Embed Size (px)
Citation preview
Peptic Ulcer DiseasePeptic Ulcer Disease
Byron Cryer, MDByron Cryer, MD
Dallas VA Medical CenterDallas VA Medical Center
University of Texas Southwestern Medical University of Texas Southwestern Medical SchoolSchool

H . pyloriH . pylori eradication should confer a benefit in all eradication should confer a benefit in all of the following diseases of the following diseases exceptexcept::
1. Active gastric ulcer
2. Past history of duodenal ulcer
3. GERD
4. MALT Lymphoma
Question 1
Question 2Question 2 Which of the following agent (s) are effective in
decreasing NSAID ulcer complications (such as bleeding, perforation, and gastric outlet obstruction) in patients with rheumatoid arthritis?
(A) H2-receptor antagonists
(B) Sucralfate(C) Proton-pump inhibitors(D) Misoprostol(E) All of the above
H2-blockers are likely to be effective in which H2-blockers are likely to be effective in which situation?situation?
1. Treatment of bleeding ulcer2. Reduction of requirement for blood
transfusion after endoscopic treatment of ulcers
3. In combination with clarithromycin and amoxcillin for H. pylori eradication
4. Treatment of MALT Lymphoma5. None of the above
Question 3

Differential Diagnosis of DyspepsiaDifferential Diagnosis of Dyspepsia•Peptic Ulcer DiseasePeptic Ulcer Disease•Related to infection with Related to infection with Helicobacter pyloriHelicobacter pylori•Related to use of nonsteroidal anti-inflammatory drugsRelated to use of nonsteroidal anti-inflammatory drugs
•Gastroesophageal reflux disease (GERD)Gastroesophageal reflux disease (GERD)
•Biliary tract diseaseBiliary tract disease•CholelithiasisCholelithiasis•CholecystitisCholecystitis
•PancreatitisPancreatitis
•CancerCancer
•Nonulcer dyspepsiaNonulcer dyspepsia
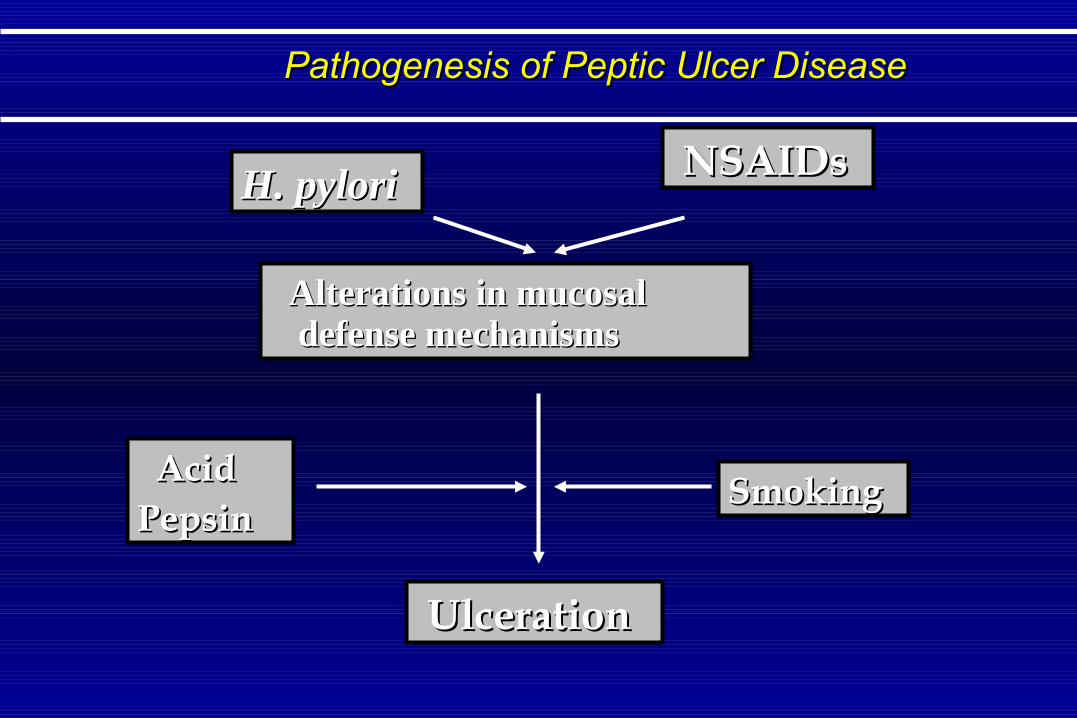
Pathogenesis of Peptic Ulcer DiseasePathogenesis of Peptic Ulcer Disease
H. pyloriH. pylori NSAIDsNSAIDs
Alterations in mucosal Alterations in mucosal defense mechanismsdefense mechanisms
UlcerationUlceration
SmokingSmoking AcidAcidPepsinPepsin
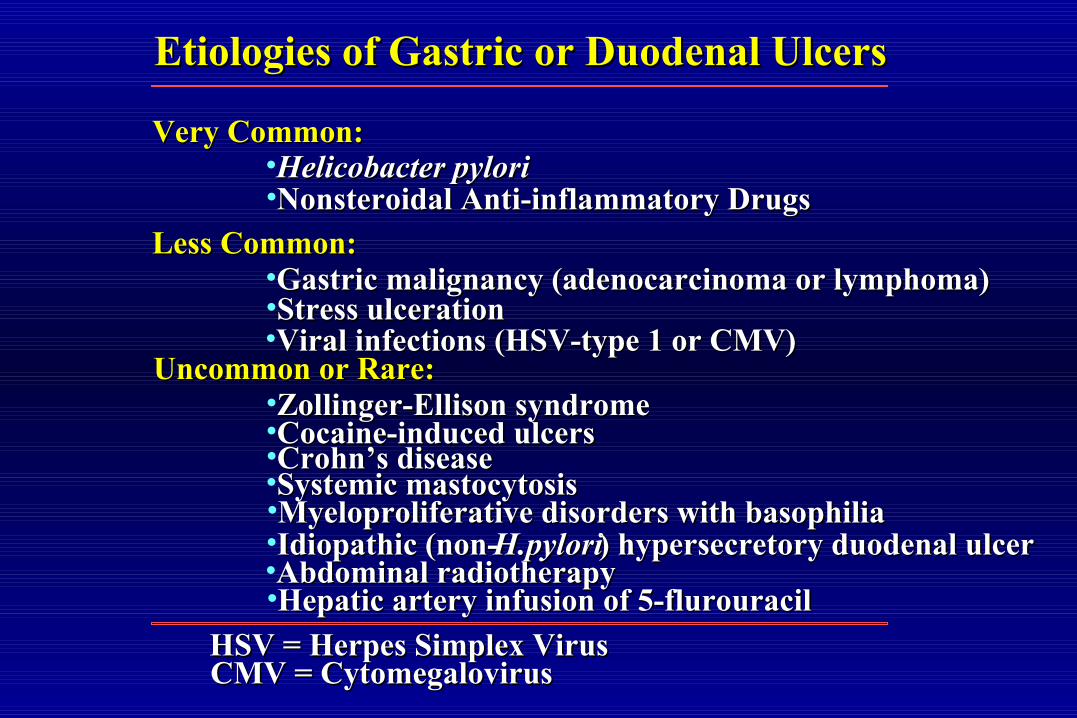
Etiologies of Gastric or Duodenal UlcersEtiologies of Gastric or Duodenal Ulcers
Very Common:Very Common:•Helicobacter pyloriHelicobacter pylori•Nonsteroidal Anti-inflammatory DrugsNonsteroidal Anti-inflammatory Drugs
Less Common:Less Common:•Gastric malignancy (adenocarcinoma or lymphoma)Gastric malignancy (adenocarcinoma or lymphoma)•Stress ulcerationStress ulceration•Viral infections (HSV-type 1 or CMV)Viral infections (HSV-type 1 or CMV)
Uncommon or Rare:Uncommon or Rare:•Zollinger-Ellison syndromeZollinger-Ellison syndrome•Cocaine-induced ulcersCocaine-induced ulcers•CrohnCrohn’s disease’s disease•Systemic mastocytosisSystemic mastocytosis•Myeloproliferative disorders with basophiliaMyeloproliferative disorders with basophilia•Idiopathic (non-Idiopathic (non- H.pyloriH.pylori) hypersecretory duodenal ulcer) hypersecretory duodenal ulcer•Abdominal radiotherapyAbdominal radiotherapy•Hepatic artery infusion of 5-flurouracilHepatic artery infusion of 5-flurouracil
HSV = Herpes Simplex VirusHSV = Herpes Simplex VirusCMV = CytomegalovirusCMV = Cytomegalovirus

Helicobacter pyloriHelicobacter pylori
• Most common human bacterial infectionMost common human bacterial infection• Infection is life longInfection is life long• Elicits a robust inflammatory responseElicits a robust inflammatory response• Associated with:Associated with:
Asymptomactic, healthy individualsAsymptomactic, healthy individualsPeptic Ulcer DiseasePeptic Ulcer DiseaseAtrophic GastritisAtrophic GastritisGastric AdenocarcinomaGastric AdenocarcinomaGastric LymphomaGastric Lymphoma
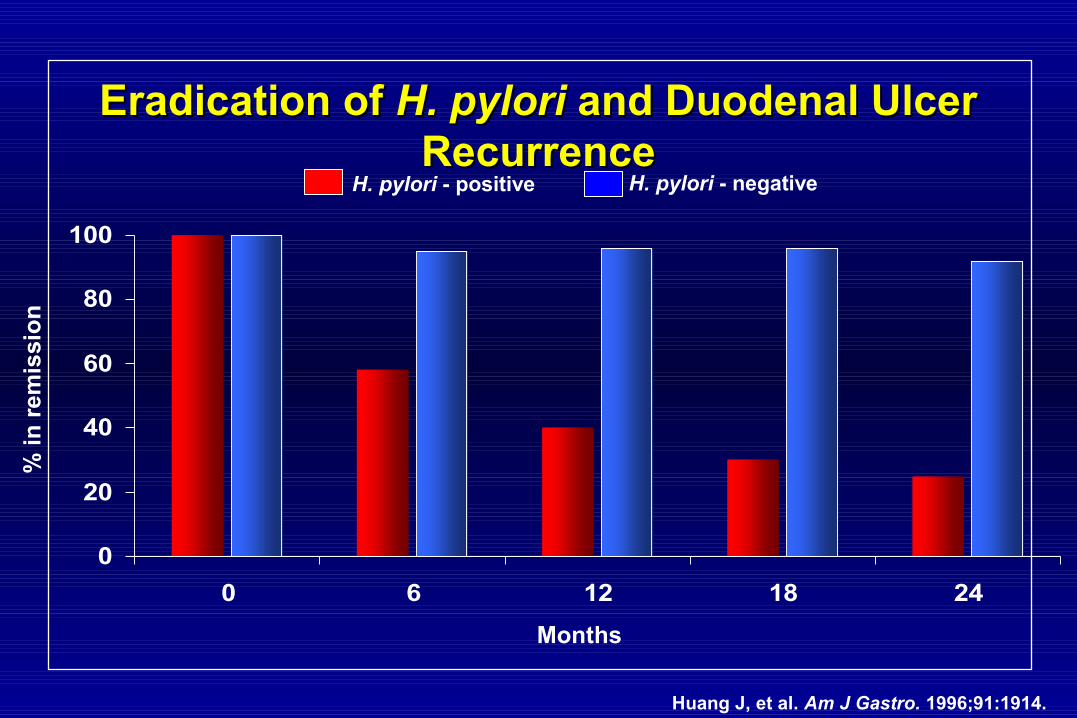
Eradication of Eradication of H. pyloriH. pylori and Duodenal Ulcer and Duodenal Ulcer RecurrenceRecurrence
Huang J, et al. Am J Gastro. 1996;91:1914.
0
20
40
60
80
100
0 6 12 18 24
% i
n r
emis
sio
n
Months
H. pylori - positive H. pylori - negative

Relationship of Relationship of H. pylori H. pylori to Gastric Cancerto Gastric Cancer
H. pyloriH. pylori
Chronic Active Superficial GastritisChronic Active Superficial Gastritis
Chronic Atrophic GastritisChronic Atrophic Gastritis
Chronic Atrophic Gastritis Chronic Atrophic Gastritis with Intestinal Metaplasiawith Intestinal Metaplasia
DysplasiaDysplasia
Gastric AdenocarcinomaGastric Adenocarcinoma
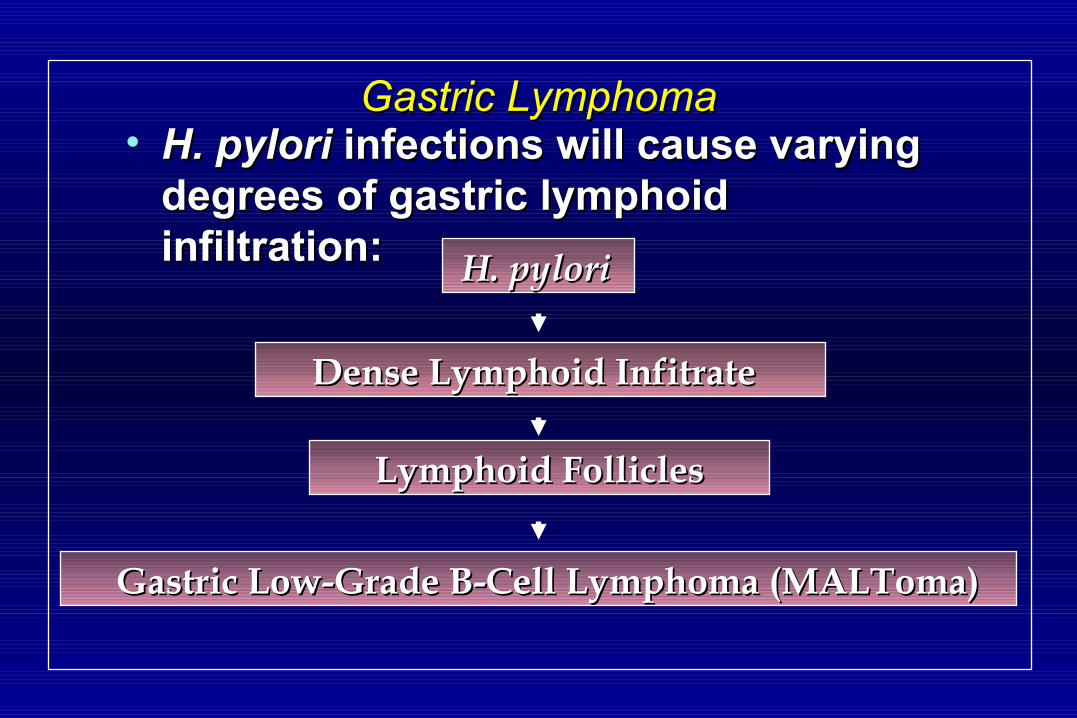
Gastric LymphomaGastric Lymphoma• H. pyloriH. pylori infections will cause varying infections will cause varying
degrees of gastric lymphoid degrees of gastric lymphoid infiltration:infiltration: H. pyloriH. pylori
Dense Lymphoid InfitrateDense Lymphoid Infitrate
Lymphoid FolliclesLymphoid Follicles
Gastric Low-Grade B-Cell Lymphoma (MALToma)Gastric Low-Grade B-Cell Lymphoma (MALToma)
What is the Relationship Between What is the Relationship Between H. pyloriH. pylori and Functional Dyspepsia?and Functional Dyspepsia?
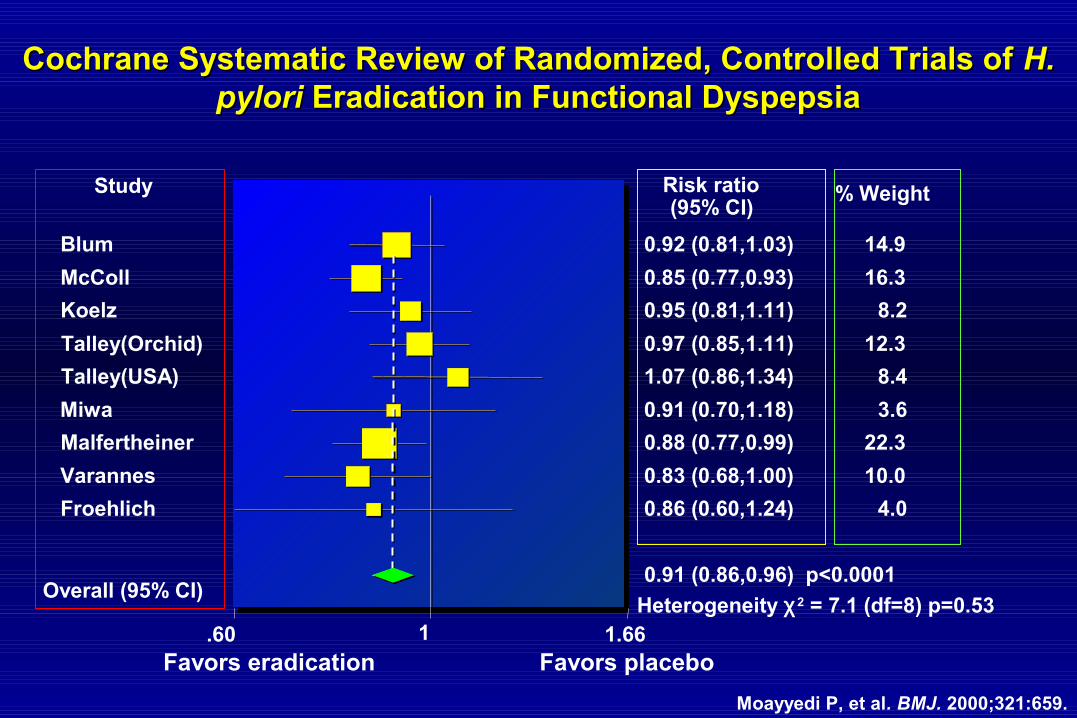
Cochrane Systematic Review of Randomized, Controlled Trials of Cochrane Systematic Review of Randomized, Controlled Trials of H. H. pyloripylori Eradication in Functional Dyspepsia Eradication in Functional Dyspepsia
.60 1 1.66
Study % Weight Risk ratio (95% CI)
0.92 (0.81,1.03) Blum 14.9
0.85 (0.77,0.93) McColl 16.3
0.95 (0.81,1.11) Koelz 8.2
0.97 (0.85,1.11) Talley(Orchid) 12.3
1.07 (0.86,1.34) Talley(USA) 8.4
0.91 (0.70,1.18) Miwa 3.6
0.88 (0.77,0.99) Malfertheiner 22.3
0.83 (0.68,1.00) Varannes 10.0
0.86 (0.60,1.24) Froehlich 4.0
0.91 (0.86,0.96) p<0.0001 Overall (95% CI)
Favors eradication Favors placebo
Heterogeneity χ2 = 7.1 (df=8) p=0.53
Moayyedi P, et al. BMJ. 2000;321:659.
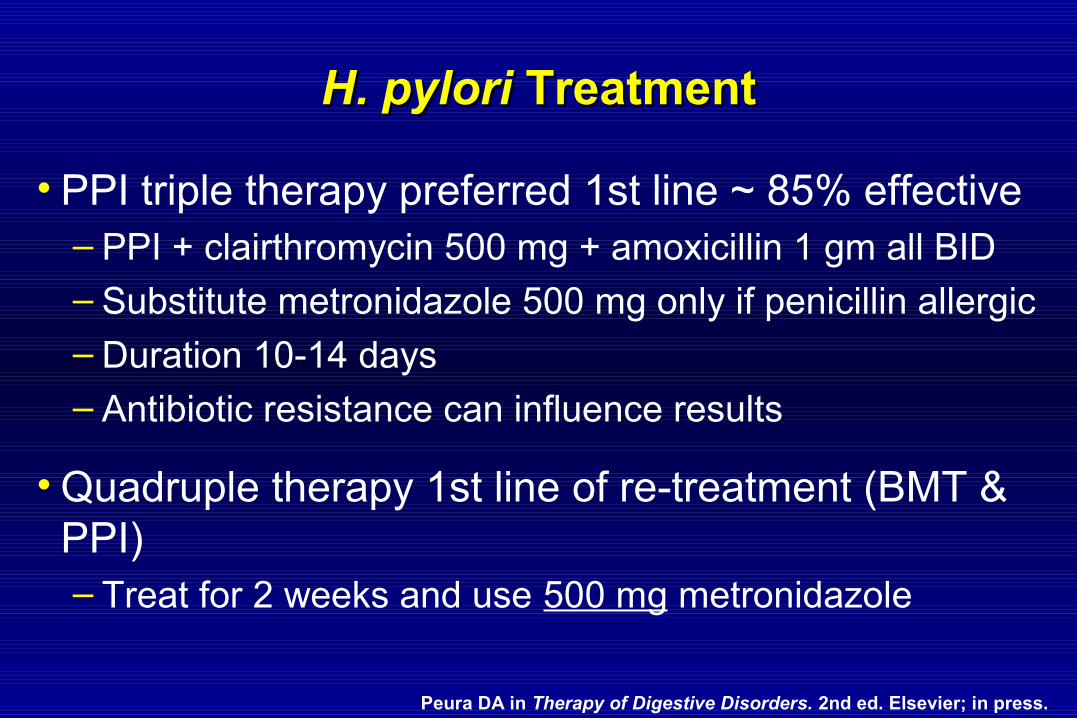
H. pyloriH. pylori Treatment Treatment
• PPI triple therapy preferred 1st line ~ 85% effective– PPI + clairthromycin 500 mg + amoxicillin 1 gm all BID
– Substitute metronidazole 500 mg only if penicillin allergic– Duration 10-14 days– Antibiotic resistance can influence results
• Quadruple therapy 1st line of re-treatment (BMT & PPI)– Treat for 2 weeks and use 500 mg metronidazole
Peura DA in Therapy of Digestive Disorders. 2nd ed. Elsevier; in press.
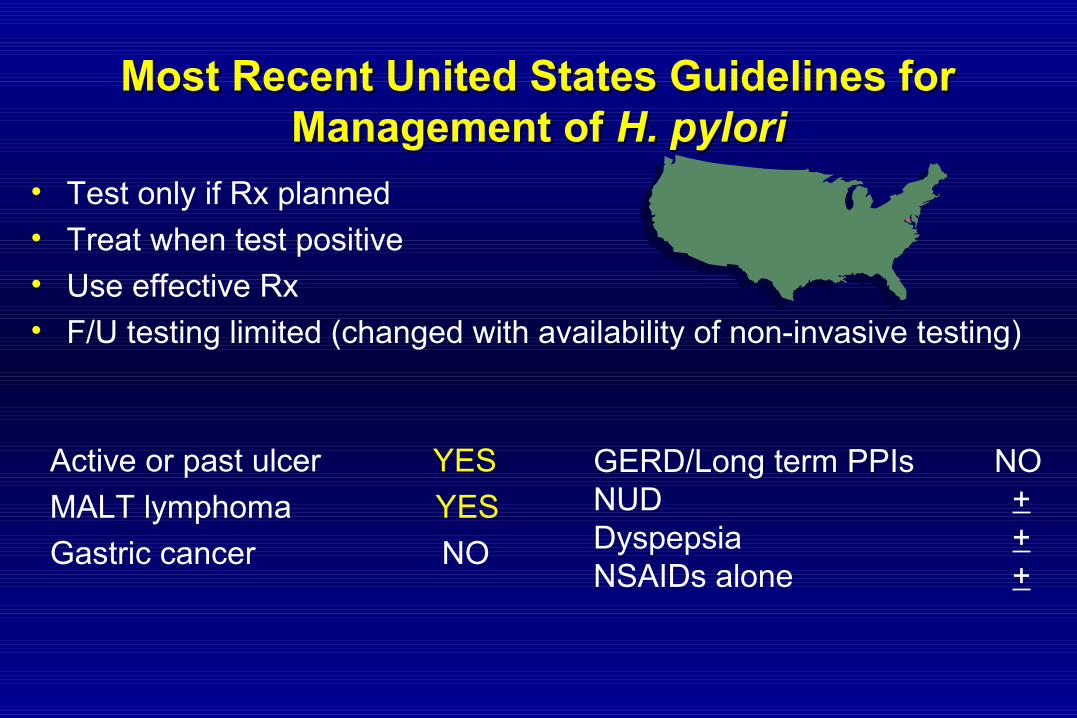
Most Recent United States Guidelines for Most Recent United States Guidelines for Management of Management of H. pyloriH. pylori
• Test only if Rx planned
• Treat when test positive• Use effective Rx• F/U testing limited (changed with availability of non-invasive testing)
Active or past ulcer YES
MALT lymphoma YES
Gastric cancer NO
GERD/Long term PPIs NONUD +Dyspepsia +NSAIDs alone +

Spectrum of NSAID-InducedSpectrum of NSAID-InducedGI Mucosal InjuryGI Mucosal Injury
Upper GIUpper GI• • GERD GERD • • Subepithelial petechialSubepithelial petechial
hemorrhages hemorrhages• • ErosionsErosions• • UlcersUlcers
– – Stomach > duodenumStomach > duodenum
• • BleedingBleeding
– – Stomach Stomach ≈≈ duodenum duodenum
• • Perforations/obstruction
Small IntestineSmall Intestine•• UlcersUlcers
• • StricturesStrictures• • DiaphragmsDiaphragms• • EnteropathyEnteropathy
ColonColon
•• ColitisColitis
• • UlcersUlcers
• • StricturesStrictures
• • Diverticular bleedDiverticular bleed
or perforation or perforation
• • CollagenousCollagenous
colitis colitis
• • Relapse of IBDRelapse of IBD
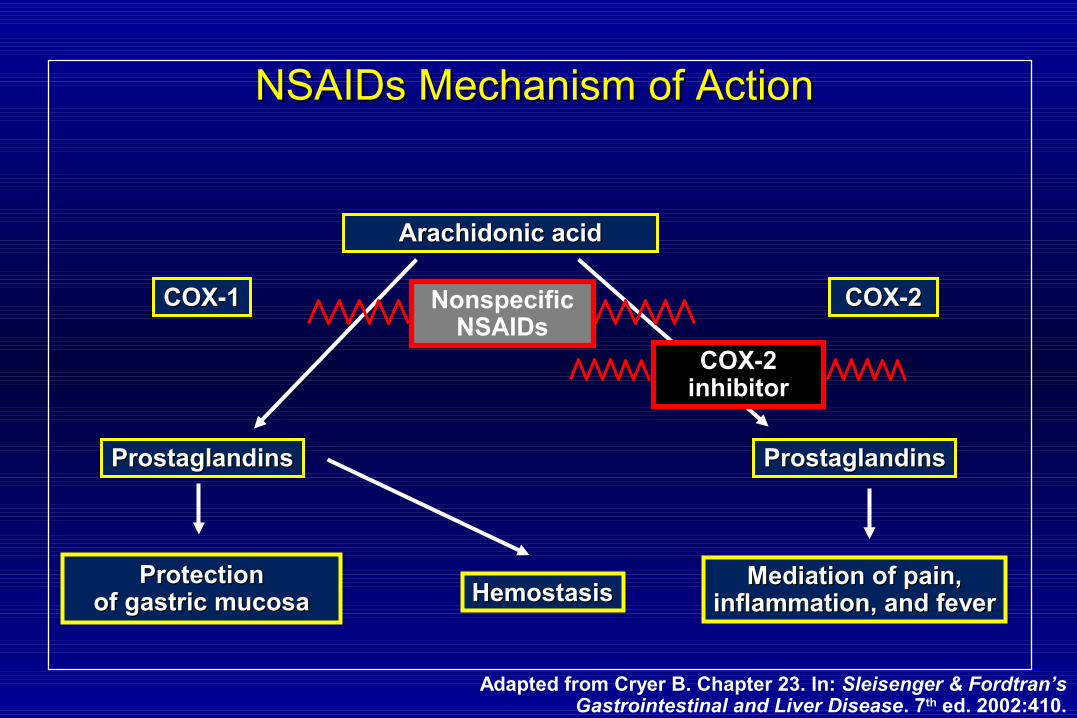
COX-1COX-1 COX-2COX-2
ProstaglandinsProstaglandins ProstaglandinsProstaglandins
Arachidonic acidArachidonic acid
ProtectionProtectionof gastric mucosaof gastric mucosa HemostasisHemostasis
Mediation of pain,Mediation of pain,inflammation, and feverinflammation, and fever
COX-2 inhibitor
Nonspecific NSAIDs
NSAIDs Mechanism of ActionNSAIDs Mechanism of Action
Adapted from Cryer B. Chapter 23. In: Sleisenger & Fordtran’s Gastrointestinal and Liver Disease. 7th ed. 2002:410.

Endoscopic Photograph of GastropathyEndoscopic Photograph of Gastropathy
Endoscopic PhotographEndoscopic Photographof Gastric Ulcerof Gastric Ulcer
SSTRATEGIESTRATEGIES FORFOR T TREATINGREATING NSAID-INSAID-INDUCEDNDUCED U ULCERSLCERS
• Discontinue NSAID
• Heal ulcer with acid suppression1,2
• Prevent ulcer recurrence2
– Eradicate Helicobacter pylori if present– GI prophylaxis if NSAIDs continued– Consider use of COX-2 specific inhibitor
or non-NSAID analgesic1. Scheiman. Curr Treatment Options Gastroenterol. 1999;2:205–213.2. Wolfe, et al. N Engl J Med. 1999;340:1888–1899.
Prevention of Ulcer DiseasePrevention of Ulcer Disease
High Risk PatientsHigh Risk Patients Prophylaxis TreatmentProphylaxis TreatmentHistory of peptic ulcerHistory of peptic ulcer MisoprostolMisoprostol::Concomitant anticoagulantConcomitant anticoagulant 100 100 µµg BID, advance tog BID, advance toConcomitant corticosteroidsConcomitant corticosteroids 200 200 µµg BID as tolerated g BID as tolerated
Significant co-morbiditiesSignificant co-morbiditiesHigh doses of NSAIDsHigh doses of NSAIDs Proton Pump InhibitorProton Pump Inhibitor::Combinations of > 1 NSAIDCombinations of > 1 NSAIDOlder Age ( i.e., > 75 y.o.)Older Age ( i.e., > 75 y.o.) COX-2 InhibitorCOX-2 Inhibitor
Low Risk PatientsLow Risk Patients No prophylaxis neededNo prophylaxis needed
NSAIDsNSAIDs• The decision for prophylaxis against NSAID-induced ulcer The decision for prophylaxis against NSAID-induced ulcer
needs to be made at the time the NSAID is started.needs to be made at the time the NSAID is started.
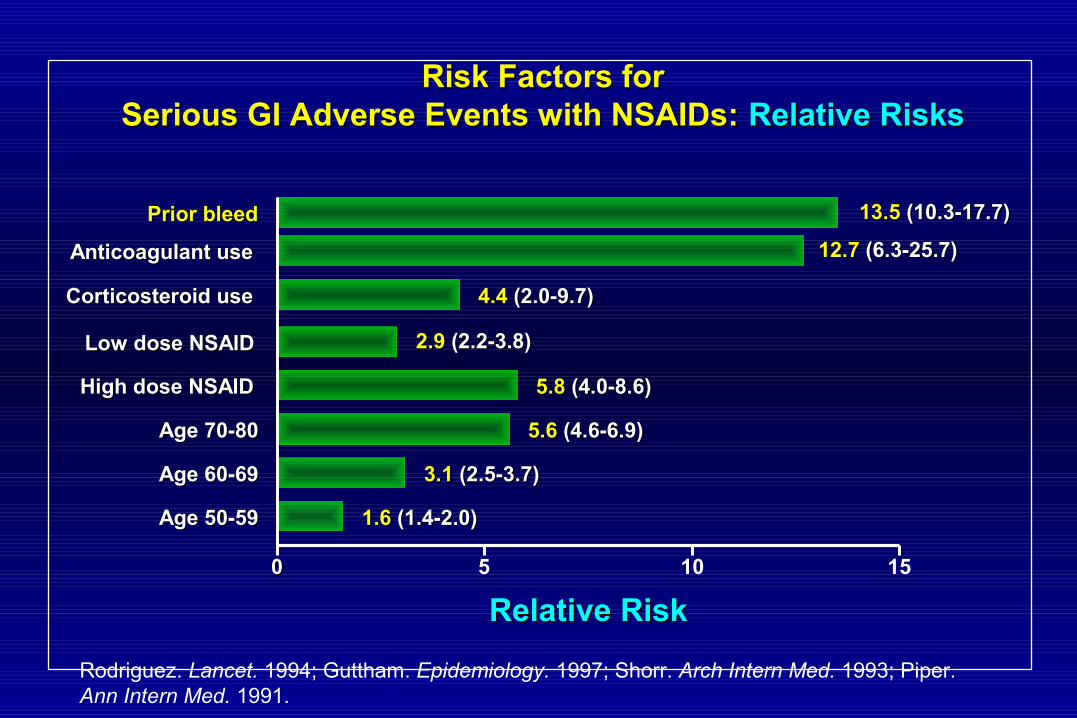
Risk Factors forRisk Factors forSerious GI Adverse Events with NSAIDs:Serious GI Adverse Events with NSAIDs: Relative RisksRelative Risks
Rodriguez. Lancet. 1994; Guttham. Epidemiology. 1997; Shorr. Arch Intern Med. 1993; Piper. Ann Intern Med. 1991.
00 5 10 15
4.44.4 (2.0-9.7) (2.0-9.7)
12.712.7 (6.3-25.7) (6.3-25.7)
2.92.9 (2.2-3.8) (2.2-3.8)
5.85.8 (4.0-8.6) (4.0-8.6)
5.65.6 (4.6-6.9) (4.6-6.9)
3.13.1 (2.5-3.7) (2.5-3.7)
1.61.6 (1.4-2.0) (1.4-2.0)
13.513.5 (10.3-17.7) (10.3-17.7)
Corticosteroid useCorticosteroid use
Anticoagulant useAnticoagulant use
Low dose NSAIDLow dose NSAID
High dose NSAIDHigh dose NSAID
Age 70-80Age 70-80
Age 60-69Age 60-69
Age 50-59Age 50-59
Prior bleedPrior bleed
Relative RiskRelative Risk

4.96.4
0
5
10
15
20
25
30
35
% r
e-b
leed
at
6-m
on
ths
19
26
0
5
10
15
20
25
30
35
6-m
on
th c
um
ula
tive
in
cid
ence
of
ulc
er (
%)
p = NS
p = NS
n = n = 143 144 116 106
Prevention of Recurrent Ulcer Bleeding in High Risk PatientsPrevention of Recurrent Ulcer Bleeding in High Risk Patients
Celecoxib 200 mg BID + placeboDiclofenac 75 mg BID + Omeprazole 20 mg QD
INITIAL STUDY GROUP 1 FOLLOW-UP STUDY GROUP 2
1Chan et al. N Engl J Med. 2002;347:2104.2Chan et al. DDW. 2004;A103404.
Patients with prior ulcer bleed on NSAID; ulcer healed and H. pylori – negative or eradicated prior to randomization

0.20.2
0.40.4
0.60.6
0.80.8
1.01.0
All PatientsAll Patients NSAID Naïve PatientsNSAID Naïve Patients00
1.21.2
Patients Not Taking AspirinPatients Not Taking Aspirin
0.50.5
1.01.0
1.51.5
2.02.0
All PatientsAll Patients NSAID Naïve PatientsNSAID Naïve Patients00
Patients Taking AspirinPatients Taking Aspirin
2.52.5
p = 0.68p = 0.68
p < 0.05p < 0.05
p = 0.97p = 0.97
p < 0.05p < 0.05
5/22105/2210
19/252619/2526
3/13733/1373
16/159716/1597
6/3296/3299/5839/583
5/3675/3678/5208/520
An
nu
aliz
ed i
nci
den
ce,
%A
nn
ual
ized
in
cid
ence
, %
An
nu
aliz
ed i
nci
den
ce,
%A
nn
ual
ized
in
cid
ence
, %
AA
BB
EtodolacEtodolacNaproxenNaproxen
EtodolacEtodolacNaproxenNaproxen
Rates of Clinically Significant Upper GI Events Rates of Clinically Significant Upper GI Events
Weideman RA et al. Gastroenterology 2004;127:1322-1328Weideman RA et al. Gastroenterology 2004;127:1322-1328
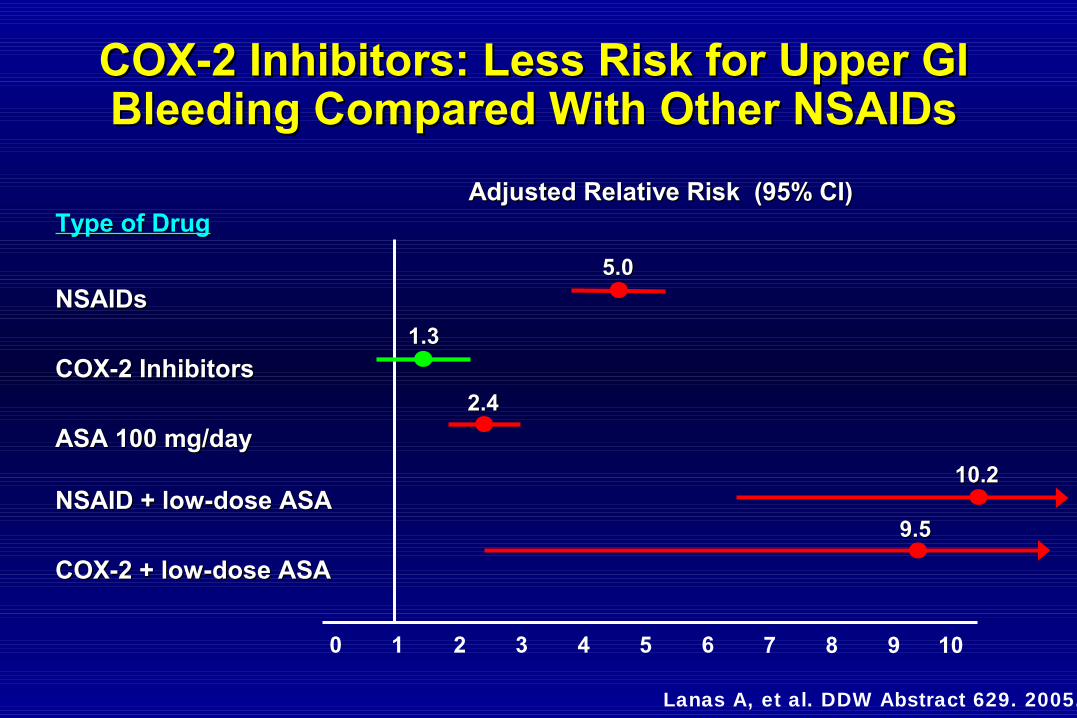
10.210.2
0 1 2
Type of DrugType of Drug
NSAIDsNSAIDs
COX-2 InhibitorsCOX-2 Inhibitors
ASA 100 mg/dayASA 100 mg/day
NSAID + low-dose ASANSAID + low-dose ASA
COX-2 + low-dose ASACOX-2 + low-dose ASA
Adjusted Relative Risk (95% CI)Adjusted Relative Risk (95% CI)
5.05.0
3 4 5 6 7 8 9
1.31.3
2.42.4
9.59.5
COX-2 Inhibitors: Less Risk for Upper GI COX-2 Inhibitors: Less Risk for Upper GI Bleeding Compared With Other NSAIDsBleeding Compared With Other NSAIDs
Lanas A, et al. DDW Abstract 629. 2005.
10

Anti-Platelet TherapiesAnti-Platelet Therapies
• AspirinAspirin
• ADP Receptor AntagonistsADP Receptor AntagonistsClopidogrel (Plavix)Clopidogrel (Plavix)Ticlopidine (Ticlid)Ticlopidine (Ticlid)
• Glycoprotein IIb / IIIa InhibitorsGlycoprotein IIb / IIIa InhibitorsTicofiban (Aggrastat)Ticofiban (Aggrastat)Abciximab (ReoPro)Abciximab (ReoPro)Eptifibatid (Integrilin)Eptifibatid (Integrilin)
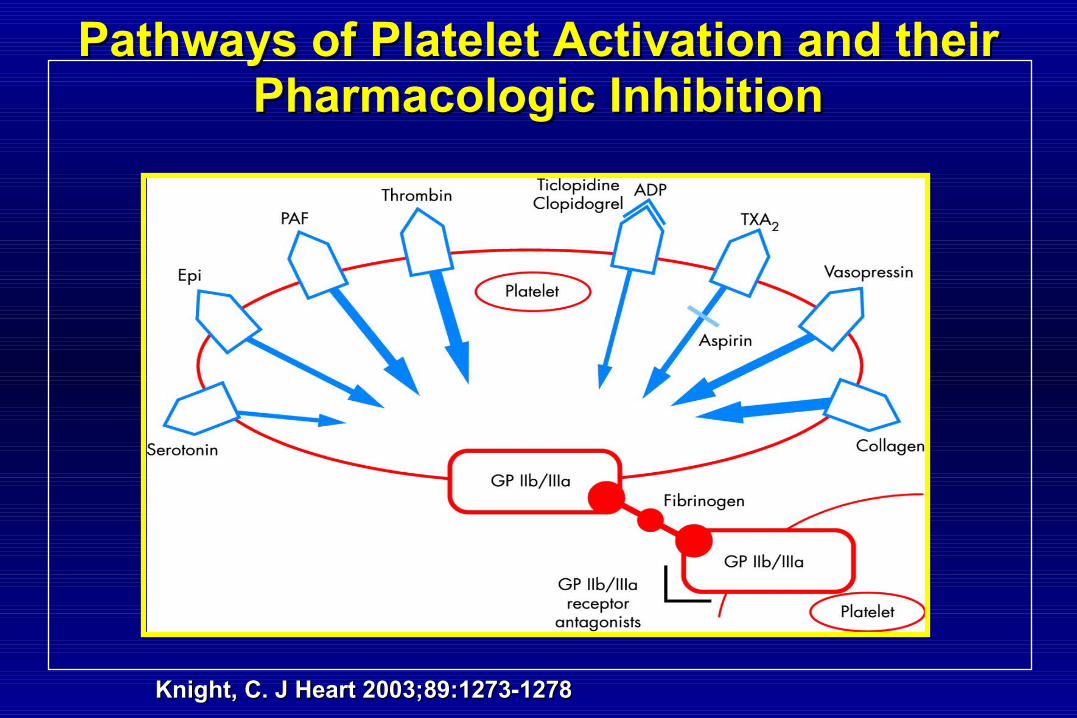
Knight, C. J Heart 2003;89:1273-1278Knight, C. J Heart 2003;89:1273-1278
Pathways of Platelet Activation and their Pathways of Platelet Activation and their Pharmacologic InhibitionPharmacologic Inhibition
Clopidogrel vs. Aspirin plus PPIClopidogrel vs. Aspirin plus PPIfor Prevention of Upper GI Bleedingfor Prevention of Upper GI Bleeding
• 320 pts with history of bleeding ulcer320 pts with history of bleeding ulcer• All All H. pyloriH. pylori negative negative• Randomized to:Randomized to:
– Clopidogrel 75 mg daily (n=161)Clopidogrel 75 mg daily (n=161)– Aspirin + esomeprazole 20 mg BID (n=159)Aspirin + esomeprazole 20 mg BID (n=159)
• Followed for 12-months for rates of recurrent major Followed for 12-months for rates of recurrent major GI bleeding (upper and lower GI tract)GI bleeding (upper and lower GI tract)
Chan, F. K.L. et al. N Engl J Med 2005;352:238-244Chan, F. K.L. et al. N Engl J Med 2005;352:238-244
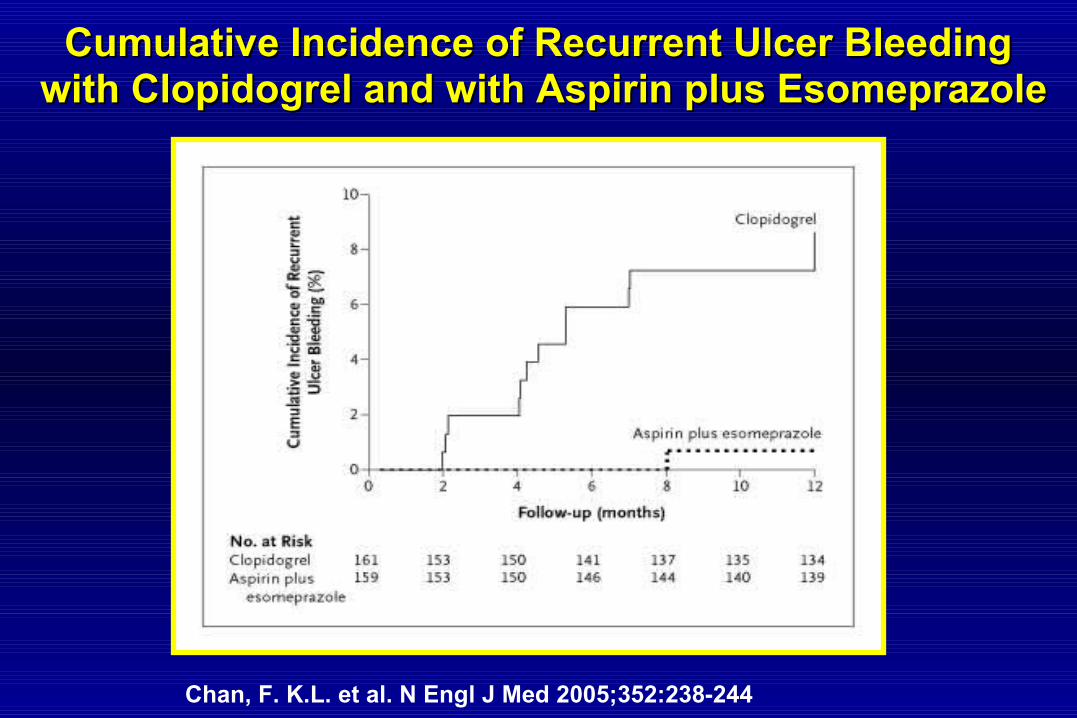
Chan, F. K.L. et al. N Engl J Med 2005;352:238-244
Cumulative Incidence of Recurrent Ulcer BleedingCumulative Incidence of Recurrent Ulcer Bleeding with Clopidogrel and with Aspirin plus Esomeprazolewith Clopidogrel and with Aspirin plus Esomeprazole
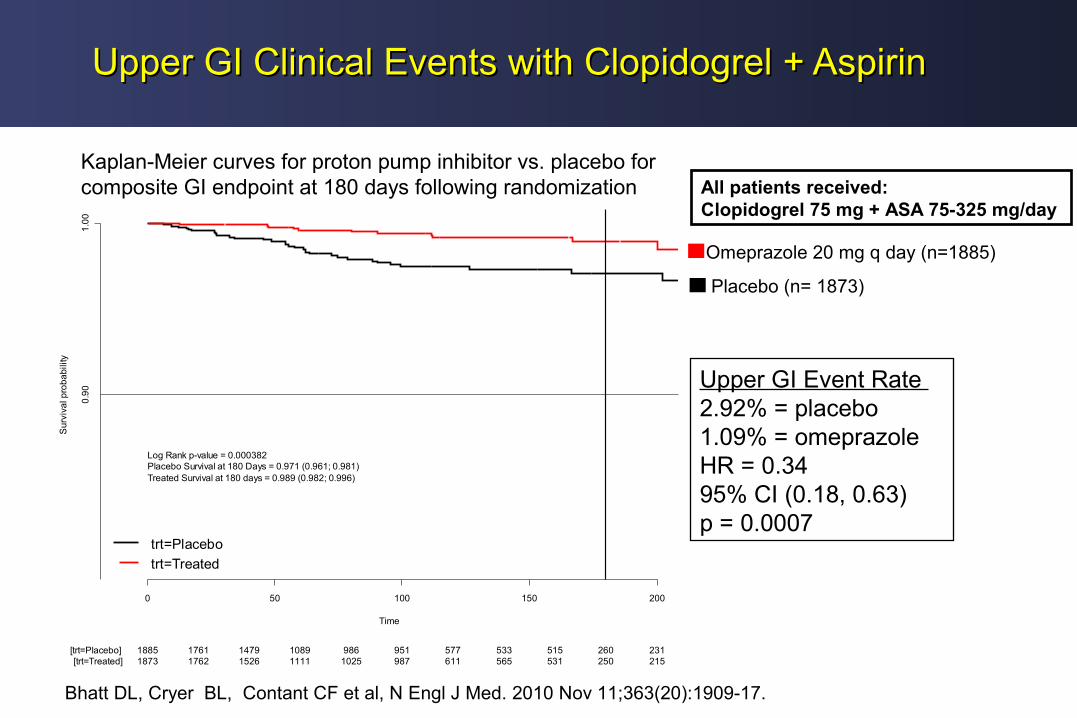
Upper GI Clinical Events with Clopidogrel + AspirinUpper GI Clinical Events with Clopidogrel + Aspirin
Percent with Ulcer
Hsu et al., DDW 2010
Time
Sur
viva
l pro
babi
lity
0 50 100 150 200
1.0
0
1885 1761 1479 1089 986 951 577 533 515 260 231[trt=Placebo]1873 1762 1526 1111 1025 987 611 565 531 250 215[trt=Treated]
trt=Placebo
trt=Treated
0.9
0
Log Rank p-value = 0.000382Placebo Survival at 180 Days = 0.971 (0.961; 0.981)Treated Survival at 180 days = 0.989 (0.982; 0.996)
Kaplan-Meier curves for proton pump inhibitor vs. placebo for composite GI endpoint at 180 days following randomization
Omeprazole 20 mg q day (n=1885)
Placebo (n= 1873)
All patients received:Clopidogrel 75 mg + ASA 75-325 mg/day
Bhatt DL, Cryer BL, Contant CF et al, N Engl J Med. 2010 Nov 11;363(20):1909-17.
Upper GI Event Rate 2.92% = placebo1.09% = omeprazoleHR = 0.3495% CI (0.18, 0.63)p = 0.0007
Alarm FeaturesAlarm Features(Indications for Early Endoscopy)(Indications for Early Endoscopy)
• New onset symptoms after age 50 yearsNew onset symptoms after age 50 years• AnorexiaAnorexia• DysphagiaDysphagia• Gross or occult gastrointestinal bleedingGross or occult gastrointestinal bleeding• Unexplained anemiaUnexplained anemia• Weight lossWeight loss• Significant vomitingSignificant vomiting• Upper GI barium study suspicious for cancerUpper GI barium study suspicious for cancer
Complicated UlcersComplicated Ulcers
Primary TherapiesPrimary Therapies:: Bleeding UlcersBleeding Ulcers Endoscopic TherapyEndoscopic Therapy
Perforated UlcersPerforated Ulcers Surgical TherapySurgical Therapy
Secondary TherapiesSecondary Therapies: : Medical TherapiesMedical Therapies::- H- H22-Receptor Antagonists-Receptor Antagonists
- Proton Pump Inhibitors- Proton Pump Inhibitors- - H. pylori H. pylori TreatmentsTreatments- NSAIDs / ASA- NSAIDs / ASA
Upper GI BleedingUpper GI Bleeding
GI Bleeding — Common CausesGI Bleeding — Common Causes
• Gastric or duodenal ulcer– Helicobacter pylori (H. pylori)– NSAIDs
• Erosive esophagitis• Mallory-Weiss tear• Esophageal or gastric varices• Arterio-venous malformation (AVM)• Stress gastropathy
Cook DJ, et al. N Engl J Med. 1998;338:791-797.Cook DJ, et al. Crit Care Med. 1999;27:2812-2817.
GI BleedGI Bleed
• Minor Bleeding– Hematemesis– ‘Coffee ground’ emesis– Hematochezia– Melena

GI BleedGI Bleed
• Major Bleeding = Minor Bleeding plus:– Decrease in systolic blood pressure > 20mm Hg– Heart rate increase > 20– Decrease in Hgb > 2g/dL in which transfusion
does not boost Hgb > 2g/dL
Cook DJ, et al. N Engl J Med. 1998;338:791-797.Cook DJ, et al. Crit Care Med. 1999;27:2812-2817.

Management of Upper GI BleedingManagement of Upper GI Bleeding
Prevention of:Stress gastropathy
Treatment of:Gastric or duodenal ulcer
Erosive esophagitis
Mallory-Weiss tear
Esophageal or gastric varices
AVM
Stress gastropathy

Stress Ulcer BleedingStress Ulcer Bleeding
• Patients admitted to an ICU demonstrate endoscopic evidence of GI damage within 24 hours of admission.
• Historically, GI bleeding occurs in approximately 15% of ICU patients without prophylactic therapy.
• Current, incidence of clinically significantly bleeding is 1.5% .
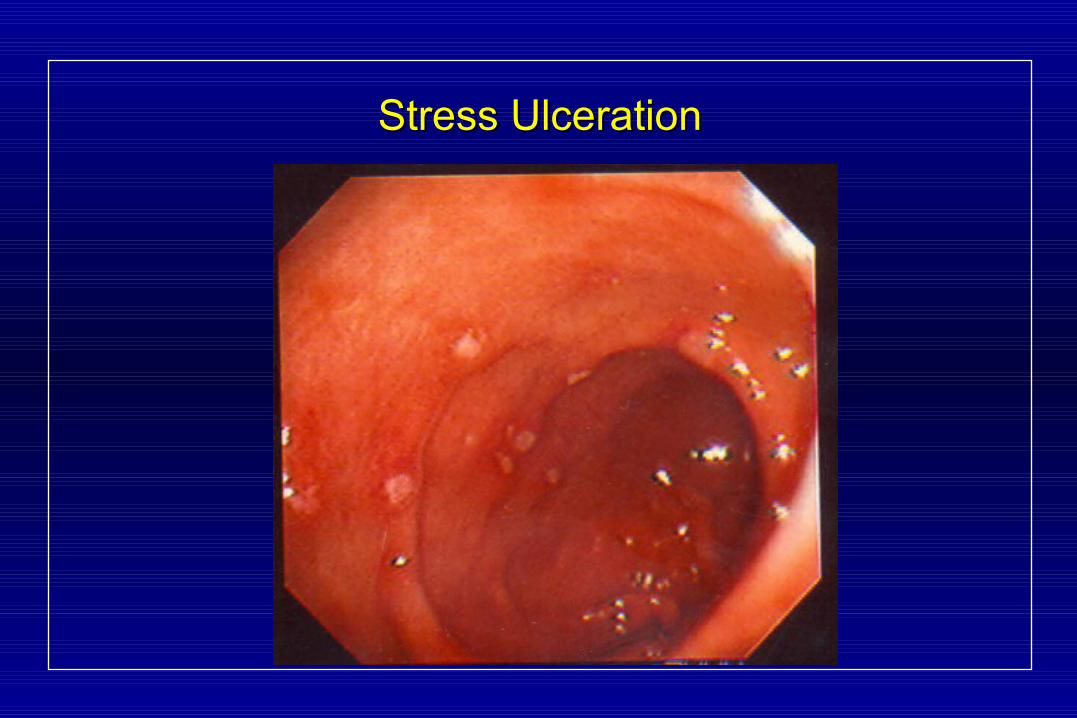
Stress UlcerationStress Ulceration
Risk Factors for Stress Ulcer Bleeding
Acute respiratory failure/mechanical vent patients (>48hrs) Coagulopathy Shock Severe burns (>30% BSA) Significant intracranial bleeding or trauma Spinal injury (immobilization >24 hrs) GI bleed within 12 weeks Multiple organ failure High dose corticosteroid therapy Long-term NSAID use
Cook DJ, et al. N.Engl. J Med. 1998;338:791-7.Cook DJ, et al. Crit Care Med. 1999;27:2812-7.
Management of Upper GI BleedingManagement of Upper GI Bleeding
Prevention of:Stress gastropathy
Treatment of:Gastric or duodenal ulcer
Erosive esophagitis
Mallory-Weiss tear
Esophageal or gastric varices
AVM
Stress gastropathy
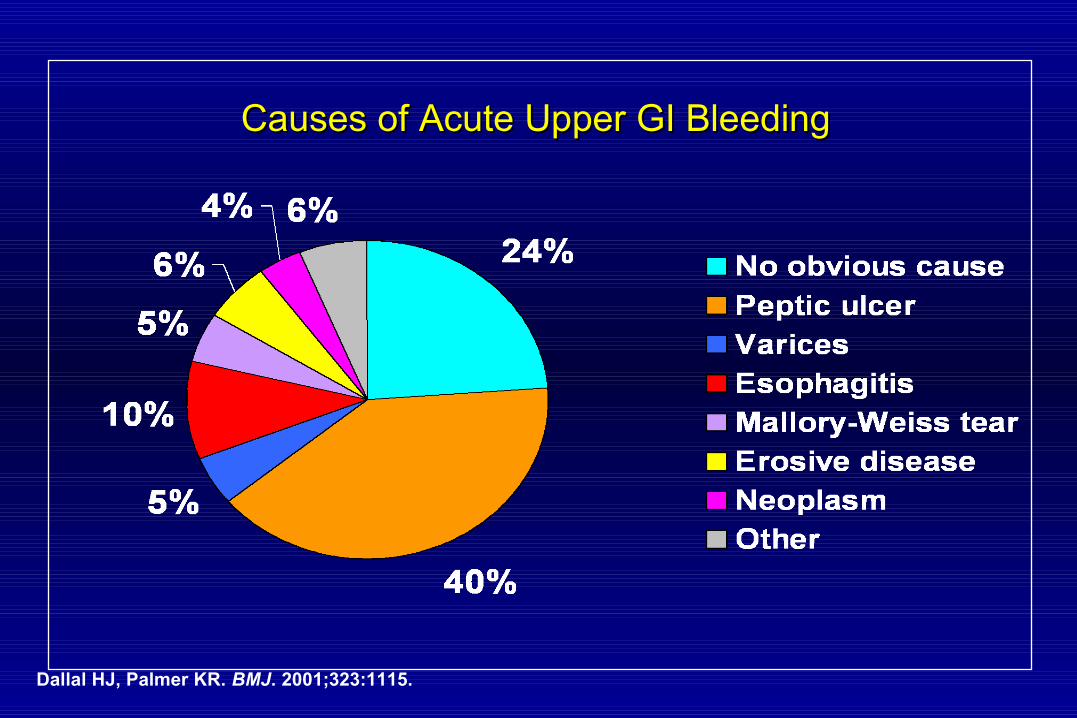
Causes of Acute Upper GI BleedingCauses of Acute Upper GI Bleeding
Dallal HJ, Palmer KR. BMJ. 2001;323:1115.
GI BleedingGI Bleeding
• Overall Management– Maintenance of hemodynamic stability– Nasogastric Lavage– Endoscopy with hemostasis– Blood products if necessary– Surgery if necessary – Antisecretory medications

Stigmata of Bleeding Stigmata of Bleeding Risks of Re-bleeding and PrevalenceRisks of Re-bleeding and Prevalence
Dot23%
Clot13%
Bleeder7%
NBVV8%
Clean base49%
0
10
20
30
40
50
60
Active bleeder NBVV Clot Dot Clean base
Ris
k o
f re
ble
edin
g (
%)
Adapted from Katschinski B et al. Dig Dis Sci 1994;39:706.
PREVALENCE
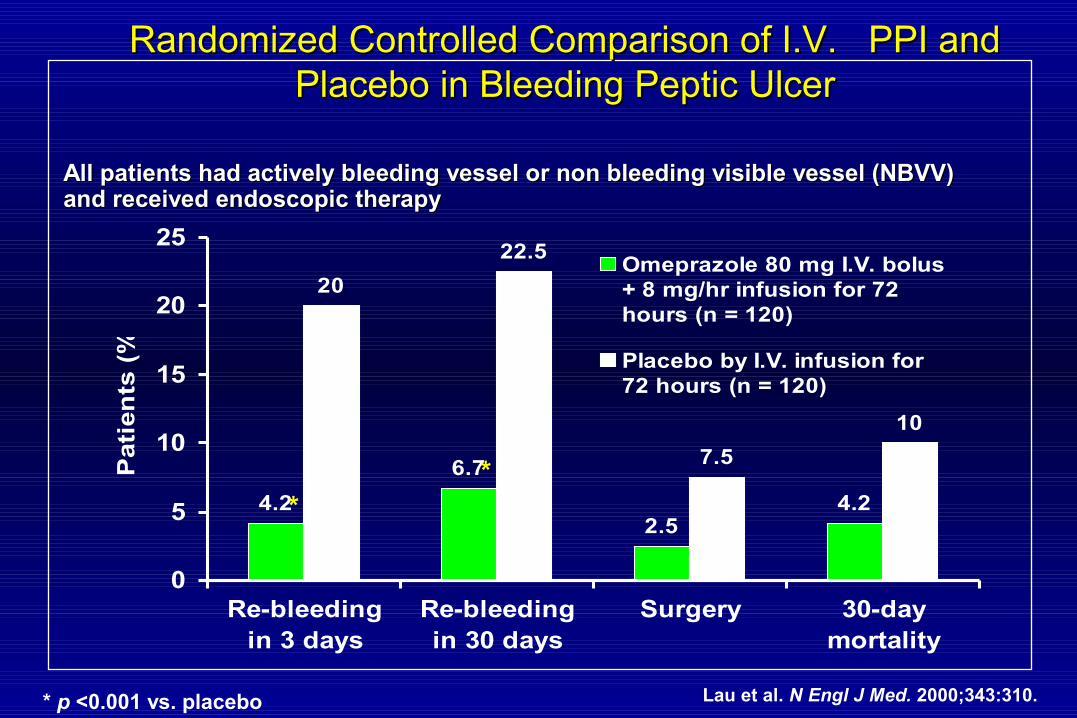
Randomized Controlled Comparison of I.V. PPI and Randomized Controlled Comparison of I.V. PPI and Placebo in Bleeding Peptic UlcerPlacebo in Bleeding Peptic Ulcer
4.2
6.7
2.54.2
20
22.5
7.5
10
0
5
10
15
20
25
Re-bleedingin 3 days
Re-bleedingin 30 days
Surgery 30-daymortality
Pati
en
ts (
%)
Omeprazole 80 mg I.V. bolus+ 8 mg/hr infusion for 72hours (n = 120)
Placebo by I.V. infusion for72 hours (n = 120)
Lau et al. N Engl J Med. 2000;343:310.
All patients had actively bleeding vessel or non bleeding visible vessel (NBVV) All patients had actively bleeding vessel or non bleeding visible vessel (NBVV) and received endoscopic therapyand received endoscopic therapy
**
* p <0.001 vs. placebo
H . pyloriH . pylori eradication should confer a benefit in all eradication should confer a benefit in all of the following diseases of the following diseases exceptexcept::
1. Active gastric ulcer
2. Past history of duodenal ulcer
3. GERD
4. MALT Lymphoma
Question 1
Question 2Question 2 Which of the following agent (s) are effective in
decreasing NSAID ulcer complications (such as bleeding, perforation, and gastric outlet obstruction) in patients with rheumatoid arthritis?
(A) H2-receptor antagonists
(B) Sucralfate(C) Proton-pump inhibitors(D) Misoprostol(E) All of the above
H2-blockers are likely to be effective in which H2-blockers are likely to be effective in which situation?situation?
1. Treatment of bleeding ulcer2. Reduction of requirement for blood
transfusion after endoscopic treatment of ulcers
3. In combination with clarithromycin and amoxcillin for H. pylori eradication
4. Treatment of MALT Lymphoma5. None of the above
Question 3

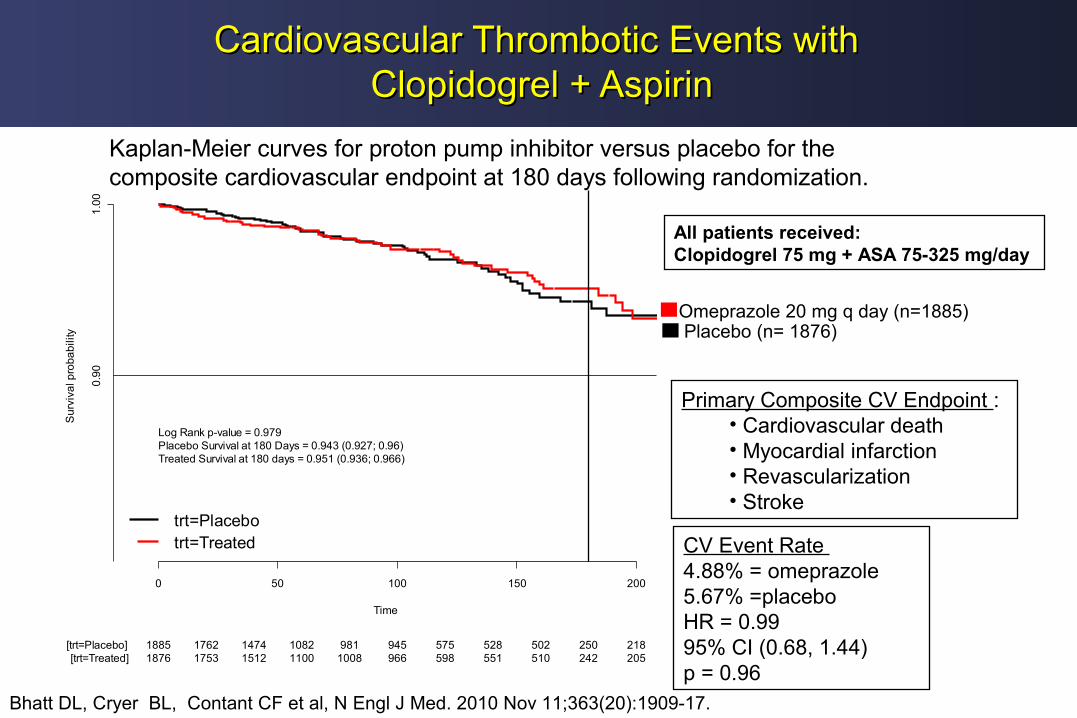
Cardiovascular Thrombotic Events with Cardiovascular Thrombotic Events with Clopidogrel + AspirinClopidogrel + Aspirin
Omeprazole 20 mg q day (n=1885) Placebo (n= 1876)
Time
Su
rviv
al p
roba
bili
ty
0 50 100 150 200
1.0
0
1885 1762 1474 1082 981 945 575 528 502 250 218[trt=Placebo]1876 1753 1512 1100 1008 966 598 551 510 242 205[trt=Treated]
trt=Placebotrt=Treated
0.9
0
Log Rank p-value = 0.979Placebo Survival at 180 Days = 0.943 (0.927; 0.96)Treated Survival at 180 days = 0.951 (0.936; 0.966)
Kaplan-Meier Plot of Cardiovascular Events by TreatmentKaplan-Meier curves for proton pump inhibitor versus placebo for the composite cardiovascular endpoint at 180 days following randomization.
All patients received:Clopidogrel 75 mg + ASA 75-325 mg/day
Bhatt DL, Cryer BL, Contant CF et al, N Engl J Med. 2010 Nov 11;363(20):1909-17.
Primary Composite CV Endpoint :• Cardiovascular death• Myocardial infarction• Revascularization• Stroke
CV Event Rate 4.88% = omeprazole 5.67% =placeboHR = 0.9995% CI (0.68, 1.44)p = 0.96