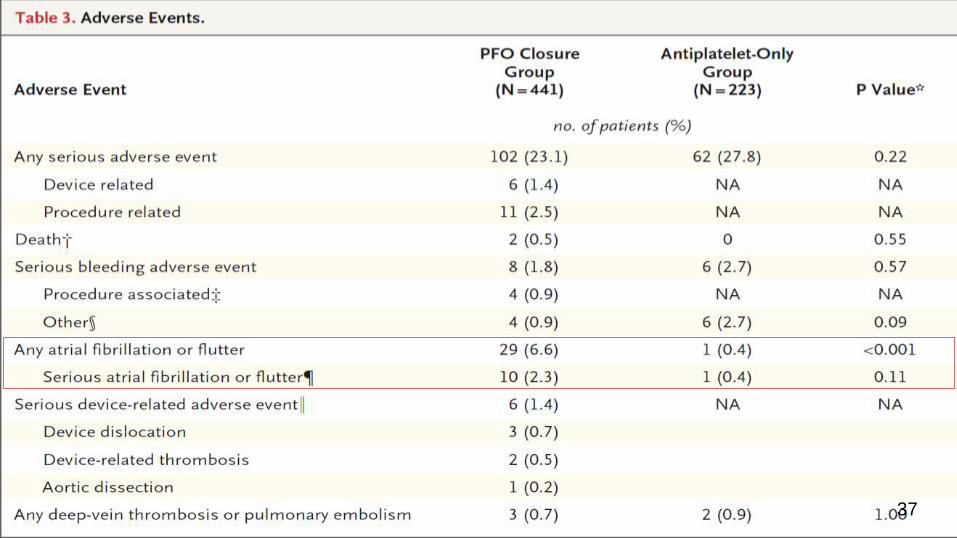
45
46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

46
Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Limitations
Lower than expected rate of enrollment
No prolonged telemetry monitoring to detect occult Afib prior to enrollment into
the study during the workup of cryptogenic stroke
47
Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

Conclusions
1 Among patients who had had a recent cryptogenic stroke attributed to PFO
with an associated atrial septal aneurysm or large interatrial shunt the
rate of stroke recurrence was lower among those assigned to PFO closure
combined with antiplatelet therapy than among those assigned to antiplatelet
therapy alone
1 PFO closure was associated with an increased risk of atrial fibrillation
48
49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

49
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
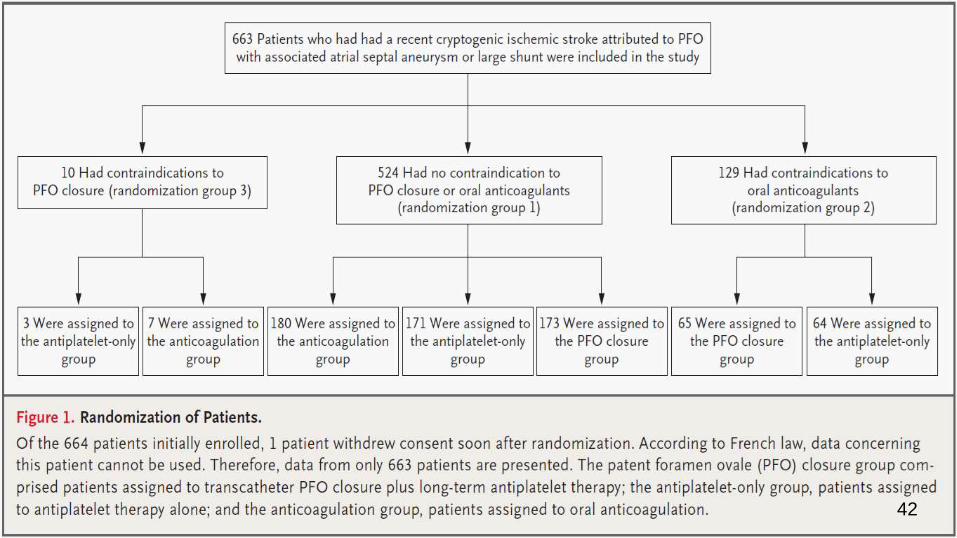
Patient
characteristics
50
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
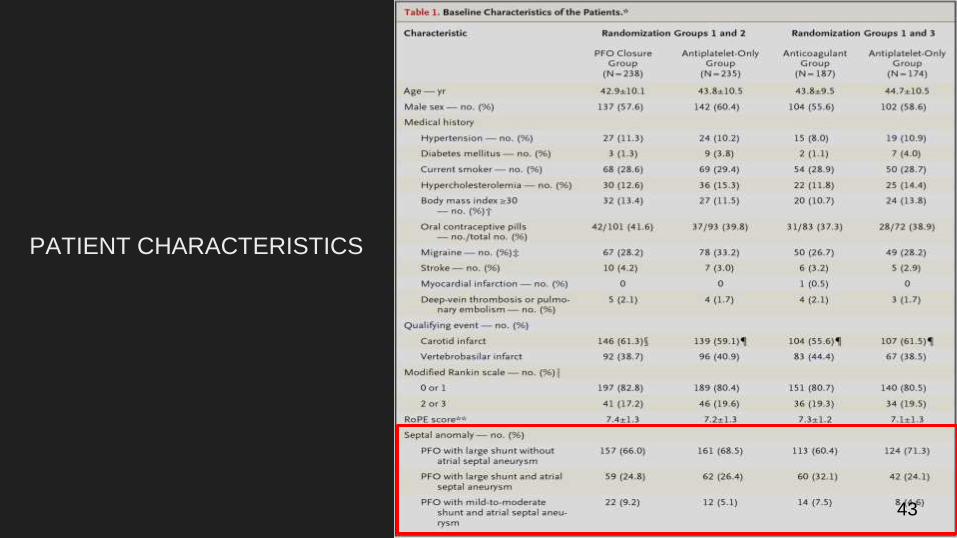
Long-term efficacy endpoints
51
52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

52
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
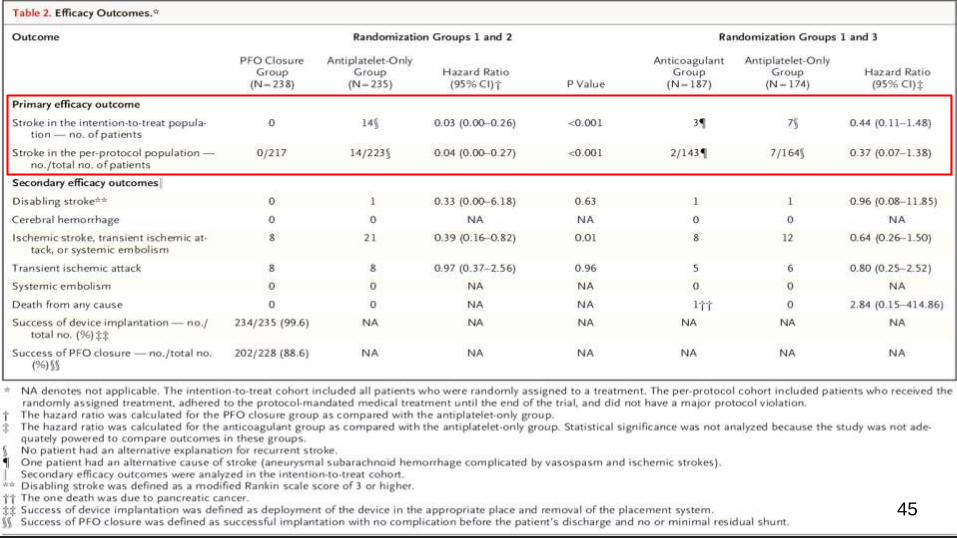
53
54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

54
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
55
CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

CONCLUSION
Among adults who had had a cryptogenic ischemic stroke closure of a PFO was
associated with a lower rate of recurrent ischemic strokes than medical therapy
alone during extended follow-up
56
57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

57
58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

58
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60
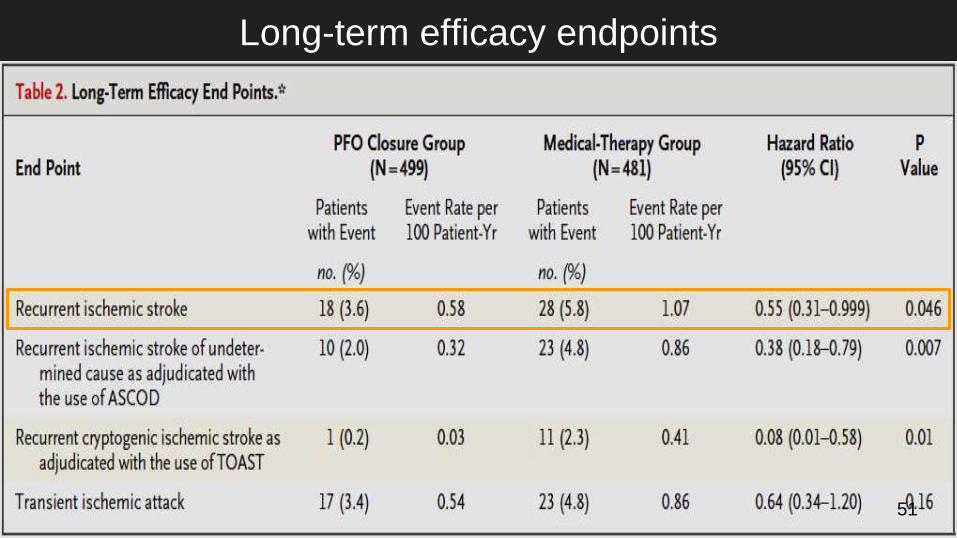
Perspectives
1 Small to moderate shunt size doesnrsquot seem to be a significant risk factor for
recurrent ischemic stroke
2 Patients with cryptogenic stroke + PFO with large R--gtL shunt with or without atrial
septal aneurysm might benefit from PFO closure + antiplatelet therapy but need
future large RCTs to confirm the findings
3 Still early to conclude that Closure is safer than medical management due to
significant perioperative complications like Afib cardiac thrombus peripheral
embolism cardiac perforation hemorrhage infection but newer closure devices
seems safer than older generation devices in terms of rate of complications and
occluding the PFO
4 Instead of leaning towards cryptogenic stroke attribution risk to PFO it might be
better to consider PFOASA characteristics along with patientrsquos age before
considering closure It is good that our understanding of Cryptogenic stroke is also
59
60

60