Embed Size (px)
DESCRIPTION
prepared by M.D., PhD Marta R. Gerasymchuk Department of Pathophysiology Ivano-Frankivsk National Medical University
Citation preview

Ivano-Frankivsk Ivano-Frankivsk National Medical National Medical
UniversityUniversity

1.1. Regulation of lipid Regulation of lipid metabolism.metabolism.
2.2. Classes of lipoproteins.Classes of lipoproteins.
3.3. Hyperlipidemias.Hyperlipidemias.
4.4. Atherosclerosis.Atherosclerosis.
5.5. Complications of Complications of atherosclerosis.atherosclerosis.
6.6. ObesityObesity
7.7. Genetic disordersGenetic disorders
8.8. Fat-soluble Fat-soluble
vitaminsvitamins

The knowledge of the reasons The knowledge of the reasons and mechanisms of atherosclerosis and mechanisms of atherosclerosis development is necessary for the development is necessary for the doctors of various profession for doctors of various profession for prophylaxis and treatment of this prophylaxis and treatment of this disease. disease.
According to modern notions, According to modern notions, main etiological factors of main etiological factors of atherosclerosis is dyslipoproteinemia atherosclerosis is dyslipoproteinemia and increased permeability arterial and increased permeability arterial wall for lipoproteins. wall for lipoproteins.
Atherosclerosis Atherosclerosis – exceptionally widespread disease. On data WHO, – exceptionally widespread disease. On data WHO, mortality of the patients in the age 35-44 years for damages of heart and mortality of the patients in the age 35-44 years for damages of heart and vessels connected with atherosclerosis, increased lately by 60%. vessels connected with atherosclerosis, increased lately by 60%.

Metabolic Rate -Metabolic Rate - tthe amount of energy liberated per unit of time.
The amount of energy liberated by the catabolism of food in the body is the same as the amount liberated when food is burned outside the body.
The energy liberated by catabolic processes in the body is used for maintaining body functions, digesting and metabolizing food, thermoregulation, and physical activity. It appears as external work, heat, and energy storage:
= + + Isotonic muscle contractions perform work at a peak efficiency approximating 50%:
= /
CaloriesCalories The standard The standard unit of heat energyunit of heat energy is the is the calorie (cal)calorie (cal),, defined as the defined as the amount of heat energy necessary to raise amount of heat energy necessary to raise the temperature of 1 g of water 1 degree, from 15 °C to 16 °Cthe temperature of 1 g of water 1 degree, from 15 °C to 16 °C. This unit is also called the gram calorie, small . This unit is also called the gram calorie, small calorie, or standard calorie. The unit commonly used in physiology and medicine is the calorie, or standard calorie. The unit commonly used in physiology and medicine is the Calorie (Calorie (kilocalorie; kilocalorie; kcalkcal),), which which equals 1000 cal. equals 1000 cal.
ENERGY ENERGY OUTPUTOUTPUT
EXTERNAL EXTERNAL WORKWORK
ENERGY ENERGY STORAGESTORAGE
HEATHEAT
WORK WORK DONEDONE
TOTAL ENERGY TOTAL ENERGY EXPENDEDEXPENDED
EFFICIENCYEFFICIENCY

Measuring the Metabolic RateMeasuring the Metabolic Rate • In determining the metabolic rate, OIn determining the metabolic rate, O22
consumption is usually measured with consumption is usually measured with some form of oxygen-filled spirometer and some form of oxygen-filled spirometer and a COa CO22-absorbing system. -absorbing system.
• The spirometer bell is connected to a pen The spirometer bell is connected to a pen that writes on a rotating drum as the bell that writes on a rotating drum as the bell moves up and down. The slope of a line moves up and down. The slope of a line joining the ends of each of the spirometer joining the ends of each of the spirometer excursions is proportionate to the Oexcursions is proportionate to the O22
consumption. consumption.
• The amount of OThe amount of O22 (in milliliters) consumed (in milliliters) consumed
per unit of time is corrected to standard per unit of time is corrected to standard temperature and pressure and then temperature and pressure and then converted to energy production by converted to energy production by multiplying by 4.82 kcal/L of Omultiplying by 4.82 kcal/L of O22 consumed. consumed.

• The metabolic rate determined at rest in a room at a The metabolic rate determined at rest in a room at a comfortable temperature in the thermoneutral zone 12-14 hours comfortable temperature in the thermoneutral zone 12-14 hours after the last meal is called the after the last meal is called the basal metabolic rate (BMR).basal metabolic rate (BMR).
• This This value falls about 10% during sleepvalue falls about 10% during sleep and up to and up to 40% 40% during prolonged starvationduring prolonged starvation. The rate during normal daytime . The rate during normal daytime activities is, of course, higher than the BMR because of activities is, of course, higher than the BMR because of muscular activity and food intake. muscular activity and food intake.
• The The maximum metabolic ratemaximum metabolic rate reached during exercise is often reached during exercise is often said to be ten times the BMR, but trained athletes can increase said to be ten times the BMR, but trained athletes can increase their metabolic rate as much as 20-fold. their metabolic rate as much as 20-fold.
• The BMR of a man of average size is about 2000 kcal/d. The BMR of a man of average size is about 2000 kcal/d.

LipidsLipids
Fatty acids Fatty acids and their and their
derivativesderivatives
SaturatedSaturated (no double (no double
bonds)bonds)
Sterols (Sterols (steroid hormones & cholesterol))
Phospholipids Phospholipids and related and related compoundscompounds
Neutral fats Neutral fats (triglyceride(triglyceride
s)s)
UnsaturatedUnsaturated (dehydrogenated, (dehydrogenated, with various numbers of double with various numbers of double
bonds)bonds)

Lipoprotein
Composition (%)
Size(nm)
ProteinFree
CholesterolCholesteryl
EstersTriglyceride Phospholipid Origin
ChylomicronsChylomicrons75-
10002 2 3 90 3 Intestine
Chylomicron Chylomicron
remnantsremnants30-80 . . . . . . . . . . . . . . . Capillaries
Very low Very low
density density
lipoproteins lipoproteins
(VLDL)(VLDL)
30-80 8 4 16 55 17Liver and intestine
Intermediate-Intermediate-
density density
lipoproteins lipoproteins
(IDL)(IDL)
25-40 10 5 25 40 20 VLDL
Low-density Low-density
lipoproteins lipoproteins
(LDL)(LDL)20 20 7 46 6 21 IDL
High-density High-density
lipoproteins lipoproteins
(HDL)(HDL)7.5-10 50 4 16 5 25
Liver and intestine

Transports diet-derived triglyceride (TG) in the blood
Composition:
(1) Protein (2%); (2) TG (87%); (3) Cholesterol (CH;3%); (4) Phospholipid (8%)
Synthesized in intestinal epithelium
(1) Requires apolipoprotein (apo) B-48 for assembly and secretion
(2) Nascent chylomicrons in the circulation obtain apo C-Il and apo E from high density lipoprotein (HDL)
Absent during fasting
If increased, it forms a creamy supranate.• 1) Test tube must be left upright in a refrigerator overnight,• 2) Chylomicron floats on top of plasma because it has very little protein (low
density).
Source of fatty acids and glycerol
• Used to synthesize TG in the liver and adipose
Hydrolysis by capillary lipoprotein lipase (CPL) leaves a chylomicron remnant,
• Chylomicron remnants arc removed by apo E receptors in the liver.

Lipoprotein Functions Apoproteins Functions
Chylomicrons
Transport dietary triglyceride and cholesterol from intestine to tissues
apoB-48apoC-IIapoE
Secreted by intestineActivates lipoprotein lipaseUptake of remnants by the liver
VLDL
Transports triglyceride from liver to tissues
apoB-100apoC-IIapoE
Secreted by liverActivates lipoprotein lipaseUptake of remnants (IDL) by liver
IDL(VLDL remnants)
Picks up cholesterol from HDL to become LDLPicked up by liver
apoEapoB-100
Uptake by liver
LDLDelivers cholesterol into cells ApoB-100 Uptake by liver and other
tissues via LDL receptor (apoB-100 receptor)
HDL
Picks up cholesterol accumulating in blood vesselsDelivers cholesterol to liver and steroidogenic tissues via scavenger receptor (SR-B1)Shuttles apoC-II and apoE in blood
apoA-1 Activates lecithin cholesterol acyltransferase (LCAT) to produce cholesterol esters

Transports liver-synthesized TG in the blood- Requires apolipoprotein B-100 for assembly and secretion
Composition:• (1) Protein (9%); (2) TG (55%); (3) CH (17%); (4) Phospholipid (19%).
Source of fatty acids and glycerol• 1) Used to synthesize TG in the adipose tissue• 2) Hydrolysis by CPL produces intermediate-density lipoprotein (IDL) and low density lipoprotein (LDL).• 3) Some of the IDL is removed from blood by apo E receptors in the liver.
Cholesterol ester transport protein (CETP)
(1) Transfers CH from HDL to VLDL;
(2) Transfers TG from VLDL to HDL;
(3) An increase in VLDL always causes a decrease in HDL-CH.
If increased, it forms a creamy infranate.
• Note that the protein is greater in VLDL than in chylomicrons, so it sinks rather than floats in plasma.
TG levels• (1) Optimal level < 150 mg/dL• (2) Borderline high level 150 to 199 mg/dL• (3) High level 200 to 499 mg/dL,• (4) Very high level > 500 mg/dL

Transports cholesterol in the bloodTransports cholesterol in the blood
Derives from continued hydrolysis of IDL Derives from continued hydrolysis of IDL by CPLby CPL
Removed from blood by LDL receptors in Removed from blood by LDL receptors in peripheral tissue peripheral tissue
Composition: 1) Protein (22%); 2) TG Composition: 1) Protein (22%); 2) TG (10%); CH (47%); (4) Phospholipid (21%)(10%); CH (47%); (4) Phospholipid (21%)
Calculated LDL = CH - HDL - TG/5Calculated LDL = CH - HDL - TG/5
1) Presence of chylomicrons falsely lowers 1) Presence of chylomicrons falsely lowers calculated LDL by increasing diet-derived calculated LDL by increasing diet-derived triglyceride; hence, fasting is required for triglyceride; hence, fasting is required for an accurate calculated LDL.an accurate calculated LDL.
2) To reduce the chance for a falsely low 2) To reduce the chance for a falsely low calculated LDL, LDL is directly measured calculated LDL, LDL is directly measured if the serum TG > 400 mg/dL.if the serum TG > 400 mg/dL.
Functions of cholesterol:Functions of cholesterol:
1) Component of the cell membrane.
2) Synthesis of vitamin D, adrenal cortex hormones, bile salts and acids.
Ranges of LDL:Ranges of LDL:
1) Optimal level < 100 mg/dL.1) Optimal level < 100 mg/dL.
• Risk for coronary heart Risk for coronary heart disease (CHD) markedly disease (CHD) markedly reducedreduced
2) Near optimal level is 100 to 129 2) Near optimal level is 100 to 129 mg/dL.mg/dL.
3) Borderline high level is 130 to 3) Borderline high level is 130 to 159 mg/dL.159 mg/dL.
4) High level is 160 to 189 mg/dL.4) High level is 160 to 189 mg/dL.
5) Very high level > 190 mg/dL.5) Very high level > 190 mg/dL.
• Greatest risk for CHDGreatest risk for CHD Fasting is Fasting is not required for an not required for an
accurate serum CH.accurate serum CH.
• • Note that the CH content in Note that the CH content in chylomicrons is <3%; hence, chylomicrons is <3%; hence, fasting does fasting does not have a not have a medically significant effect on medically significant effect on the serum level.the serum level.

“Good cholesterol”
• Increased by exercise, wine, estrogen
Composition: 1) Protein (50%); 2) TG (3%; unless VLDL is increased); 3) CH (20%);
4) Phospholipid (27%)
Synthesized by the liver and small intestine
Functions of HDL
1) Source of apolipoproteins for other lipoprotein fractions
2) Removes cholesterol from atherosclerotic plaques
a) Delivers CH from peripheral tissue to the liver
b) CH is either excreted into bile or converted into bile acids/salts.
Measured in the laboratory as HDL-CH
1) Inverse association of levels of HDL-CH and incidence and prevalence of CHD
2) Decreased if VLDL is increased
3) Ranges of HDL-CH
(a) High level (optimal) ≥ 60 g/dL
(b) Low level (suboptimal) < 40 mg/dL
4) Fasting is not required for an accurate serum HDL-CH.
Same reason as for serum CH.

• In the body, fatty acids are broken down to In the body, fatty acids are broken down to acetyl-CoAacetyl-CoA, which enters the , which enters the citric acid cyclecitric acid cycle. . • The main breakdown occurs in the mitochondria by β-oxidation. The main breakdown occurs in the mitochondria by β-oxidation. • Fatty acid oxidation Fatty acid oxidation begins with activation of the fatty acid, a reaction that occurs both inside and begins with activation of the fatty acid, a reaction that occurs both inside and
outside the mitochondria. outside the mitochondria. • Medium- and short-chain fatty acids can enter the mitochondria without difficulty, but long-chain Medium- and short-chain fatty acids can enter the mitochondria without difficulty, but long-chain
fatty acids must be bound to fatty acids must be bound to carnitinecarnitine in ester linkage before they can cross the inner in ester linkage before they can cross the inner mitochondrial membrane. mitochondrial membrane.
• Carnitine Carnitine is β-hydroxy-γ-trimethylammonium butyrate, and it is synthesized in the body from lysine is β-hydroxy-γ-trimethylammonium butyrate, and it is synthesized in the body from lysine and methionine. and methionine.
• A translocase moves the fatty acid-carnitine ester into the matrix space in exchange for free A translocase moves the fatty acid-carnitine ester into the matrix space in exchange for free carnitine. carnitine.
• In the matrix space, the ester is hydrolyzed, making the activated fatty acid molecule available for In the matrix space, the ester is hydrolyzed, making the activated fatty acid molecule available for β-oxidation and providing free carnitine for further exchange. β-oxidation and providing free carnitine for further exchange.
• β-Oxidationβ-Oxidation proceeds by serial removal of two carbon fragments from the fatty acid. The energy proceeds by serial removal of two carbon fragments from the fatty acid. The energy yield of this process is large. yield of this process is large.


• Deficient β-oxidation of fatty acids can be Deficient β-oxidation of fatty acids can be produced by produced by carnitine deficiency carnitine deficiency or or genetic genetic defects in the translocasedefects in the translocase or or other enzymes other enzymes involved in the transfer of long-chain fatty involved in the transfer of long-chain fatty acids into the mitochondria. acids into the mitochondria.
• This causes This causes cardiomyopathycardiomyopathy. . • In addition, it causes In addition, it causes hypoketonemic hypoketonemic
hypoglycemiahypoglycemia with with comacoma, a serious and , a serious and often fatal condition triggered by fasting, in often fatal condition triggered by fasting, in which glucose stores are used up because of which glucose stores are used up because of the lack of fatty acid oxidation to provide the lack of fatty acid oxidation to provide energy, and energy, and ketone bodies ketone bodies are not formed in are not formed in normal amountsnormal amounts because of the because of the lack of lack of adequate CoA in the liveradequate CoA in the liver..

In many tissues, acetyl-CoA units acetyl-CoA units condense to form acetoacetyl-CoAform acetoacetyl-CoA. In the liverliver, which (unlike other tissues) contains a deacylasecontains a deacylase, free aceto-acetate is formed. This β-keto acid β-keto acid is converted to β-hydroxybutyrateβ-hydroxybutyrate and acetoneacetone, and because these compounds are
metabolized with difficulty in the liver, they diffuse into the circulation. AcetoacetateAcetoacetate is also formed in the liver via the formation of 3-hydroxy-3-methylglutaryl-CoA, and this
pathway is quantitatively more important than deacylation. AcetoacetateAcetoacetate, β-hydroxybutyrateβ-hydroxybutyrate, and acetoneacetone are called ketone bodies (KB)ketone bodies (KB). Tissues other than liver transfer CoA from succinyl-CoA to acetoacetate and metabolize the "active"
acetoacetate to CO2 and H2O via the citric acid cycle. There are also other pathways whereby ketone bodies are metabolized.
AcetoneAcetone is discharged in the urine and expired air. The normal blood ketone level in humans is low (about 1 mg/dL) and less than 1 mg is excreted
per 24 hours, because the ketones are normally metabolized as rapidly as they are formed. However, if the entry of acetyl-CoA into the citric acid cycle is depressed entry of acetyl-CoA into the citric acid cycle is depressed because of a decreased supply of the decreased supply of the products of glucose metabolismproducts of glucose metabolism, or if the entry does not increase when the supply of acetyl-CoA increases, acetyl-CoA accumulates, the rate of condensation to acetoacetyl-CoA increases, and more more acetoacetate is formed in the liveracetoacetate is formed in the liver.
The ability of the tissues to oxidize the ketones oxidize the ketones is soon exceeded, and they accumulate in the bloodstream (ketosis).
Acetone Acetone breathbreath KB in urineKB in urine
KETONURIAKETONURIA KB in the bloodKB in the blood
KETONEMIA KETONEMIA pH - pH -
AcidosisAcidosisDehydra-Dehydra-
tationtation
Are Are osmotic!osmotic!

High-fat mealHigh-fat meal80 g TGs 80 g TGs
recommended daily recommended daily maxmaxTT
GG
Bile (liver)Bile (liver)Pancreatic lipasePancreatic lipaseColipase (protects lipase from the bile)Colipase (protects lipase from the bile)
2 – MG2 – MG ++ 2 FA2 FA
INTESTINEINTESTINE
MONOGLICERIDEMONOGLICERIDE
TGTGCHYLOMICROCHYLOMICRO
NSNS
LYMPLYMPHH
Via thoracicduct
Can’t pass membrane by they Can’t pass membrane by they own, they need be divided by own, they need be divided by
breakdownbreakdown
Blood Blood streamstream
Steatorrhea Steatorrhea ––Fatty stool (6% of Fatty stool (6% of
fats)fats)

AtherosclerosisAtherosclerosis is a form of is a form of arteriosclerosisarteriosclerosis in which in which thickeningthickening and and hardeninghardening of the vessel of the vessel are caused by the are caused by the accumulation of lipid-laden macrophages accumulation of lipid-laden macrophages within within the arterial wall, which leads to the formation of the arterial wall, which leads to the formation of a lesion called a a lesion called a plaque. plaque.
Atherosclerosis Atherosclerosis is is not a single disease but but rather a pathologic process that can rather a pathologic process that can affect affect vascular systems vascular systems throughout the body, resulting throughout the body, resulting in ischemic syndromes that can vary widely in in ischemic syndromes that can vary widely in their severity and clinical manifestations. their severity and clinical manifestations.
It is the leading contributor to It is the leading contributor to coronary artery coronary artery and and cerebrovascular diseasecerebrovascular disease..


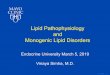
The mummified Egyptians, were likely to have been wealthy, and The mummified Egyptians, were likely to have been wealthy, and therefore probably consumed a lot of saturated fat. This is in fact not the first therefore probably consumed a lot of saturated fat. This is in fact not the first time that hardened arteries were identified in Egyptian mummies. And yet time that hardened arteries were identified in Egyptian mummies. And yet the Unangans, of the Aluetian Islands in Alaska, subsisted almost entirely on the Unangans, of the Aluetian Islands in Alaska, subsisted almost entirely on marine life. They, and the other mummies, were preserved naturally through marine life. They, and the other mummies, were preserved naturally through climate factors, not because they had attained any special status that would climate factors, not because they had attained any special status that would have privileged them with extra-rich foods. have privileged them with extra-rich foods. But that ancient people, too, had calcified arteries, "suggests that the But that ancient people, too, had calcified arteries, "suggests that the disease is an inherent component of human aging and not necessarily disease is an inherent component of human aging and not necessarily associated with any specific diet or lifestyle." Indeed, the mummies with associated with any specific diet or lifestyle." Indeed, the mummies with signs of calcification tended to be older, or what in those days counted as signs of calcification tended to be older, or what in those days counted as age: they died at around 43 years as opposed to 32. For each decade of life age: they died at around 43 years as opposed to 32. For each decade of life the mummies survived before being mummified, the risk of severe the mummies survived before being mummified, the risk of severe atherosclerosis increased by 69 percent.atherosclerosis increased by 69 percent.
Hatiay, a male Egyptian scribe who lived during the New Kingdom (1570-1293 BCE), enters the CT scanner. [The Lancet]
Evidence of carotid artery disease in Hatiay
• And yet ancient people of And yet ancient people of Egypt, Peru, southwest Egypt, Peru, southwest America, and Alaska America, and Alaska commonly suffered from commonly suffered from hardened arteries, too. hardened arteries, too. Using CT scans, Using CT scans, researchers examined researchers examined the remaining arteries of the remaining arteries of 137 mummies, and found 137 mummies, and found signs of probable or signs of probable or definite atherosclerosis in definite atherosclerosis in 34 % of them.34 % of them.



•Role of blood monocytes. Though blood monocytes do not possess receptors for normal LDL, LDL does appear in the monocyte cytoplasm to form foam cell. Plasma LDL on entry into the intima undergoes oxidation. The ‘oxidised LDL’ formed in the intima performs the following all-important functions on monocytes and endothelium: •For monocytes: Oxidised LDL acts to attract, proliferate,immobilise and activate them as well as is readily taken up by scavenger receptor on the monocyte to transform it to a lipid-laden foam cell.•For endothelium: Oxidised LDL is cytotoxic.•Death of foam cell by apoptosis releases lipid to form lipid core of plaque.

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
• 11. Injured endothelial cells . Injured endothelial cells become inflamedbecome inflamed and and cannot make normal amounts of antithrombotic cannot make normal amounts of antithrombotic and vasodilating cytokines.and vasodilating cytokines.
• 2. Numerous 2. Numerous inflammatory cytokines are releasedinflammatory cytokines are released, , including including tumor necrosis factor-alpha (TNF-α), tumor necrosis factor-alpha (TNF-α), interferongamma interferongamma (IFN-(IFN-γ), γ), interleukin-1 (IL-1), toxic interleukin-1 (IL-1), toxic oxygen radicals, and heat shock proteins.oxygen radicals, and heat shock proteins.
• 3. 3. Macrophages adhere to injured endothelium Macrophages adhere to injured endothelium by by way of adhesion molecules, such as vascular cell way of adhesion molecules, such as vascular cell adhesion molecule-1 (VCAM-1).adhesion molecule-1 (VCAM-1).
• 4. These 4. These macrophagesmacrophages then release enzymes and then release enzymes and toxic oxygen radicals that toxic oxygen radicals that create oxidative stresscreate oxidative stress, , oxidize LDLoxidize LDL, and , and further injure the vessel wallfurther injure the vessel wall..
• 55. Growth factors . Growth factors also are released, including also are released, including angiotensin II, fibroblast growth factor, and angiotensin II, fibroblast growth factor, and platelet-derived growth factor, which platelet-derived growth factor, which stimulate stimulate smooth muscle cell proliferation in the affected smooth muscle cell proliferation in the affected vesselvessel..
Once injury has occurred, endothelial dysfunction and inflammation Once injury has occurred, endothelial dysfunction and inflammation lead to the following pathophysiologic events:lead to the following pathophysiologic events:


Endothelial Dysfunction in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.
Macrophages play main role:
1. They have “scavenger”-
receptors so cholesterol
comes in macrophage
only due to concentration
difference.
2. They can accumulate a
lot of Chl inside (this
process is controlled by
HDLP only)
3. Changed LDLP
stimulate macrophages activity


Fatty-Streak Formation in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

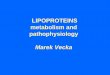
Formation of an Advanced, Complicated Lesion in Atherosclerosis
Ross R. N Engl J Med 1999; 340:115–126.

Cholesterol and
lisosomal enzymes irritates intimae
(because they are the alien bodies)
Excreation of proliferation factors by macrophages, еndotheliocytes, lymphocytes, thrombocytes
SMC migration in intimae and active proliferation collagen and elastin (capsule for Cholesterol and injured vessel wall isolation)

1. THROMBOSIS (due to endothelium damage)
2. Ulceration(necrosis of and releasing of lisosomal enzymes causes damage of plaque wall)
3. Calcinations(deposit of insoluble calcium salts)
4 4 stagestage - - COMPLICATIONSCOMPLICATIONS

Particle Uptake by Macrophage
Cholesterol Deposition;
Increased Plaque Burden
Particle Uptake by Macrophage
Cholesterol Deposition;
Increased Plaque Burden
Particle Movement into Intima
– Gradient driven
Particle Movement into Intima
– Gradient driven
Particle Oxidation Particle Oxidation
Adhesionmolecules MCP-1
Colony-stimulatingfactors
TissuefactorPAI-1
Endothelial cellscells
MonocyteMonocyte
Particle Retention
– Lipoprotein particle binding to proteoglycans
Particle Retention
– Lipoprotein particle binding to proteoglycans
Mildly modified LDL
Extensively modified LDL
“The rate of passive diffusion is increased when the circulating levels of LDL are elevated.” 1
“The rate of passive diffusion is increased when the circulating levels of LDL are elevated.” 1
Enhanced Endothelial Dysfunction
Enhanced Endothelial Dysfunction
1 Weissberg PL, Rudd JH. Textbook of Cardiovascular Medicine. 2002. p. 6.
LDL Particles Promote Atherogenesis
Lumen
Intima

Clinical EffectsClinical Effects
Major sites of atherosclerosis (serially numbered) in descending order of frequency.
The clinical effects of atherosclerosis depend upon the size and type of arteries affected. In general, the clinical effects result from the following:
1. Slow luminal narrowing causing ischaemia and atrophy.
2. Sudden luminal occlusion causing infarction necrosis.
3. Propagation of plaque by formation of thrombi and emboli.
4. Formation of aneurysmal dilatation and eventual rupture.
Accordingly, the symptomatic atherosclerotic disease involves most often the heart, brain, kidneys, small intestine and lower extremities
The effects pertaining to these organs are:1) AortaAorta—Aneurysm formation, thrombosis and
embolisation to other organs.2) HeartHeart—Myocardial infarction, ischaemic heart
disease.3) Brain—Chronic ischaemic brain damage,
cerebral infarction.4) Small intestineSmall intestine—Ischaemic bowel disease,
infarction.5) Lower extremitiesLower extremities—Intermittent claudication,
gangrene.


It is estimated that nearly half of the U.S. population has It is estimated that nearly half of the U.S. population has some form of some form of dyslipidemiadyslipidemia, especially , especially among white and among white and Asian Asian populations. These abnormalities are the result of a populations. These abnormalities are the result of a combination of genetic and dietary factors. combination of genetic and dietary factors.
PrimaryPrimary or familial dyslipoproteinemias result from or familial dyslipoproteinemias result from genetic genetic defects defects that cause abnormalities that cause abnormalities in lipid-metabolizing in lipid-metabolizing enzymes enzymes and and abnormal cellular lipid receptorsabnormal cellular lipid receptors. .
SecondarySecondary causes of dyslipidemia include several common causes of dyslipidemia include several common systemic disorders, such as systemic disorders, such as diabetesdiabetes, , hypothyroidismhypothyroidism, , pancreatitispancreatitis, and , and renal nephrosisrenal nephrosis, as well as the use of , as well as the use of certain medications such as certain certain medications such as certain diureticsdiuretics, , beta-blockersbeta-blockers, , glucocorticoidsglucocorticoids, , interferonsinterferons, and , and antiretroviralsantiretrovirals..
Optimal Optimal Near Optimal Near Optimal Desirable Desirable Low Low Borderline Borderline High High Very HighVery High
Total cholesterol Total cholesterol
<200 <200 200-239200-239 ≥≥240240
LDL LDL <100 <100 100-129 100-129 130-159 130-159 160-189 160-189 ≥≥190190
Triglycerides Triglycerides <150 <150 150-199 150-199 200-499 200-499 ≥≥500500
HDL HDL <40 <40 ≥≥6060
or or dyslipoproteinemiadyslipoproteinemia refers to abnormal refers to abnormal concentrations of serum lipoproteins concentrations of serum lipoproteins

Name Name Laboratory Findings Laboratory Findings Clinical Features Clinical Features TherapyTherapy
Type I: exogenous hyperlipidemia;fat-induced hypertriglyceridemia
Cholesterol normalTriglycerides increased three timesChylomicrons increased
Abdominal painHepatosplenomegalySkin and retinal lipid depositsUsual onset: childhood
Low-fat diet
Type IIa: hypercholesterolemia
Triglycerides normalLDL increasedCholesterol increased
Premature vascular diseaseXanthomas of tendons and bony prominencesCommonOnset: all ages
Low-saturated-fat and low-cholesterol dietCholestyramine (a); Colestipol (b); Lovastatin (c); Nicotinic acid (d) ;Neomycin (e).Intestinal bypass
Type IIb: combined hyperlipidemia;carbohydrate-induced hypertriglyceridemia
LDL, VLDL increasedCholesterol increasedTriglycerides increased
Same as IIa
Same as IIa; plus carbohydrate restrictionClofibrate (f); Gemfibrozil (g) Lovastatin
a) Cholestyramine (Questran), anion exchange resin; binds bile acids; enhances cholesterol excretion.b) Colestipol (Colestid), same as cholestyramine.c) Lovastatin, 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitor; decreases cholesterol synthesis in the liver.d) Nicotinic acid (niacin), decreases release of free fatty acids from adipose tissue; increases lipogenesis in liver; decreases glucagon release; most effective for type V disorder.e) Neomycin, experimental medication; questionable mode of action; decreases LDLs.f) Clofibrate (Atromid-S), decreases release of free fatty acids from adipose tissue; decreases hepatic secretion of VLDL and increases catabolism of VLDL.g) Gemfibrozil (Lopid), similar to clofibrate but increases HDLs more.

Name Name Laboratory Findings Laboratory Findings Clinical Features Clinical Features TherapyTherapy
Type III: Type III:
dysbetalipoproteinemiadysbetalipoproteinemia
IDL or chylomicron IDL or chylomicron
remnants increasedremnants increased
Cholesterol increasedCholesterol increased
Triglycerides increasedTriglycerides increased
Premature vascular Premature vascular
diseasedisease
Xanthomas of tendons Xanthomas of tendons
and bony prominencesand bony prominences
UncommonUncommon
Onset: adulthoodOnset: adulthood
Weight controlWeight control
Low-carbohydrate, low-Low-carbohydrate, low-
saturated-fat, andsaturated-fat, and
low-cholesterol dietlow-cholesterol diet
Alcohol restrictionAlcohol restriction
Clofibrate; Gemfibrozil; Clofibrate; Gemfibrozil;
Lovastatin; Nicotinic acid; Lovastatin; Nicotinic acid;
Estrogens Estrogens (h)(h)
Intestinal bypassIntestinal bypass
Type IV: endogenous Type IV: endogenous
hyperlipidemia;hyperlipidemia;
carbohydrate-induced carbohydrate-induced
hypertriglyceridemiahypertriglyceridemia
Glucose intoleranceGlucose intolerance
HyperuricemiaHyperuricemia
Cholesterol normal or Cholesterol normal or
increasedincreased
VLDL increasedVLDL increased
Triglycerides increasedTriglycerides increased
Premature vascular Premature vascular
diseasedisease
Skin lipid depositsSkin lipid deposits
ObesityObesity
HepatomegalyHepatomegaly
Common onset: adulthoodCommon onset: adulthood
Weight controlWeight control
Low-carbohydrate dietLow-carbohydrate diet
Alcohol restrictionAlcohol restriction
Clofibrate; Nicotinic acidClofibrate; Nicotinic acid
Intestinal bypassIntestinal bypass
Type V: mixed Type V: mixed
hyperlipidemia;hyperlipidemia;
carbohydrate and fat-carbohydrate and fat-
induced induced
hypertriglyceridemiahypertriglyceridemia
Glucose intoleranceGlucose intolerance
HyperuricemiaHyperuricemia
Chylomicrons increasedChylomicrons increased
VLDL increasedVLDL increased
LDL increasedLDL increased
Cholesterol increasedCholesterol increased
Triglycerides increased Triglycerides increased
three three timestimes
Abdominal painAbdominal pain
HepatosplenomegalyHepatosplenomegaly
Skin lipid depositsSkin lipid deposits
Retinal lipid depositsRetinal lipid deposits
Onset: childhoodOnset: childhood
Weight controlWeight control
Low-carbohydrate and Low-carbohydrate and
low-fat dietlow-fat diet
Clofibrate; Lovastatin;Clofibrate; Lovastatin;
Nicotinic acid; Nicotinic acid;
Progesterone Progesterone (i)(i)
Intestinal bypassIntestinal bypass
(h) Estrogens, decrease IDL levels in type III disorders; experimental.(i) Progesterone, decreases plasma triglycerides in type V disorders; experimental.

a. Epidemiology1) Autosomal recessive2) Rare childhood diseaseb. Pathogenesis1) Deficiency of CPL or2) Deficiency of apo C-llc. Clinical findings1) Chylomicrons are primarily increased
in early childhood.2) VLDL increases later in life.3) Presents with acute pancreatitis• Pancreatic vessels filled with
chylomicrons rupture.d. Laboratory findings1) Increase in serum TG > 1000 mg/dL
(primarily chylomicrons)2) Turbid supranate (chylomicrons) and
clear infranate (early childhood)3) Normal (usual case) to moderately
increased serum CH
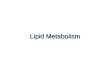
A: Lateral borders of thickened Achilles' tendons are shown with arrows. B: Tendinous xanthomas can also occur in the extensor tendons of the hands (shown), feet, elbows and knees. C: Xanthelasmas are cholesterol deposits in the eyelids. D: Arcus cornealis results from cholesterol infiltration around the corneal rim (arrow).

a. Laboratory findings
1) Serum LDL > 190 mg/dL
2) Serum CH > 260 mg/dL
a) Serum TG < 300 mg/dL (called type IIa)
b) Serum TG > 300 mg/dL (called type lIb)
b. Pathogenesis
• Decreased synthesis of LDL receptors.
c. Acquired causes of hypercholesterolemia
1) Primary hypothyroidism
• Decrease in LDL receptor synthesis or function
2) Nephrotic syndrome
• Increase in LDL correlates with the degree of hypoalbuminemia
3) Extrahepatic cholestasis (obstruction of bile)• Bile contains CH for excretion
d. Familial hypercholesterolemia
1) Autosomal dominant (AD) disorder
2) Deficiency of LDL receptors
3) Clinical findings
a) Premature coronary- artery- disease and stroke
b) Tendon xanthomas• Cholesterol deposit located over tendons (e.g.
Achilles) and extensor surfaces of joints
c) Xanthelasma• Yellow, raised plaque on the eyelid
e. Polygenic hypercholesterolemia (type Ila)
1) Most common hereditary cause (85% of cases)
2) Multifactorial (polygenic) inheritance
3) Alteration in regulation of LDL levels
4) Normal serum TG
f. Familial combined hypercholesterolemia (type lIb)
1) AD inheritance.
2) Serum CH and TG begin to increase around puberty.
3) Associated with metabolic syndrome.
4) Increase in CH and TG and decrease in HDL.

Familial dysbetalipoproteinemia ("remnant disease")1) AD inheritance2) Deficiency of apo E3) Decreased liver uptake of chylomicron remnants and IDL Clinical findings1) Palmar xanthomas in flexor creases2) Increased risk for coronary artery disease3) Increased risk for peripheral vascular disease (unlike type II disorders) Laboratorv findings1) Serum CH and TG > 300 mg/dL2) Serum CH 250 to 500 mg/dL3) LDL< 190 mg/dL4) Confirm diagnosis with ultracentrifugation to identify remnants • Lipoprotein electrophoresis and identification of apo E gene
defect are other studies that can be used. Treatment • Fibric acid derivatives

Laboratory findings
1) Serum TG > 300 mg/dL; 2) Serum CH 250 to 500 mg/dL; 3) Serum LDL < 190 mg/dL;
4) Turbid infranate after refrigeration
Increase in VLDL - due to increase in synthesis or decrease in catabolism
Acquired causes of hypertriglyceridemia
1) Excess alcohol intake
2) Oral contraceptives - estrogen increases synthesis of VLDL
3) Diabetes mellitus - decreased muscle and adipose CLP
4) Chronic renal failure - increased synthesis of VLDL
5) Thiazides, β-blockers - possible inhibition of CPL
Familial hypertriglyceridemia
1) Autosomal dominant disorder
2) Clinical findings
a) Eruptive xanthomas - yellow, papular lesions
(b) Increased risk for coronary artery- and peripheral
vascular disease
Tubero-eruptive xanthoma

a. Pathogenesis1) Increase in chylomicrons and VLDL2) Due to decreased activation and release of CPLb. Familial hypercholesterolemia (type IV) + exacerbating disorder• Exacerbating disorders — diabetic ketoacidosis (DKA: most common), alcoholc. Increased serum TG > 1000 mg/dL; normal CH and LDL.d. Turbid plasma1) Supranate after refrigeration, due to increased chylomicrons2) Infranate after refrigeration, due to increased VLDL.e. Hyperchylomicronemia syndrome1) Eruptive xanthomas2) Increased incidence of acute pancreatitis3) Lipemia retinalis - retinal vessels look like milk: blurry vision4) Dyspnea and hypoxemia - impaired gas exchange in pulmonary capillaries5) Hepatosplenomegaly6) Increase in serum TG (usually >1000 mg/dL)7) Normal serum CH and LDL8) Turbid supranate and infranate after refrigerationf. Treatment(1) Treat exacerbating disorder (e.g.. DKA)(2) Nicotinic acid or fibric acid derivatives

Apolipoprotein B deficiency (abetalipoproteinemia)
a. Autosomal recessive
b. Deficiency of apolipoprotein B-48 and B-100• (1) Deficiency of chylomicrons, VLDL and
LDL• (2) Decrease in serum CH and TG
c. Clinical findings
1) Malabsorption
a) Chylomicrons accumulate in villi and prevent reabsorption of micelles.
b) Marked decrease in vitamin E
2) Ataxia (spinocerebellar degeneration), hemolytic anemia with thorny RBCs (acanthocytes) related to vitamin E deficiency.
d. Treatment - vitamin E


ObesityObesity an excess of adipose tissue that imparts an excess of adipose tissue that imparts health risk; a body weight of 20% excess over ideal health risk; a body weight of 20% excess over ideal weight for age, sex and height is considered a health weight for age, sex and height is considered a health risk. risk.
•1. Body mass index (BMI) > 30kg/m2 (normal, 19.5-24.9kg/m2)•1) Excess fat in the waist and flanks is
more important than an excess in the thighs and buttocks.
•2) Excess visceral fat in the abdominal cavity has greater significance than excess subcutaneous fat.
•Magnetic resonance imaging is used to access the amount of visceral fat.
Body mass index (Body mass index (BMIBMI) which is equal to ) which is equal to weight in weight in kg/height in m2kg/height in m2

ETIOLOGY ETIOLOGY ObesityObesity results when caloric intake results when caloric intake
exceeds utilisation.exceeds utilisation. The imbalance of these two The imbalance of these two
components can occur in the components can occur in the following situations:following situations:
1. 1. InadequateInadequate pushing of oneself away from the dining table pushing of oneself away from the dining table causing causing overeating.overeating.
2. 2. Insufficient Insufficient pushing of oneself out of the chair leading to pushing of oneself out of the chair leading to inactivity and inactivity and sedentary life style.sedentary life style.
3. 3. GeneticGenetic predisposition to develop obesity. predisposition to develop obesity.
4. 4. DietsDiets largely derived from carbohydrates and fats than largely derived from carbohydrates and fats than protein-rich diet.protein-rich diet.
5. 5. Secondary obesity Secondary obesity may result following a number of underlying may result following a number of underlying diseases diseases such as hypothyroidism, Cushing’s disease, insulinoma and hypothalamic such as hypothyroidism, Cushing’s disease, insulinoma and hypothalamic disorders.disorders.

LeptinSatiety (hunger/appetite suppression) and regulation of eating behavior by hypothalamusSympathoactivationInsulin sensitizingModulating role in reproduction, angiogenesis, immune response, blood pressure control, and osteogenesisAdiponectinInsulin sensitizingAnti-inflammatoryAnti-atherogenicResistinPromotes insulin resistance and increased blood glucose levelsInhibits adipocyte differentiation and may function as a feedback regulator of adipogenesisVisfatin (from visceral fat)Mimics insulin and binds to insulin receptors in ratsVaspin—may be insulin sensitizing
Hormones (AdipokinesHormones (Adipokines)
Lipoprotein lipaseApolipoprotein ECholesterol ester transfer protein
Regulators of Lipoprotein Regulators of Lipoprotein MetabolismMetabolism
Inflammatory Inflammatory CytokinesCytokinesTumor necrosis factor-alphaInterleukins (IL-6, IL-8, IL-10)Plasminogen activator inhibitor-1Monocyte chemoattractant protein-1
Other Hormones and Other Hormones and CytokinesCytokinesEstrogen
AngiotensinogenTissue factorTransforming growth factor-betaInsulin-like growth factorNitric oxide synthaseAcylation stimulating proteinAdipophilinAdipoQMonobutyrinAgouti protein

Regulation of appetite and satiety occurs through Regulation of appetite and satiety occurs through neuroendocrine regulation of eating behavior, energy neuroendocrine regulation of eating behavior, energy metabolism, and body fat mass. The system is complex and metabolism, and body fat mass. The system is complex and controlled by a dynamic circuit of signaling molecules from controlled by a dynamic circuit of signaling molecules from the periphery acting on central controls including the brain the periphery acting on central controls including the brain stem, hypothalamus, and autonomic nervous system. An stem, hypothalamus, and autonomic nervous system. An imbalance in this system is usually associated with excessive imbalance in this system is usually associated with excessive caloric intake in relation to exercise with the consequence of caloric intake in relation to exercise with the consequence of weight gain and obesity.weight gain and obesity.
The The arcuate nucleus (ARC)arcuate nucleus (ARC) in the hypothalamus has two in the hypothalamus has two sets of neurons with opposing effects that interact to sets of neurons with opposing effects that interact to regulate and balance food intake and energy metabolism. regulate and balance food intake and energy metabolism.
One set of neurons produces One set of neurons produces neuropeptide Y (NPY)neuropeptide Y (NPY) and and agoutirelated protein (AGRP)agoutirelated protein (AGRP), which , which stimulates eating stimulates eating and and decreases metabolismdecreases metabolism (anabolic). (anabolic).
Another set of neurons synthesizes Another set of neurons synthesizes pro-opiomelanocortin pro-opiomelanocortin (POMC)(POMC)-producing peptide and -producing peptide and cocaineand-amphetamine-cocaineand-amphetamine-regulated transcript (CART)regulated transcript (CART), collectively known as , collectively known as POMC/CART POMC/CART neurons. They neurons. They inhibit eating inhibit eating and and increase increase metabolismmetabolism (catabolic). (catabolic).
Both sets of neurons express their effects by activating Both sets of neurons express their effects by activating second-order neurons in the hypothalamus, which increases second-order neurons in the hypothalamus, which increases or decreases appetite and energy metabolism.or decreases appetite and energy metabolism.

Fat cell mass
[Leptin/insulin] expression
[Leptin/insulin] action in hypothalamusNPY/AGRP
neurons
POMC/CARTneurons
NPY/AGRPexpression
Food intakeSympathetic activity
CART α-MSH expressionand release
NPY release AGRP release
CatabolismCatabolism
α-MSH binding andactivation of melanocortin
MC4R receptors
Food intakeFood intakeEnergyEnergy expenditureexpenditure
Leptin and insulin normally decrease appetite, increase satiety, and increase energy expenditure (catabolism). Leptin/insulin inhibits NPY/AGRP gene expression resulting in decreased appetite and food intake; and stimulates POMC/CART gene expression with resulting α-MSH release and decrease in appetite and food intake. With leptin resistance as occurs in obesity, these effects are depressed and food intake increases in excess of energy expenditure. AGRP, agouti-related peptide; α-MSH, alpha-melanocyte stimulating hormone; NPY, neuropeptide Y; POMC/CART, proopiomelanocortin/cocaine-and-amphetamine-related transcript
Arcuate nucleus
Paraventricular
nucleus

Neuropeptide Y (NPY) Melanin-concentrating hormone (MCH) Agouti-related protein (AGRP) Ghrelin Galanin Orexins A and B Peptide YY (PYY) Cortisol
Leptin Insulin Cholecystokinin (CCK) Corticotropin-releasing hormone (CRF) Urocortin (a CRF satiety signaling hormone) Cocaine- and amphetamine-regulated transcript (CART) Alpha-melanocyte-stimulating hormone (α-MSH) Bombesin Serotonin Calcitonin
molecules that stimulate eatingmolecules that stimulate eating
molecules that inhibit eating

GhrelinGhrelin is produced by the stomach in response to hunger is produced by the stomach in response to hunger and stimulates and stimulates food intake and induces metabolic changes leadingfood intake and induces metabolic changes leading to an increase in body to an increase in body weight and body fat mass. weight and body fat mass. GhrelinGhrelin also stimulates release of growth also stimulates release of growth hormone (GH) from anteriorhormone (GH) from anterior pituitary cells, the release of gastric acid and pituitary cells, the release of gastric acid and gastric motility,gastric motility, and affects pancreatic functions. It hasand affects pancreatic functions. It has vasodilatory, vasodilatory, cardioprotective,cardioprotective, and antiproliferative effects.and antiproliferative effects.
AdiponectinAdiponectin has insulin-sensitizing properties and plasma has insulin-sensitizing properties and plasma levels decrease levels decrease with visceral obesity, contributing to insulinwith visceral obesity, contributing to insulin resistance, cardiovascular resistance, cardiovascular disease, and metabolic syndrome.disease, and metabolic syndrome.
ObeseObese individuals, particularly those with expansion of visceral individuals, particularly those with expansion of visceral adipose adipose tissue, are at increased risk for coronary arterytissue, are at increased risk for coronary artery disease resulting from disease resulting from hyperlipidemia, hypertension, and factorshyperlipidemia, hypertension, and factors that promote thrombosis and that promote thrombosis and inflammationinflammation..
Decreased adiponectin levels are associated with increased levels of inflammatory markers, such as IL-6 and TNF-α.
Adiponectin may serve as an anti-inflammatory and anti-atherogenic plasma protein and may have an important role in vascular remodeling that is limited with obesity.
Obesity is associated with insulin resistance, which predisposes an individual to type 2 diabetes mellitus. The insulin resistance may be related to an insulin receptor defect or to postreceptor effects with alteration in glucose transporter functions. Excess insulin also may be a response to excessive caloric intake.
Resistin is greatly increased in those with obesity and may be an antagonist to insulin action and a mediator of inflammation.

PathogenesisPathogenesis a. Genetic factors a. Genetic factors account for 50% to 80% of eases.account for 50% to 80% of eases. • • Examples—defects in the leptin gene, syndrome X (obesity, Examples—defects in the leptin gene, syndrome X (obesity,
hypertension, diabetes)hypertension, diabetes) b. Acquired causesb. Acquired causes (1) Endocrine disorders—hypothyroidism, Cushing syndrome(1) Endocrine disorders—hypothyroidism, Cushing syndrome (2) Hypothalamic lesions, menopause(2) Hypothalamic lesions, menopause c. Leptinc. Leptin 1) Leptin is a hormone.1) Leptin is a hormone. a) Secreted by adipose tissuea) Secreted by adipose tissue b) Maintains energy balance (intake and output)b) Maintains energy balance (intake and output) 2) Leptin increases when adipose stores are adequate.2) Leptin increases when adipose stores are adequate. a) Decreases food intake (inhibits satiety center)a) Decreases food intake (inhibits satiety center) b) Increases energy expenditure (stimulates (b) Increases energy expenditure (stimulates (ββ-oxidation -oxidation
of fatty- acids)of fatty- acids) 3) Leptin decreases when adipose stores are inadequate.3) Leptin decreases when adipose stores are inadequate. a) Increases food intake (stimulates the satiety center)a) Increases food intake (stimulates the satiety center) b) Decreases energy expenditure (inhibits b) Decreases energy expenditure (inhibits ββ-oxidation of -oxidation of
fatty acids)fatty acids) 4) Obesity related to leptin dysfunction may be caused by the 4) Obesity related to leptin dysfunction may be caused by the
following;following; a) Resistance to leptin effectsa) Resistance to leptin effects b) Mutations resulting in inhibition of leptin releaseb) Mutations resulting in inhibition of leptin release

• 1. Hyperinsulinaemia. Increased insulin secretion is a feature of obesity. Many obese individuals exhibit hyperglycaemia or frank diabetes despite hyperinsulinaemia. This is due to a state of insulin-resistance consequent to tissue insensitivity.
• 2. Type 2 diabetes mellitus. There is a strong association of type 2 diabetes mellitus with obesity. Obesity often exacerbates the diabetic state and in many cases weight reduction often leads to amelioration of diabetes.
• 3. Hypertension. A strong association between hypertension and obesity is observed which is perhaps due to increased blood volume. Weight reduction leads to significant reduction in systolic blood pressure.

4. Hyperlipoproteinaemia. The plasma cholesterol circulates in the blood as low-density lipoprotein (LDL) containing most of the circulating triglycerides. Obesity is strongly associated with VLDL and mildly with LDL. Total blood cholesterol levels are also elevated in obesity.
5. Atherosclerosis. Obesity predisposes to development of atherosclerosis. As a result of atherosclerosis and hypertension, there is increased risk of myocardial infarction and stroke in obese individuals.
6. Nonalcoholic fatty liver disease (NAFLD). Obesity contributes to development of NAFLD which may progress further to cirrhosis of the liver.
7. Cholelithiasis. There is six times higher incidence of gallstones in obese persons, mainly due to increased total body cholesterol.

8. 8. Hypoventilation syndrome (Pickwickian Hypoventilation syndrome (Pickwickian syndrome). syndrome). This is characterised by This is characterised by hypersomnolence, both at night and during day hypersomnolence, both at night and during day in obese individuals along with carbon dioxide in obese individuals along with carbon dioxide retention, hypoxia, polycythaemia and retention, hypoxia, polycythaemia and eventually right-sided heart failure. (Mr Pickwick eventually right-sided heart failure. (Mr Pickwick was a character, the fat boy, in Charles Dickens’ was a character, the fat boy, in Charles Dickens’ Pickwick Papers. The term pickwickian Pickwick Papers. The term pickwickian syndrome was first used by Sir William Osler for syndrome was first used by Sir William Osler for the sleepapnoea syndrome).the sleepapnoea syndrome).
9. 9. Osteoarthritis.Osteoarthritis. These individuals are more These individuals are more prone to prone to develop degenerative joint disease develop degenerative joint disease due to wear and tear following trauma to joints due to wear and tear following trauma to joints as a result of large body weight.as a result of large body weight.
10. 10. Cancer.Cancer. Diet rich in fats, particularly Diet rich in fats, particularly derived from animal derived from animal fats and meats, is fats and meats, is associated with higher incidence of cancers of associated with higher incidence of cancers of colon, breast, endometrium and prostate.colon, breast, endometrium and prostate.


CLINICAL FINDINGCLINICAL FINDING COMMENTSCOMMENTS
CancerCancerIncreased incidence of estrogen-related cancers (e.g., endometrial, breast) because of increased aromatization of androgens to estrogens in adipose tissue
CholelithiasisCholelithiasisIncreased incidence of cholecystitis and cholesterol stones: bile is supersaturated with cholesterol
Diabetes meDiabetes melllitus, litus,
type type 22
Increased adipose downregulates insulin receptor synthesis Hyperinsulinemia increases adipose storesWeight reduction upregulates insulin receptor synthesis
HepatomegalyHepatomegaly Fatty change accompanied by liver cell injury and repair by fibrosis
HypertensionHypertensionHyperinsulinemia increases sodium retention, leading lo increase in plasma volumeLeft venlricular hypertrophy and stroke complicate hypertension
HypertriglyceridemiaHypertriglyceridemiaHypertriglyceridemia decreases serum high-density lipoprotein levels, increasing risk of coronary artery disease
Increased low-density Increased low-density
lipoprotein levelslipoprotein levelsHypercholesterolemia predisposes lo coronary artery disease
Obstructive sleep Obstructive sleep
apneaapnea
Weight of adipose tissue compresses upper airways causing respiratory acidosis and hypoxemiaPotential for developing cor pulmonale (pulmonary hypertension and right ventricular hypertrophy)
OsteoarthritisOsteoarthritis Degenerative arthritis in weight-bearing joints (e.g., femoral heads)



Prader-Willi syndrome Prader-Willi syndrome (PWS) is a single gene imprinting disorder (Psora/ Syphilis) caused by defects in chromosome 15. These defects may be of two types:
1. Paternally inherited deletion or disruption of genes in the proximal arm of chromosome 15. (Syphilis)
2. Maternal disomy in the proximal arm of chromosome 15. (Psora) Related wordsRelated words Cryptorchidism-dwarfism-subnormal mentality; hypogenital dystrophy
with diabetic tendency; hypotonia-hypomentia-hypogonadism-obesity syndrome; Labhart-Willi syndrome; Prader-Labhart-Willi Fancone syndrome; Willi-Prader syndrome.
Historical BackgroundHistorical Background The first patient with Prader-Willi syndrome was described by Langdon-Down In
1887 as an adolescent girl with mental impairment (Psora), short stature (Psora), hypogonadism (Psora), obesity (Psora). He called these symptoms to polysarcia.
In 1956, Prader et al reported some patients with similar phenotypes. In 1981, Ledbetter et al identified microdeletions (Syphilis) within chromosome 15
and determined it to be the site for Prader-Willi syndrome.

• PathophysiologyPathophysiology• Prader-Willi syndrome Prader-Willi syndrome is the first is the first
human disorder recognized to human disorder recognized to genomic imprinting. In such genomic imprinting. In such disorders, genes are expressed disorders, genes are expressed differentially based on the parent of differentially based on the parent of origin. It results from the loss of origin. It results from the loss of imprinted genomic material within imprinted genomic material within the the paternal paternal 15q11.2-13 locus. 15q11.2-13 locus.
• The loss of The loss of maternalmaternal genomic genomic material (Syphilis) at the 15q11.2-13 material (Syphilis) at the 15q11.2-13 locus results in locus results in Angelman Angelman syndromesyndrome..
• Most cases of Prader-Willi Most cases of Prader-Willi syndrome that involve deletions syndrome that involve deletions (Syphilis), unbalanced (Syphilis), unbalanced translocations (Psora), and translocations (Psora), and uniparental (maternal) disomy uniparental (maternal) disomy (Psora) are sporadic.(Psora) are sporadic.

ChildrenChildren• HyperphagiaHyperphagia (Psora) with (Psora) with progressive development of obesity progressive development of obesity (Psora).(Psora).• Short stature Short stature (Psora) with lack of (Psora) with lack of pubertal growth shot (Syphilis).pubertal growth shot (Syphilis).• Sleep disturbances Sleep disturbances (Psora), (Psora), obstructive sleep apnea and obstructive sleep apnea and narcolepsy (Psora).narcolepsy (Psora).• Growth hormone deficiency Growth hormone deficiency (Psora).(Psora).• Premature growth Premature growth of pubic and of pubic and axillary hair (Psora) but other axillary hair (Psora) but other features of Prader-Willi syndrome are features of Prader-Willi syndrome are usually delayed or incomplete.usually delayed or incomplete.• Testicular descent late Testicular descent late (Psora) ; menarche may occur as late as age 30 (Psora) ; menarche may occur as late as age 30
(Psora).(Psora).• Features of psychosis Features of psychosis and behavioural problems- temper outbursts (Psora), and behavioural problems- temper outbursts (Psora), stubborn (Psora), and obsessive-compulsive behaviour (Psora), eating stubborn (Psora), and obsessive-compulsive behaviour (Psora), eating garbage (Psora) and frozen food (Psora), and stealing resources to obtain garbage (Psora) and frozen food (Psora), and stealing resources to obtain food (Psora) leading to gastric complications, gastric necrosis (Psora/Syphilis) food (Psora) leading to gastric complications, gastric necrosis (Psora/Syphilis) and even death.and even death.• Mild mental retardation (Psora).Mild mental retardation (Psora).• Obesity complications- sleep apnoea (Psora), cor pulmonale Obesity complications- sleep apnoea (Psora), cor pulmonale (Psora/Sycosis), diabetes mellitus (Pseudopsora), atherosclerosis (Sycosis).(Psora/Sycosis), diabetes mellitus (Pseudopsora), atherosclerosis (Sycosis).


SPINGOLIPIDS. DISORDERS
Classes of sphingolipids and their hydrophilic groups include: Sphingomyelin: phosphorylcholine Cerebrosides: galactose or glucose Gangliosides: branched oligosaccharide chains terminating in
the 9-carbon sugar, sialic acid (N-acetylneuraminic acid, NANA)
Sphingolipids released when membrane is degraded are digested in endosomes after fusion with lysosomes. Lysosomes contain many enzymes, each of which removes specific groups from individual sphingolipids. Genetic deficiencies of many of these enzymes are known, and the diseases share some of the characteristics of I-cell disease.

DiseaseLysosomal
Enzyme Missing
Substrate Accumulating in Inclusion Body
Symptoms
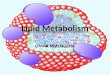
Tay-Sachs Hexosaminidase A Ganglioside GM2Cherry red spots in macula; blindness
Gaucher Glucocerebrosidase Glucocerebroside
Type 1: AdultHepatosplenomegaly Erosion of bones, fractures; Pancytopenia or thrombocytopenia; Characteristic macrophages (crumpled paper inclusions)
Niemann-Pick
Sphingomyelinase Sphingomyelin
Cherry red spot in maculaHepatosplenomegaly, Microcephaly, severe mental retardation; Zebra bodies in inclusions; Characteristic foamy macrophages; Early death

The bright light at right enters through the pupil of the eye; at left, the “red spot” in diagnosis of Tay-Sachs disease
Adult onset Niemann-Pick disease type C presenting with psychosis


VitaminVitamin EFFECTS OF DEFICIENCYEFFECTS OF DEFICIENCY EFFECTS OF TOXICITYEFFECTS OF TOXICITY
AARetinolRetinol
Ocular lesions: night blindness, xerophthalmia - dry and scaly scleral conjunctiva; keratomalacia - corneal ulcers may occur which may get infected; Bitot’s spots - focal triangular areas of opacities due to accumulation of keratinised epithelium; blindness - squamous metaplasia of corneal epithelium)Cutaneous lesions: xeroderma - the skin develops papular lesions giving toad-like appearance, due tofollicular hyperkeratosis and keratin plugging in thesebaceous glands; Other lesions: squamous metaplasia of respiratory epithelium, pneumonia; urothelium and pancreatic ductal epithelium, subsequent anaplasia; retarded bone growth; renal calculi
Papilledema and seizures (due to an increase In intracranial pressure), hepatitis, bone pain (due to periosteal proliferation)
DDCalcitriolCalcitriol
Pathologic fractures, excess osteoid, bow legsChildren: rickets; craniotabes (soft skull bones); rachitic rosary (defective mineralization and overgrowth of epiphyseal cartilage in ribs)Adults: called osteomalaciaContinuous muscle contraction (hypocalcaemic tetany)
Hypercalcemia with metastatic calcification, renal calculi

VitaminVitamin EFFECTS OF DEFICIENCYEFFECTS OF DEFICIENCY EFFECTS OF TOXICITYEFFECTS OF TOXICITY
EEαα--
Tocophe-Tocophe-
rolrol
Hemolytic anemia (damage to RBC membrane), reduced red cell lifespan;Peripheral neuropathy, degeneration of posterior column (poor joint sensation) and spinocerebellar tract (ataxia), retinal pigments, degeneration axons of peripheral nerves; denervation of musclesSterility in male and female animals
Decreased synthesis of vitamin K-dependent procoagulant factors;synergistic effect with
warfarin anticoagulation
KK
Newborns: Hypoprothrombinaemia in hemorrhagic disease of newborn (CNS bleeding, ecchymoses); Adults: gastrointestinal bleeding, ecchymoses; prolonged prothrombin time and partial thromboplastin time biliary obstruction - bile is prevented from entering the bowel due to biliary obstruction which prevents the absorption of this fat-soluble vitamin. Surgery in patients of obstructive jaundice, therefore, leads to marked tendency to bleeding. malabsorption of fat develop vitamin K deficiency e.g. coeliac disease, sprue, pancreatic disease, hypermotility of bowel etc. anticoagulant therapy - patients on warfarin group of anticoagulants have impaired biosynthesis of vitamin K-dependent coagulation factors.antibiotic therapy - the use of broad-spectrum antibiotics and sulfa drugs reduces the normal intestinal flora. diffuse liver disease - (e.g. cirrhosis, amyloidosis of liver, hepatocellular carcinoma, hepatoblastoma) have hypoprothrombinaemia due to impaired synthesis of prothrombin. Administration of vitamin K to such patients is of no avail since liver, where prothrombin synthesis utilising vitamin K takes place, is diseased.
Hemolytic anemia and jaundice in newborns if mother receives excess
vitamin K

1. Copstead Lee-Ellen C. Pathophysiology / Lee-Ellen C. Copstead, Jacquelyn L. Banasic // Elsevier Inc. – 2010.
2. ROBBINS BASIC PATHOLOGY / [edited by] Vinay Kumar, Abul K. Abbas, Jon C. Aster. – 9th ed. – 2013.
3. Kathryn L. McCance . Pathophysiology: the biologic basis for disease in adults and children / [edited by] Kathryn L. McCance, Sue E. Huether; section editors, Valentina L. Brashers, Neal S. Rote - 6th ed. – 2010.
4. Pathophysiology, Concepts of Altered Health States, Carol Mattson Porth, Glenn Matfin.– New York, Milwaukee. – 2009.
5. Essentials of Pathophysiology: Concepts of Altered Health States (Lippincott Williams & Wilkins), Trade paperback (2003) / Carol Mattson Porth, Kathryn J. Gaspard. Chapters 15, 29.
6. General and clinical pathophysiology. Edited by prof. A.V. Kubyskin. Simferopol. – 2011.
7. Silbernagl S. Color Atlas of Pathophysiology / S. Silbernagl, F. Lang // Thieme. Stuttgart. New York. – 2000.