Embed Size (px)
Citation preview

“Life’s battles don’t go always to the stronger or faster man, sooner or later,
the man who wins is the man who thinks he can”
Aim for the Moon… even if you miss, you will Aim for the Moon… even if you miss, you will land among Stars…..!land among Stars…..!


DERMATOPATHOLOGYAcute, Chronic, Infections, Blistering, Neoplastic
Dr. Shashidhar Venkatesh MurthyAssociate Prof. & Head of Pathology

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Psoriasis,
• Chronic Eczema, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Actinic Keratosis, • Seborrheic Keratosis.
• Malignant:• BCC, SCC, Melanoma.

Normal Skin: (Thin)

Prominent granular layer
Thick Skin:

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Psoriasis,
• Chronic Eczema, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Actinic Keratosis, • Seborrheic Keratosis.
• Malignant:• BCC, SCC, Melanoma.

INFLAMMATORY disorders: Pathogenesis
Urticaria Acute Chronic LichenEczema Eczema Sclerosis
Dermal Infl Epidermal Infl Hyperplasia Hyperkeratosis
Acute Inflam. Chronic Inflam.
Ep
. Hy
pe
rpla
sia

URTICARIA (Hives)• Type I hypersensitivity – Allergy• All ages, more in 20 – 40y.• Erythematous papules and
plaques• Individual lesions are transient,
usually resolve in 24 hr, but entire episode may last for days.
• Usually on trunk and extremities.

Urticaria (Hives)

URTICARIA – Histopathology
Perivascular inflammatory infiltrate: lymphocytes, neutrophils, eosinophils.
* Note lack of spongiosis or other epidermal changes.

URTICARIA (Hives)• Follows exposure to pollens, foods,
drugs, pressure, temperature etc. • Ag IgE Mast cell
Degranulation Inflam.
• perivascular inflammatory infiltrate: lymphocytes, neutrophils or eosinophils.
• Hereditary angioneurotic edema Congenital C1 esterase inhibitor deficiency causes uncontrolled complement activation and urticaria.

Urticaria – Microscopic features
1. Superficial dermal edema (space between collagen)2. Dilated blood vessels with perivascular inflammatory cells.3. Normal Epidermis (no spongiosis or hyperplasia)
1
3
2

Acute ECZEMA – Types• Contact dermatitis• Atopic dermatitis• Drug eczema • Photoeczema• Primary irritant dermatitis
Intraepidermal edema & blister

ECZEMA dry - (atopic)

My ear is dripping on my shirt…!
• A 36y Male, 12wk rash left ear. • Spreading and becoming increasingly irritating despite twice daily applications of Kenacomb Otic ointment.
• he is otherwise in good health, with no history of serious illness, and there are no known allergies nor rashes anywhere else.
• DD: contact dermatitis, fungal infection (Tinea), Imeptigo (bact), others.
Drug induced Eczema

ECZEMA – histology
• Spongiosis (Intraepidermal) edema
• Superficial perivascular lymphocytic infiltrate

ECZEMA – pathogenesis:
Hypersensitivity Reaction:• Initial exposure to antigen:
• Antigen processed by Langerhans cells and presented to T cells in the lymph node T cell activation memory cells.
• Re-exposure to antigen:• Quick (memory T cells) response inflammation
urticaria, erythema, wet eczema
• Persistence of antigen stimulation:• Chronic inflammation Acanthosis, hyperkeratosis
(lichenification) – dry eczema.

ECZEMA (irritant)

ECZEMA (contact dermatitis)

ERYTHEMA MULTIFORME:
• Self limited Hypersensitivity response to,• Infections: herpes simplex, Mycoplasma • Drugs: sulfonamides, penicillin barbiturates• Malignancy: carcinoma, lymphoma• Auto Immune dis: SLE, SS, dermatomyositis
• Multiple forms - papules, plaques, nodules, blisters, ulcers etc..
• Characteristic “targetoid” lesions. • Central grey necrosis, Erythematous raised border.
• Mild to severe forms – spectrum • EM Minor, EM Major, Stevens-Johnsons
syndrome and toxic epidermal necrolysis.

ERYTHEMA MULTIFORME
Target Lesions

ERYTHEMA MULTIFORME - Microscopy
• Necrotic keratinocytes
• Spongiosis (edema)
• Epidermal lymphocytes
• Superficial perivascular lymphocytes
Note: destruction of basal epidermal layer.

Stevens-Johnson Sy.(EM major)
• A 2y black male, who was started on Phenobarbital after his third febrile seizure. Seven days later, he developed erythematous lesions over his extremities, hands, face and trunk with high fever. Bullae, Erosion and crusting of mucosal surfaces.
• May be caused by other drugs, infections, histology same as EM.

Toxic Epidermal Necrolysis (TENs):• Larger body surface
involvement (>40%)• Development of bullae &
peeling of epidermis in sheets >3 cm & the skin becomes tender within 48 hours.
• Extensive basal layer degeneration.
• Serious complication of EM Major & TENs is conjunctival damage resulting in corneal drying and opacification (blindness).

"The gem cannot be polished without friction, nor man perfected without trials or problems (or exams)…!."
--Chinese proverb

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Chronic Eczema,
• Psoriasis, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Actinic Keratosis, • Seborrheic Keratosis.
• Malignant:• BCC, SCC, Melanoma.

PSORIASIS - pathophysiology
• Multifactorial: genetic and immune• strong association HLA-C (w 0602 allele)⋆ • Sensitized T cells infiltrate the skin and
secrete cytokines and growth factors• Inflammation, Increased cell turnover• Vascular proliferation angiogenesis• Trauma precipitates lesions – Koebner phen.
• Multi system disorder:• Arthritis, myopathy, enteropathy, Immunodef.

PSORIASIS - clinical• Chronic, recurrent elbows, knee, scalp• well-demarcated, pink plaque covered with loosely
adherent silvery scales.• Removal of scales point bleeds – Auspitz sign.

PSORIASIS
CLINICAL:•Pink Plaques•Silvery scales.•Koebner Phenomenon•Auspitz sign•Arthritis.

PSORIASIS – Nail changes
• “Oil-slick” nail discoloration• Nail pitting• Onycholysis

PSORIASIS – Arthritis.

Psoriasis: Histopathology
Acanthosis, Parakeratosis, neutrophilic microabscesses.

PSORIASIS - histology
Parakeratosis
Diminished granular layer
Regular elongation of the rete ridges
Tortuous papillary dermal vessels
neutrophil abscess in epidermis

Lichen Planus:• Pruritic, Purple, Polygonal, Planar,
Papules and Plaques.• Skin & mucosa. Genitals, oral, • Self limited. 1-2 years.• Basal layer, Interface dermatitis.• Degenration, Squamatization• Anucleate dead epidermal cells in
basal layer – Civatte bodies.• Similar to EM but chronic with
hyperplasia, hyperkeratosis(scaling).

Lichen Planus:
Mucosal involvement

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Chronic Eczema,
• Psoriasis, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Actinic Keratosis, • Seborrheic Keratosis.
• Malignant:• BCC, SCC, Melanoma.

Impetigo: Bacterial Infection
• Staph or Strep• Superficial, Bacterial• Oozing & crusting.• Spongiosis• Neutrophils.

Impetigo:
Epithelium
Ulcer + Inflam

Acne: Acne: Pathogenesis
• Inflammation of pilosebaceous units • Interplay of four factors• Excessive sebum - sebaceoussebaceous glandgland
hyperplasiahyperplasia • HyperkeratinizationHyperkeratinization – Microcomedo -
Obstruct pores.• Lipids and cellular debris accumulate
within the blocked follicle. • Colonization of PropionibacteriumPropionibacterium acnes acnes
(+ secondary infection)• InflammationInflammation is further enhanced by
follicular rupture and subsequent leakage of lipids, bacteria, and fatty acids into the dermis.

Acne: Hair fol. infection:
Neutrophil Abscess
Hair Follicle (infected)
Hair Follicle (infected)Block sebum infectionHarmonal, excess/drying/oily
Comedo

BacterialSkin Infections:
Types

Viral Infections:• Human papillomavirus: Warts (verrucae)
• Keratotic(hard) & condyloma (fleshy)
• Molluscum contagiosum:• Herpes – Zoster & Shingles.• HIV – Kaposi sarcoma (HHV 8)

Verruca Plana:
•HPV-3 or 10•Face, young, flat •Small, hyperkeratotic•Koilocytic keratinocytes.

Palmoplantar warts: Myrmecia
•HPV-3 or 10•Sole & Palms •Intradermal hard cyst.•Inward growth•Koilocytic keratinocytes.

Condyloma accuminatum:• HPV-6, Genital warts• Fleshy growths• Acanthosis, papillomatosis• Koilocytes- perinuclear
halo. – viral inclusions.
Pap Smear
Cervical Biopsy

Molluscum contagiosum:• DNA pox virus • Grouped pearly hypopigmented
flask like papules with central cupped scaly centre (arrow A).
• Pink cytoplasmic viral inclusions “Molluscum body” (arrow B)
B A

Fungal: Tineasis• Ring worm, Round, scaly, itchy
dermatitis – Trichophyton sp• Spreading out with Central clearing.• Lab: Scrapings in KOH solution
• Tinea cruris.• Tinea capitis• Tinea versicolor – pale macules – • Pityrosporum.
Fungus
Fungus

Case Study: Painful, Itchy vesicles:• A 32y man, itchy and painful
rash on the back of his left leg • About 7 days ago, he began to
feel an “intense itching & burning pain” behind his left knee.
• “small blisters” began to “pop up” over the area.
• Not responding to antibiotic ointment and acetaminophen (Tylenol).
? likely diagnosis?
*Intense, burning pain & blisters along nerve distribution
Cutaneous Herpes - Shingles.

“The worst thing in your life may contain seeds of the best. When you can
see crisis as an opportunity, your life becomes not only easier, but more
satisfying.”
–Joe Kogel

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Chronic Eczema,
• Psoriasis, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Actinic Keratosis, • Seborrheic Keratosis.
• Malignant:• BCC, SCC, Melanoma.

BLISTERING DISEASES
• Subcornial.• Suprabasal.• Subepidermal.
PEMPIGUS FOLIACESOUS PEMPIGUS VULGARIS BULLOUS PEMPHIGOID

BLISTERING DISEASES• Pemphigus :
• vulgaris most common (80%) other variants (vegetans, foliaceus, erythematosus) are rare
• 40-60y, mucosa & skin.• scalp, face, axilla, groin, trunk.• Autoimmune, IgG against desmosomes. • acantholysis, intraepidermal blister, loose cells inside bulla.
• Bullous pemphigoid:• Elderly, Autoimmune (subepidermal Anchoring proteins).• thighs, flexor surface of forearms, axilla, groin, 30% oral.• Large, Tense, Subepidermal bullae, no acantholysis.
• Dermatitis Herpetiformis:• Rare, very itchy small papules, vesicles, occassional bullae.
Males, associated with celiac disease (gluten sensitivity).

Pemphigus vulgaris

Pemphigus vulgaris
• Gross: Axilla, flaccid, erythematous base, easy rupture, crusted ulcers.
• Microscopy: intraepidermal location. Loose acantholytic cells inside.

Acanthocytes - Acantholysis:

PEMPHIGUS – Immunoflourescence
Deposition of immunoglobulin and complement along keratinocyte membranes giving a “fish net” appearance



PEMPHIGUS• Four variants: P. vulgaris – most common

Intraepidermal bulla:

BLISTERING DISEASES• Pemphigus :
• vulgaris most common (80%) other variants (vegetans, foliaceus, erythematosus) are rare
• 40-60y, mucosa & skin.• scalp, face, axilla, groin, trunk.• Autoimmune, IgG against desmosomes. • acantholysis, intraepidermal blister, loose cells inside bulla.
• Bullous pemphigoid:• Elderly, Autoimmune (subepidermal Anchoring proteins).• thighs, flexor surface of forearms, axilla, groin, 30% oral.• Large, Tense, Subepidermal bullae, no acantholysis.
• Dermatitis Herpetiformis:• Rare, very itchy small papules, vesicles, occassional bullae.
Males, associated with celiac disease (gluten sensitivity).

BULLOUS PEMPHIGOID• Tense large bulla• Intact epithelium.

BULLOUS PEMPHIGOID
82 year old nursing home, dementia, gastrostomy tube, treated for urinary tract infection

BULLOUS PEMPHIGOID
Hemorrhagic blisters annular arrangement in bullous pemphigoid

BULLOUS PEMPHIGOIDAntibody against bullous pemphigoid antigen in basement membrane causing subepidermal separation Type II hypersensitivity reaction.

BULLOUS PEMPHIGOID
Eosinophils at the DE junction.
Subepidermal bulla

BULLOUS PEMPHIGOID - histology
Subepidermal blister
Inflammation characterized by eosinophils
Intact acanthocytic layer.

BLISTERING DISEASES• Pemphigus :
• vulgaris most common (80%) other variants (vegetans, foliaceus, erythematosus) are rare
• 40-60y, mucosa & skin.• scalp, face, axilla, groin, trunk.• Autoimmune, IgG against desmosomes. • acantholysis, intraepidermal blister, loose cells inside bulla.
• Bullous pemphigoid:• Elderly, Autoimmune (subepidermal Anchoring proteins).• thighs, flexor surface of forearms, axilla, groin, 30% oral.• Large, Tense, Subepidermal bullae, no acantholysis.
• Dermatitis Herpetiformis:• Rare, very itchy small papules, vesicles, occassional bullae.
Males, associated with celiac disease (gluten sensitivity).

Dermatitis Herpetiformis
• Extremely pruritic, small vesicles• Associated with Celiac disease.• IgA Anti-gluten Ab cross react with
basement membrane proteins.
• Microabscess – papillae• Subepidermal blister.• Granular IgA deposits.

Dermatitis Herpetiformis:
• Gross: Intense Itchy, small, erythematous, pappules, small blisters in groups. (sub epithelial)
• Micro: supepidermal, neutrophilic microabscesses in dermal papilla.

PEMPHIGUSPEMPHIGUS PEMPHIGOIDPEMPHIGOID DHDH
age mid - older elderly 30-40
antibody IgG IgG IgA
location Suprabasilar Subepidermal subepidermal
inflammation
mixed eosinophils neutrophils
Site of dysfunctio
nDesmosomes
Basement membrane and
hemidesmosomes
Anchoring fibrils
Antibody against:
DesmogleinBullous
pemphigoid antigen
reticulin
Immuno “fish net” Linear basement
membraneDermal tip

"When you speak, speak the truth; perform when you promise; discharge your trust... Withhold your hands from striking, and from taking that which is unlawful and bad...“ - - APJ Abdul Kalam, President of India.

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Chronic Eczema,
• Psoriasis, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Seborrheic Keratosis.• Actinic Keratosis,
• Malignant:• SCC, BCC, Melanoma.

Skin Tumours Incidence:
• Most Common: (no count, ?disease ….! )• Moles, Nevi, Freckles, • Skin Tags & Cherry angioma
• Common:• Benign: Warts, Seborrheic & Actinic keratosis,.. • Malignant: Carcinoma (Basal, Sq, Melanoma)
• Rare: (less but not uncommon..!)• Many… Epithelial, adnexal, con. tissue, others.• Adenoma, fibroma, lipoma, cylindroma… etc..

Benign: Nevus/nevi:
• Commonest *• Congenital / after birth• Stable, permanent.• Uniform, symmetrical
suggest benign.• Irregular, varying
color or growth - malignancy.
• Rarely grow.• Changes suggest
malignant transformation (rare).

Nevi types & Pathology:

Junctional Nevus:• Small, flat, symmetric, uniform lesions.• Cluster of melanocytes at DE junction. (arrow)

Compound Nevus:
• Small, raised, dome shaped, symmetric, uniform.• Cluster of melanocytes in dermis & DE junction.
(arrow)

Dysplastic Nevus:1.Pigmented raised lesion with central darker shade (arrow).2.Junctional cluster of irregular melanocytes (arrow)
1
2

Progression of dysplastic nevus:
A. Lentiginous melanocytic hyperplasia. B. Lentiginous junctional nevus. C. Lentiginous compound dysplastic nevus D. Early melanoma, E. Advanced melanoma (vertical growth)
MelanomaNevus

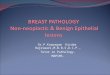
SEBORRHEIC KERATOSIS• Very common in elderly, Face.• Round, flat, velvety plaques, • ?arrest in epidermal maturation.• May be pigmented, Appear
“stuck on” skin.• Treatment only if inflammed.• Sudden crop of lesions occur in
internal cancers (Sign of Leser-Trelat)
• No malignant potential.

SEBORRHEIC KERATOSIS

SEBORRHEIC KERATOSIS

Seborrheic Keratosis:

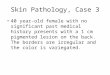
Seborrheic Keratoses: Microscopy
• Thick hyperplastic epidermis above the surrounding level.
• Keratin cysts
1
2

Seborrheic Keratoses:Exophytic (outward) growth of Epidermal hyperplasia

ACTINIC KERATOSIS• Aged, sun exposure areas.• Red or tan, Irregular, scaly plaques • Pre-cancerous skin growth• Sun-exposed skin• Hyperkeratosis • Inflammation• ulceration• Crusting• Dysplasia• Premalignant

Actinic Keratosis
• Lymphoid infiltrate
• Epithelial atypia.• Hyperkeratosis,
parakeratosis• Sun damaged
dermis - Solar elastosis.

ACTINIC KERATOSIS - histology
Parakeratosis
Atrophy
Basilar atypia

ACTINIC KERATOSIS - histology
Parakeratosis, atypical basal layer, solar elastosis
Note: atypical cells “spare” hair follicle epithelium.

Actinic Keratosis – Horn / Ca.

"Thinking is progress. Non-thinking is stagnation of the individual, organisation and the country. Thinking leads to right action. Knowledge without action is useless and irrelevant. Knowledge with action, converts adversity into prosperity.”- - APJ Abdul Kalam, President of India.

SQUAMOUS CELL CARCINOMA
• Common cancer on sun-exposed skin in older people.• Industrial carcinogens• Arsenic, tobacco, Beetle
nut chewing.• UV, Ionizing radiation
• Squamous epithelial cells
• Microscopy: dyskeratosis. Epithelial pearls –
Keratin Pearl

SQUAMOUS CELL CARCINOMA

Epithelial (Keratin) pearl in SCC:
Keratinized – ep. pearl
Dysplastic ep. cells

BASAL CELL CARCINOMA
• Relatively common• Slow growing• Rarely metastasize• Occur on sun-exposed
skin• Pearly papule with
telangectasia• Large tumors may
ulcerate (rodent ulcer)

Basal Cell Carcinoma:Type •Features Picture
Nodular BCC •Most common •Small, shiny, pink lump •Prominent BV network.
Superficial BCC •Often multiple •Pink or red scaly irregular plaques
Morphoeic BCC •sclerosing BCC •scar-like •(perineural spread)
Pigmented BCC •Brown, blue or grey•Like melanoma •Nodular or superficial
Basisquamous BCC •Mixed BCC & SCC •more aggressive

Gross appearance:
• Round, nodular, pearly/shiny.
• Prominent blood vessels over the tumor.
• Shiny Crust over the lesion.

BASAL CELL CARCINOMA
• Note central ulcer & prominent blood vessels around.

BASAL CELL CARCINOMA

Basal Cell Carcinoma:
Squamous cells (malignant) extending deep breaking through basement membrane
Squamous eddies or “ep. pearls”

BASAL CELL CARCINOMA

BASAL CELL CARCINOMA
Cords and islands of basaloid cells
Hyperchromatic nuclei
Peripheral palisading
Clefting between tumor and stroma
Mucinous stroma

Melanoma:
• Nests of atypical melanocytes
• Melanin pigment.
• Mitotic figure.

Melanoma Clinical Features: note ABCD..

Melanoma Types:
• Lentigenous: Flat superficial basal layer – sun damage.
• Superficial Spreading: Early stage. Upper layers. Commonest.
• Nodular: Tumor growing deep. advanced (all types)
• Acral – Palm/sole, lentigenous or nodular.
• Subungual: Nail bed, nodular.

Melanoma :

Melanoma :
ABCD..
Multiple Nevi one of them changing recently Melanoma

Melanoma Types:Nodular Melanotic ↓ Nodular Amelanotic
Lentigo
Nodular

Melanoma : Histopathology
Tumor cells extend from epidermis to invade the dermis. Focal brown melanin pigment in some tumor cells.

Melanoma : Histopathology
• Clusters of malignant cells. Clear cytoplasm. Large pleomorphic nucleus.
• focal melanin pigmentation.

Melanoma : Histopathology• Tumor in
dermis.• focal
melanin pigmentation.
• Inflammatory cells around.

Melanoma Staging: Clark’s levels

"If you always put limit on everything you do, physical or anything else it will spread into your
work and into your life. There are no limits. There are only plateaus, and you must not stay there, you
must go beyond them."
- - Bruce Lee1940-1973, Martial Artist and Actor

Dermatopathology: MD3020 curriculum1. Acute Inflammations:
• Urticaria, • Acute Eczema, • Erythema Multiforme.
2. Chronic Inflammations:
• Chronic Eczema,
• Psoriasis, • Lichen planus.
3. Infections• Bacterial (Impetigo), • Fungal(tinea) &
• Viral(warts).
1. Blistering Diseases• Pemphigus, • Pemphigoid, • Dermatitis herpetiformis.
5. Neoplastic:
• Benign:
• Nevi, • Seborrheic Keratosis.• Actinic Keratosis,
• Malignant:• SCC, BCC, Melanoma.

Psychodermatosis

Study Tips:• Preparation:
• Read Lecture notes, attend lecture*.• Read Robbins Pathology (Basic).• “Study Images” Gross & Microscopic.
• Make short notes for each condition,• List 3* clinical features.• Etiology, Pathogenesis• List 3* gross features.• List 3* microscopic features.
• Self Assessment:• Case studies.• Questions & Answers.
Test your commitment, Get ready for Exam tomorrow.....!

“Fixing your goal is like identifying the North Star. You sight your compass on it and then use it as the means of getting back on track when you tend to stray”--Marshall Dimock
1. What I want to be? Am I going there? 2. What is the best use of my time right now?
Stick this on the wall in your room... !