Plasma Cell Dyscrasias
Plasma Cell Dyscrasia+Multiple Choice QuestionsBy Mojgan
Talebian
Plasma Cell DyscrasiasFrom a single cell of B cell
lineageProliferation of monoclonal population of plasma
cellsProduction of a single type of immunoglobulin/immunoglobulin
fragmentHomogenous M protein in serum protein electrophoresis
2
Malignant Disordersof Plasma CellMultiple Myeloma
Macroglobulinemia
Heavy chain disease
Multiple Myeloma (MM)A Trial of: An abnormal proliferation of
plasma cells in the bone marrowOverproduction of monoclonal
immunoglobulinRelated tissue/organ impairment; lytic bone disease,
increased calcium ,renal insufficiency, anemia,Classification is
according to the type of Ig Mostly produce IgG or IgA, a few IgD
and IgEIgM production is rare, usually in Waldenstrm's
macroglobulinemiaMM variants:IgM myeloma; with the presence of
osteolytic lesionsBence-Jones myeloma; production of excess light
chains, dimers form of either or , in serum and urine
MM pathogenesisChronic progressive disorder, fatalthe median age
at the time of diagnosis 65; prevalence increase with aging
processMore in mengenetics; more common in primary relatives of the
patientOther potential risk factors:Exposure to large doses of
radiation, chemicalsChronic antigenic
exposuresArthritisOsteomyelitis
MM PathogenesisProduction of multiple tumors in the
boneSecretion of osteoclast activating factor by solid tumors in
the bone results in osteoporosis:Bone fractures, lytic bone
lesions: hypercalcemia Reduction in normal hemopoiesis; anemia,
neutropenia, and thrombocytopenia
Production of paraproteins; hyperviscosity, dilutional anemia,
hyponatremia, high ESR, and rouleaux formation
Reduction of normal Ig level; rise of the total serum globulin
and reduction of serum albumin
Easy bruising and bleeding due to interference with platelet
function
Amyloidosis; deposition of glycoprotein, amyloid in tissues and
organs
Proteinuria, renal tubular dysfunction, renal failure due to
excess light chain and paraprotein precipitationLight chains
filtered and reabsorbed by the renal tubules; damaging the
tubulesIncrease loss of amino acids, glucose and
electrolytesGranular or waxy casts
Plasma cell leukemia: if plasma cells presence in large number
in the peripheral blood
Chromosome abnormalitiesSeen in 30% to 40% of
patientsTranslocations; t(11;14) and t(4;14), t(14;16),
(q13;q32)Trisomy 3, 5, 7, 9 and 11 The worst prognosis: monosomy
13, 13q14 deletion, and hypodiploidy The most frequent abnormality:
translocations involving 14q32 (the site of heavy chain
locus)Hyperdiploidy and aneuploidy; plasma cells are bi- and
multi-nucleated
Clinical symptomsBone pain, bone fractures, skeletal
deformityCNS involvementAmyloidosisHypercalcemia: anorexia, nausea,
vomiting, constipation and dehydrationRenal dysfunction,
edemaHyperviscosity syndrome; purpura, bruises, nose bleeding,
headaches, and blurred vision
Laboratory FindingsMild to moderate reduction in
HemoglobinNormochromic normocytic anemiaRouleaux formation, blue
background stainHigh ESR over 100 mm/hr, (in light chain disease it
is normal or moderately increased)Decreased leukocyte number,
neutropeniaMild decrease in platelets numberFew number of plasma
cell in peripheral bloodHypercalcemia
Bone Marrow BM examinations: aspirate and biopsyDiffuse or
localized marrow infiltration, hypercellularityBM plasma cell
labeling index (% of dividing plasma cells), differentiate between
benign and malignant plasma cell, a major prognosis
factorPlasmacytosis; ranging from 10% to 100%Malignant plasma
cells: small and mature to large and immature and atypicalFlaming
plasma cells, red areas in the cytoplasm, associated with IgA
myeloma
Grey gelatinous bone marrow in advanced form of the disease
Myeloma Plasma cellsTwo variants:Mature:Eccentric nucleus with
coarse chromatin pattern, typical cartwheel appearance is not
apparentVery blue cytoplasm with perinuclear haloImmature:Finer
nucleus with prominent nucleoliMultinucleated cells; in the
advanced form of the disease and presence of hyperdiploidy and
aneuploidyMore cytoplasm but lighter with perinuclear halo,
vacuoles and Russell bodies (Mott cell)
MMBlood Chemistry and ElectrophoresisIncrease of plasma volume
and serum viscositySerum calcium, indicator of hypercalcemiaSerum
creatinine, indicator of renal functionIncreased total
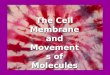
proteinDecreased albuminSerum protein electrophoresisSingle
homogeneous M-band, mostly in gamma or occasionally in beta
regionNo noticeable M-band in patients with light chain myeloma,
presence of light chain in Ig electrophoresisIn rare cases of
non-secretory myeloma: no M-band and no light chains fragments in
Pr or Ig electrophoresisDecreased gamma globulin
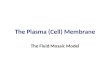
MM Bone Marrow
http://www.thrombocyte.com/causes-of-multiple-myeloma-cancer
13
MM Blood Chemistry and ElectrophoresisImmunoelectrophoresisThe
type of monoclonal IgThe class of heavy chainThe monoclonality
confirmation, single light chainOn concentrated urine sample to
identify Bence-Jones ProteinuriaThe heat precipitation of B-J
protein: solubility of B-J protein by slowly heating urine to 50 to
60 C, and reappearance of the Protein when the urine temperature
cools to below 60CThe test of choice is immunoelectrophoresisSerum
immunofixation test, to clarify if the monoclonal pattern is masked
by normal proteins
Serum Protein Electrophoresis
http://pleiad.umdnj.edu/~dweiss/pc/pcSerum_img.html
MM Staging
New International Staging SystemStage I: Serum 2 microglobulin
3.5 g/dlStage II: not stage I or IIISerum 2 microglobulin 5.5
mg/L
Grippe PR et all : international staging system for multiple
myeloma J Clin Oncol 23: 3412, 2005HemoglobinCorrected serum
CalciumLytic bone lesionsM-SpikeMedial survivalStage I>100 g/L70
g/LIgA >50 g/LUrine light chain > 12 g / 24 hrs23 monthsType
A. Serum creatinine < 2.0 mg/dL (0.18 mmol/L)Type B. Serum
creatinine > 2.0 mg/dL (0.18 mmol/L)
MM Clinical PresentationSign and SymptomsLaboratory
findingsRadiographic FeaturesBone MarrowBone painFatigueWeight
lossRecurrent infectionRenal failureSpinal cord compression Back
painParesthesiaElevated paraproteins-M peakLow
hemoglobinHypercalcemiaLow albuminHigh 2 microglobulinHigh serum
creatinineHigh c-reactive proteinLytic
lesionsOsteoporosisfracturesHigh in plasma cells
Treatment An Incurable hematological malignancyChemotherapy;
Dexamethasone, thalidomide and/or lemalidomiteRadiotherapy,
reducing bone painPlasmapheresis, reducing hyperviscosityBlood
transfusionIV fluids and diuretics, increasing urinary excretion of
calciumBisphophonates, preventing of bone loss and repairing of
bone lesions and control of hypercalcemia
Waldenstrm's MacroglobulinemiaWMInvolve small lymphocytes with
the exhibition of plasma cell differentiation; plasmacytoid
lymphocytesCells exhibit Pan-B lymphocyte surface antigens: CD19,
CD20, CD24, with light chain restriction mostly
IgM-secreting lymphoplasmacytoid cells express both cytoplasmic
and surface IgM Accumulation of monoclonal IgM paraproteins
(macroglobulin) in the bloodThe IgM acts like cryoglobulin with
anti-i specificity; cold autoimmune hemolytic anemia
Diseases associated with IgM monoclonal proteinsIgM monoclonal
gammapathy of undetermined significance (MGUS), the most common
Waldenstrm's macroglobulinemia, the next most commonmalignant
lymphoma IgM MMchronic lymphocytic leukemia (CLL), primary systemic
Amyloidosis, the least common
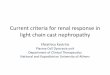
WM Bone Marrow Aspirate
http://imagebank.hematology.org/AssetDetail.aspx?AssetID=1178&AssetType=Asset
Differential Diagnosis WM vs IgM MMWMBone marrow infiltration by
small lymphocytesSurface Ig+, CD5-, CD10-, CD19+, CD20+, CD22+,
CD23- IgM MM Is extremely rare, account for













![Plasma cell neoplasmas [Read-Only]](https://img.pdfslide.net/doc/110x75/61c307aa2d33612dab6737b3/plasma-cell-neoplasmas-read-only.jpg)