Embed Size (px)
Citation preview

Patient-reported outcomes for asthma in children and adults
Marion Sills, MD, MPHBarbara Yawn, MD, MPH
Monica Federico, MDBethany Kwan, PhD, MSPH
Presentation to the SAFTINet PECApril 1, 2011

Asthma Monitoring• Office based
pulmonary function test units to be installed by SAFTINet in partner practices*
*Only on April 1
SAFTINet PFT

Objectives of this discussion• Present 2 asthma PRO tools, including pros
and cons of each• Discuss process for selecting one tool that
will be used by all partners• Discuss questions, considerations, and
processes that each organization will need to address
• Timeline

Review: SAFTINet partners’ current use of asthma PRO tools• Assessments in narratives only• No use of standardized, validated, uniform
tools

SAFTINet Partner Requirements for a PRO tool• Simplicity• Does not interfere with workflow• Appropriate for literacy level and language
of patient populations• Alignment with other organizational efforts
and initiatives

Rationale for use of PROs for children and adults with asthma in SAFTINet• Clinical utility
– Screening tool– Patient monitoring tool– Patient centered care (feedback to patients)– Decision aid– Facilitating multidisciplinary team communications
• Research utility– Standardized evaluation of outcomes
• Why asthma?– Effects of disease on functioning and quality of life not accounted for in
standard EHR data– Severity of disease difficult to assess– Patients experience symptoms (unlike hypertension)

What the guidelines say• Expert Panel Report 3 (EPR-3):
Guidelines for the Diagnosis and Management of Asthma
• EPR-3: “The key elements of assessment and monitoring are refined to include the separate, but related, concepts of severity, control, and responsiveness to treatment.”

What the guidelines say• EPR-3 recommends that clinicians
– Identify precipitating factors – Identify comorbidities that may aggravate
asthma – Assess patient’s knowledge/skills for self-
mgt – Classify asthma severity

What the guidelines say• EPR-3 recommends that clinicians
– Identify precipitating factors – Identify comorbidities that may aggravate
asthma [from chart, history]– Assess patient’s knowledge/skills for self-
mgt – Classify asthma severity

What the guidelines say• EPR-3 recommends that clinicians
– Identify precipitating factors – Identify comorbidities that may aggravate
asthma [from chart, history]– Assess patient’s knowledge/skills for self-
mgt – Classify asthma severity

What the guidelines say• EPR-3 recommends that clinicians
– Classify asthma severity
“Assessment is made on the basis of current spirometry and the patient’s recall of symptoms over the previous 2–4 weeks.”

What the guidelines say• EPR-3 recommends that clinicians
– Classify asthma severity• Nighttime awakenings• Daytime symptoms • Need for SABA* for quick relief of symptoms • Work/school days missed • Ability to engage in normal daily activities or in
desired activities • Quality-of-life assessments
*SABA: short-acting beta-agonist, a “rescue” or “quick relief” medication

What the guidelines sayEPR-3 recommendation ACT APGAR
Precipitating factors
Patient’s self-mgt knowledge/skills
Nighttime awakenings
Daytime symptoms
Need for rescue SABA
Work/school days missed
Engage in normal daily activities
Quality-of-life

Proposed tools• Asthma Control Test (ACT, C-ACT)• Asthma APGAR

ACT• 2 versions: adult (5
questions) and child (7 questions)
• GlaxoSmithKline product
• Score range 5-25; <20 may indicate need for greater asthma control


Engage in normal daily activities
Nighttime awakenings
Daytime symptoms
Overall (acute) severity

Daytime symptoms
Daytime symptoms
Nighttime awakenings

Engage in normal daily activities
Nighttime awakenings
Daytime symptoms
Overall severity
Need for rescue SABA

Comparing ACT to EPR-3 recommendationsEPR-3 recommendation ACT APGAR
Precipitating factors N
Patient’s self-mgt knowledge/skills N
Nighttime awakenings Y
Daytime symptoms Y
Need for rescue SABA Y (adult)
Work/school days missed N
Engage in normal daily activities Y
Quality-of-life Y
4 weeks of symptomsAdult and child4-5 options/question5-7 questions<20 = poor control

ACT pros and consPROs
• Well validated• Widely used• Minimal level for good
control and MCID established
• Translated into many languages
CONs• Long questions• Does not include days
missed from school/work
• No guide to how to use the results
• Not studied in association with clinical outcomes

ACT pros
Widely validated

If ACT <20, then what?

Asthma APGAR• Designed to measure severity to include elements
missing in > 60% of primary care charts: – trigger exposure– adherence to prescribed therapy– patient reported value of their asthma therapy
• Developed by Dr. Yawn in collaboration with practicing primary care physicians—– face validity– practical

AS
THM
A A
PG
AR
Engage in normal daily activities
Daytime symptoms
Nighttime awakenings
Precipitating factors
Patient’s self-mgt knowledge/skills
Need for rescue SABA
Quality-of-life
Patient’s self-mgt knowledge/skills

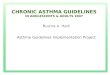
Comparing ACT and APGAR to EPR-3EPR-3 recommendation ACT APGAR
Precipitating factors N Y
Patient’s self-mgt knowledge/skills N Y
Nighttime awakenings Y Y
Daytime symptoms Y Y
Need for rescue SABA Y (adult) Y
Work/school days missed N N
Engage in normal daily activities Y Y
Quality-of-life Y Y
4 weeks of symptomsAdult and child4-5 options/question5-7 questions<20 = poor control
2 weeks of symptomsNo child version3 options/question8 questionsAlgorithm for mgt

Asthma APGAR• PROs
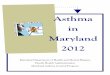
– Addresses missed and modified activities– Addresses most common causes of poor control– Is linked to an algorithm for next steps– Shown to improve outcomes in clinical practice– Test/retest, face validity and comparable to EPR-3
• CONs– Not compared to ACT for validation– Minimally clinically significant difference unknown

APGAR algorithm

Comparing the ACT and the Asthma APGAR• Similarities
– Test for symptoms, activity limitations, and use of rescue medications
• Differences– ACT more widely validated– ACT is shorter– ACT has child version– APGAR has linked treatment algorithm– APGAR addresses asthma triggers, adherence to
prescribed medications, and patient’s perception of asthma relief from therapy

Questions and considerations• What would the tool be used for in your organization?• What resources are required? • Which patients will you assess?• How often should patients complete questionnaires? Should it
be tied to visits or a way to follow patients between visits?• How will the tool be administered and scored? • What tools are available to aid in interpretation and how will
scores requiring follow-up be determined?• When, where, how, and to whom will results be presented?• How will the value of using PROs be evaluated?• Which key barriers require attention?

Clinical utility• Likely utility of Asthma PROs:
– Patient monitoring tool– Decision aid
• Less likely utility for asthma PROs– Screening tool– Feedback to patients– Facilitating multidisciplinary team
communications

Resources• Manpower• Information systems and technical support• Space• Financial investment (SAFTINet funds
available)

Selecting patients to complete the tool• Ambulatory patients with asthma
– How would they be identified?• How often would they complete the tool?
– Every ambulatory visit?• When does the patient complete the tool?
– Beginning of visit?

Mode of administration• Person completing the tool
• Self-administration• Interviewer administration
• Medium for presentation of tool and data collection• Pencil and paper survey• EHR template• Portable devices (e.g., iPad)• Web-based• Telephony-based

Scoring• Who will score the results?
• Patient• Member of the health care team
• What tools are available to assist with scoring?

Presentation of results• Are results presented to patient/provider?• If yes:
• When are results presented?• At time of visit?
• Where are results presented?• Part of workflow?
• How are results presented?• Numeric or graphical presentation

Data entry• How will data be entered?• Depends on mode of administration

Interpreting and responding to scores
• Algorithms (Asthma APGAR)• Meaningful scores (ACT)• Linking to clinical guidelines

Evaluation• Plans for evaluating use of tool on:
• Process/workflow• Quality of care

Barriers• Clinicians
– Lack of familiarity with the instruments– Doubt about the ability of pros to modify outcomes– Time and resource constraints– Disagreements over impact on patient-clinician relationship
• Patients – Literacy– Being too sick to complete questionnaires– Concern about impact on relationship with clinician
• Health system – Reimbursement– Fit within the clinical workflow

Anticipated barriers• Generate list of perceived barriers and
potential solutions

Process for selecting a tool and an implementation strategy• Provider meetings?• IT conversations?• Decision making?• Trainings?

Organization Worksheet• Walks through the different issues and
processes discussed today• To be completed by organization, with
assistance from PEC liaison• Weekly phone calls with PEC liaison

Proposed Timeline - 2011
Explore options for asthma
PROs
Discuss PRO with provider
groups
Select asthma PRO tool
Make implementation plan for asthma
PRO tool
Create infrastructure for PRO tool deployment (e.g., EHR
template, iPad purchase &
configuration)
PRO tool training
Begin using asthma PRO
tool
March
April May June July Sept Oct