Embed Size (px)
Citation preview

REGIONAL ANAESTHESIA IN
PAEDIATRICS
Dr. P. NARASIMHA REDDYDept. of ANAESTHESIOLOGY
NARAYANA MEDICAL COLLEGENELLORE
• HISTORY• INTRODUCTION• ADVANTAGES OF REGIONAL
ANAESTHESIA• RISK-BENEFIT RATIO• ESSENTIAL THINGS REQUIRED• HOW CHILDREN DIFFER FROM ADULT• REGIONAL ANAESTHESIA
PROCEDURES• SUMMARY

HISTORY

• First introduced at the end of last century at almost the same time as GA
• In 1898 BIER in his original paper on spinal anaesthesia on eleven year old boy described clinical effects
• JUNKIN, 1933 and ROBSON, 1936 described spinal anaesthesia for thoracic surgery
• Epidural anaesthesia in children was described by SIEVERS in 1936
• 1959 RUSTON introduced continuous epidural catheter technique.
• Local anaesthesia was invented by LADD by infiltration for abdominal procedures in neonates in 1930
• Sedation guidelines are released by ASA in 1996 and by AAP in 1992 and in 1997 by emergency physicians.
• In 1986 Dr. ANAND published his remarkable paper on pain in children and opened the eyes of many physicians’.
• RA in children is currently undergoing a renaissance in
anaesthesia practice.
• RA with GA fulfills the characters of an ideal anaesthetic.
• RA is also becoming the main stay of post operative pain relief in children.

INTRODUCTION
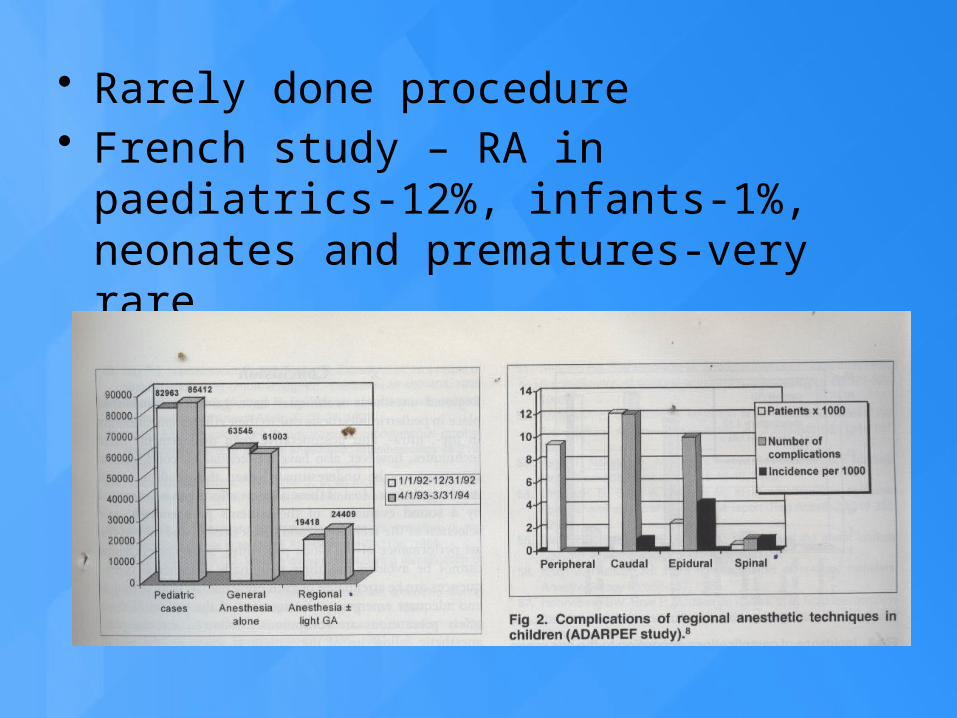
• Rarely done procedure• French study – RA in paediatrics-12%,
infants-1%, neonates and prematures-very rare

ADVANTAGES

• Modification of stress response and improved out come.
• IVRA in emergency department for surgeries on extremities with full stomach
• Epidural with catheter is very useful in ortho surgeries and post operative pain relief
• Caudal block as anaesthetic, analgesic for post operative and also after bone marrow harvesting.
• Effective for controlling pain in ICUs where Narcotics are dangerous or inadequate leading to undesirable effects.
• Decreases the GA drugs• Optimal post operative analgesia

RISK – BENEFIT RATIO

• Warning signals are missing such as pain in case of intra neural or CNS Symptoms in case of intra vascular injection.
• It is an accepted procedure provided the clinician performs the technique care fully and skillfully
• DALENS 1999 quoted that “It would be considered malpractice to perform RA in children who are not fully anaesthetized”.
• De Negri 2002 said “Any performance of a block in a agitated moving child is not only unethical but could be dangerous when needle approaches the delicate nerve structures”.
ESSENTIAL THINGS REQUIRED
• Skill in performing RA in adults for long time.
• Supportive surgical nursing facilities.• Assistance in OR • Proper equipment• PACU and DSU• Policies and procedures

HOW CHILDREN DIFFER FROM ADULT
• Psychological and parents psychology
• Physiological• Pharmacological• Anatomical

PSYCHOLOGICAL: • More apprehensive• Separation phobia• Universal needle phobia• Pain and disfigurement in older
children

• PSYCHOLOGICAL: Parents and grand parents:
• Loss of control over the situation• Dependency behavior• Financial constraints• Concern about the child’s
problem and outcome

PHYSIOLOGICAL• Post OP APNOEA is common in
premature infants.• Immature CNS • Immature BBB• Immature Sympathetic system• Nerve fibre are thin, less
myelinated, less nodes of Ranvier

PHARMACOLOGICAL:• Volume distribution is more• CSF volume high• Total body water high• Protein binding less
Metabolism of drugs-• Less than six months metabolism is
less• More than six months metabolism is
active.

Rate of absorption of local Anaesthetic• AIRWAY > INTERCOSTEL > CAUDAL >
EPIDURAL >BRACHIAL > DISTALPERIPHERAL> SUBCUTAENIOUS
• DOSAGE OF Drugs:• 0.25 % BUPIVICAINE 0.5 to 1ml per kg
caudal

• CSF Volume

• Duration of action of LA
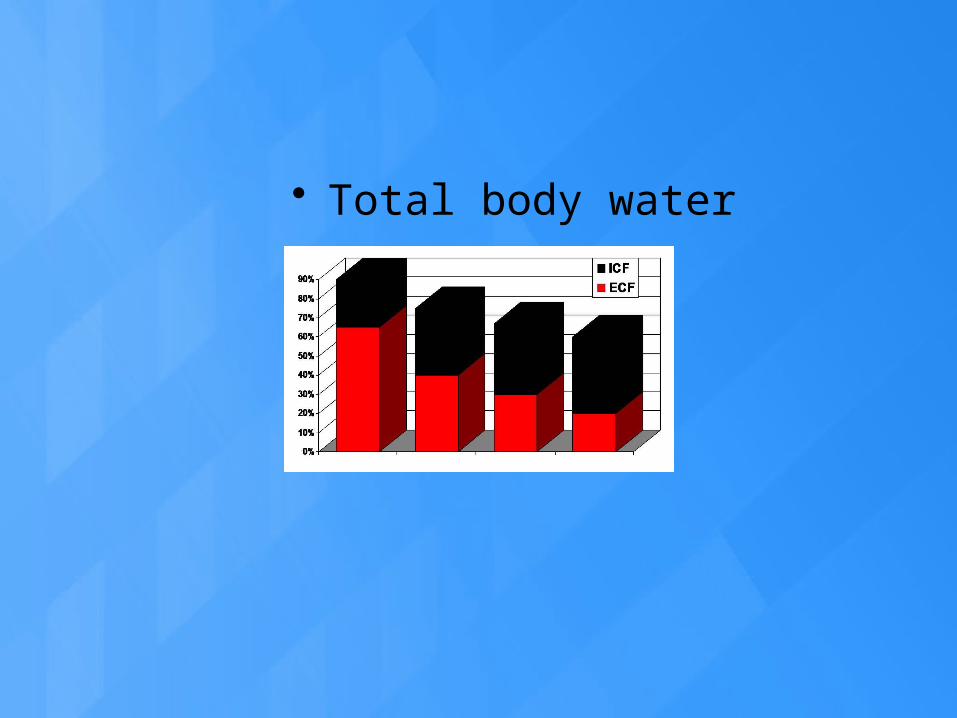
• Total body water

• Protein binding• It is low at birth• Albumin and alpha acid glycol protein less• Comes to adult level at one year
• Clearance –• Liver: phase 1 and phase 2 reactions
decreased • Kidney: GFR 30 % of adults• Adult level by 3-5 years of age.

• Morphine t 1/2 life is twice of adults • IV < 6/12 Apnoea, Cei < 12/12 no
fentanyl • Be careful with repeated dosing and
infusions • Neurological symptoms > cardiac symptoms
first symptom may be grand mal epilepsy

Anatomical:

• Anatomical:• Spinal cord is at lower level ( L3-L4)• Laminae are not well developed• CSF volume is high, turnover is high, shorter
duration of LAs action• No hypotension up to 6-8 yrs as
sympathetic system is not well developed• Epidural fat is like gel• Ligaments are not well developed

REGIONAL ANAESTHESIA PROCEDURES

• REGIONAL ONLY
• COMBINED REGIONAL AND GENERAL

• RA only : • Reduces the risk of post operative
apnoea in pre mature children. • Over night monitoring must be there• Caudal 0.25 % , 1 ml/ kg + clonidine
mcg/ kg• Spinal bupivicaine 0.5 % heavy
depending on the age of the patient ( 0.3 to 0.6 mg/kg)
• In older age group RA can not be done alone.
• COMBINED RA + GA :• Usually RA for anaesthesia and also for post
operative pain relief• Single caudal • Continuous epidural / caudal• Peripheral nerve blocks • Field blocks• Local infiltration.
• Indications: All blocks which are possible in adults can be done. PNS can be used; ultra sounding also can be done.
• MH• Avoiding need of OPIOIDS • Better analgesia • Epidural infusions
• Pulmonary diseases, fracture ribs• Bladder surgery• Abdominal and thoracic surgeries

• Contra-indications:• Parent refusal • Sensory nervous system diseases• Serious sepsis• Bleeding disorders• Vertebral malformations• Previous surgery on spines• Allergy
• Caudal anaesthesia and analgesia • Single Dose• Continuous Infusions• Adjuvants
• Spinal anesthesia
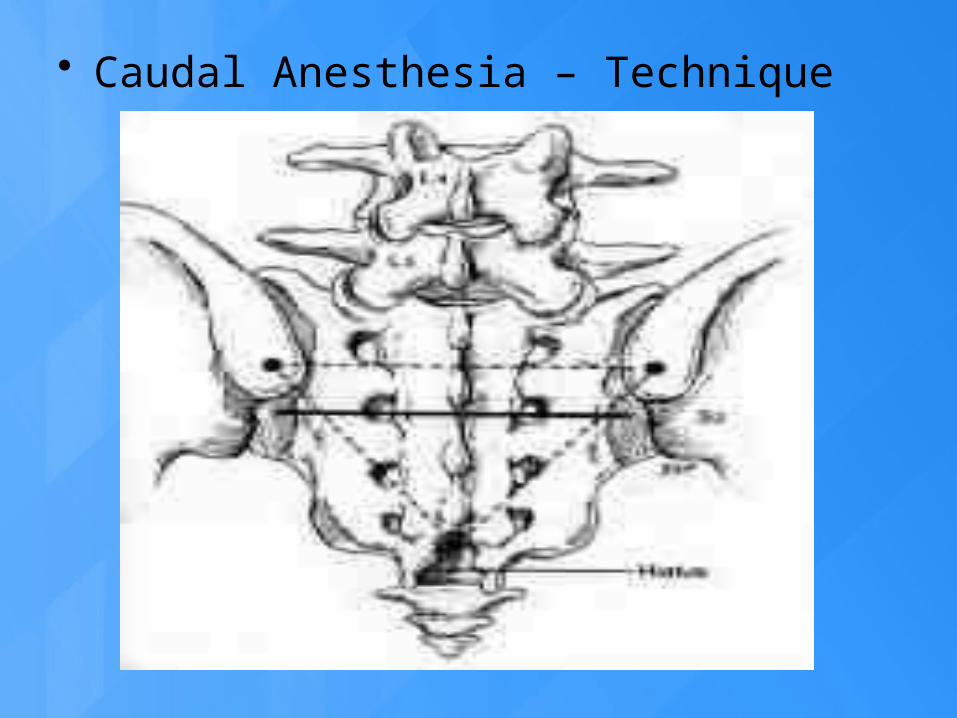
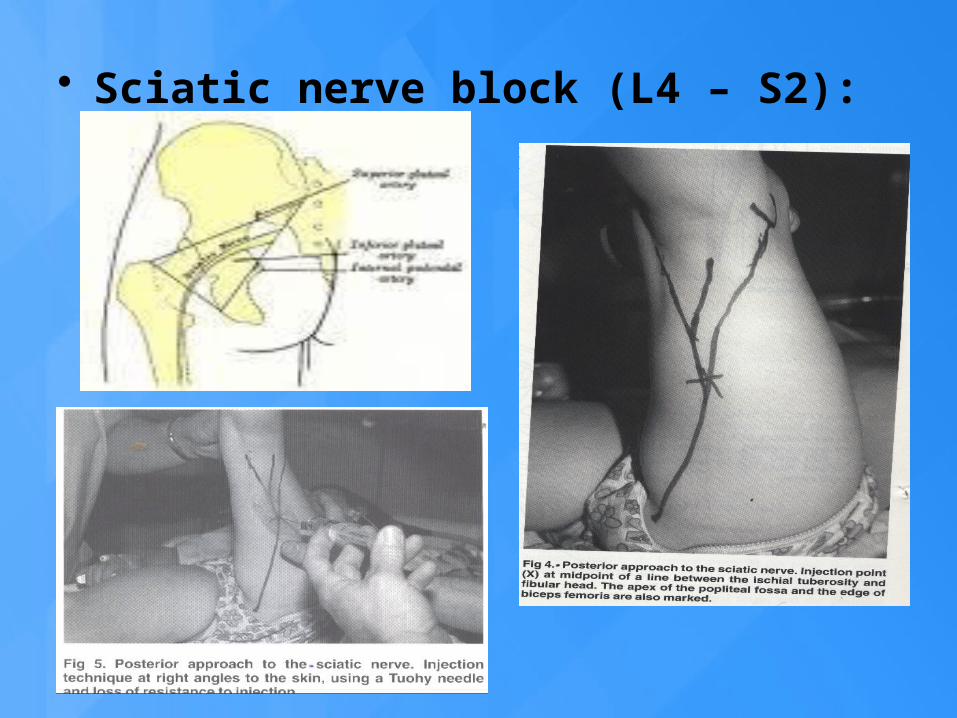
• Caudal Anesthesia – Technique

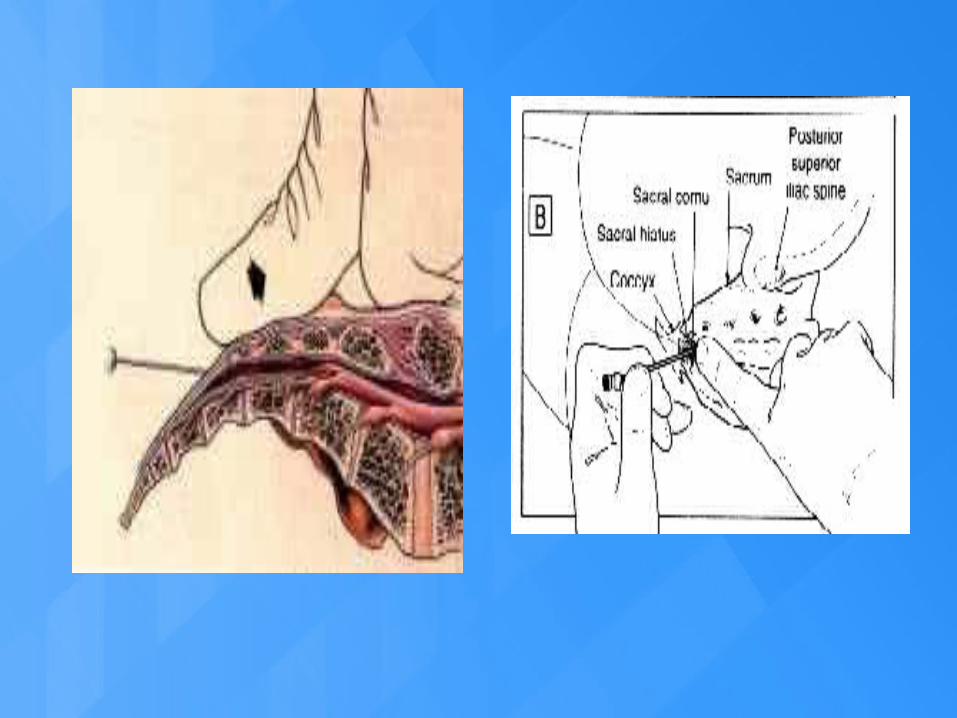


Where can a caudal go?Periosteum Sacral ligamentsDural sheathSacral marrowIntra vascular Sacral foraminae

• Commonly used drugs
DRUG BOLUS DOSE INFUSION
Bupivacaine 2.5 mg/kg 0.25 mg/kg/hr
Ropivacaine 3 – 4 mg/kg 0.4 mg/kg/hr
Levobupivacaine 2.5 mg/kg 0.25 mg/kg/hr
Lidocaine 7 mg/kg 2 mg/kg/hr

• LA volumes:• Traditional
• 0.05ml/seg/kg • 0.5 ml/kg upto T-10 segments 0.25%
Bupi• 1 ml/kg upto T-6 segments
• For longer duration• Lower concentrations with higher dosage
– 1.5ml/kg upto T-2 segments
• Concentration of local anaesthetics:• Balance analgesia with risk of motor block,
0.25% Bupivacaine, maximum dose of 1mg/kg gives excellent analgesia, less motor blockade and shorter duration of action.
• 0.175% Bupivacaine, 1.5mg/kg causes less motor blocked, good analgesia with higher level and longer duration of action (10ml = 7 ml of 0.25 + 3 ml of NS)
• Caudal morphine: • 30-40 mcg provides analgesia for 12 to 24 hours no
respiratory depression. • Nausea present • less labor intensive. • Does not require special pain clinics.
Side effects: • Nausea, itching • Clonidine:• Increases the effects of Bupi. Risk of sedation if given
more than 1 mcg/kg. •


• Continous infusions: • Caudal 16 G angio-cath with 19 G epidural
catheter can be threaded up to thoracic level and covered with sterile drape.Volume of drug:
• Less than 1 yr.: 0.1-0.2 ml/kg/hr• More than 1 yr. 0.1-0.4 ml/kg/hr + Fentanyl:
< 0.5 mcg/kg/hrConcentration of drug:
• Less than 1 yr.: 0.1% Bupivacaine• More than 1 yr.: 0.1% Bupivacaine + Fentanyl

Itching Diphenhydramine Naloxone - 0.5-2mcg/kg
Nausea Metoclopramide Naloxone
Urinary retention
Straight cath prn Naloxone
Sedation Turn down infusion
Respiratory depression
Naloxone -10mcg/kg

• Epidural anaesthesia: Technically similar to adults except for
• Depth of epidural space is less
• Ligaments are thinner and difficult to feel the resistance
• Midline approach is preferred as laminae are not well developed
• Epidural fat is like gel and catheters can be passed very easily


• Spinal anaesthesia: Technically similar to adults. Not very commonly done procedure, must have IV access, 1.5 inch 25 G beveled needle.
• Dose: 0.3-0.6 mg/kg of 0.5 % Bupivacaine heavy. Higher the age, lower the dose and vice versa
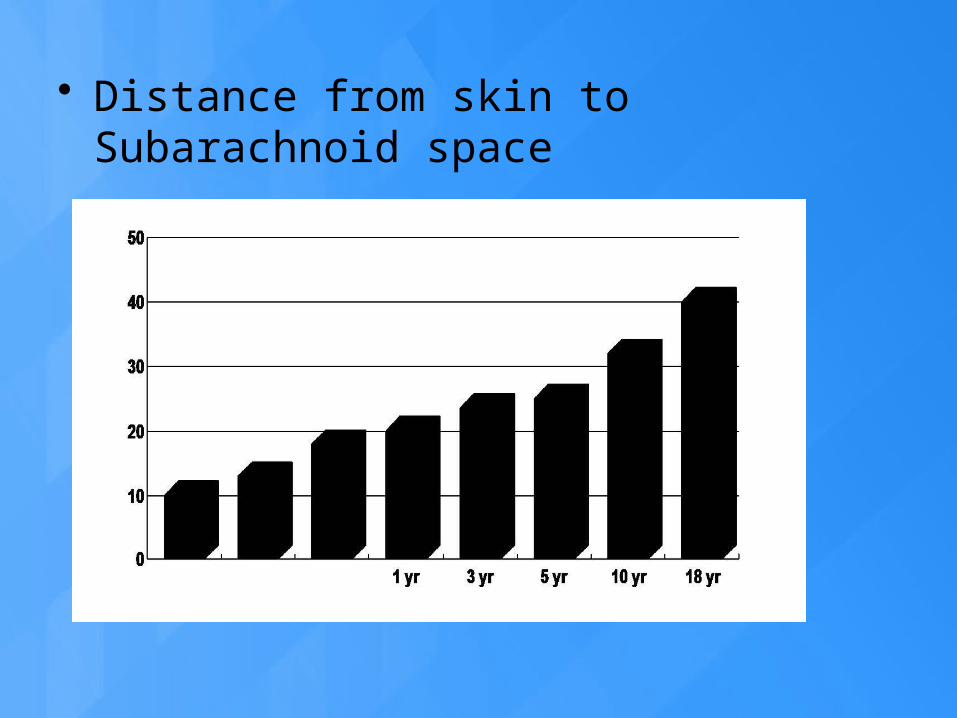
• Distance from skin to Subarachnoid space
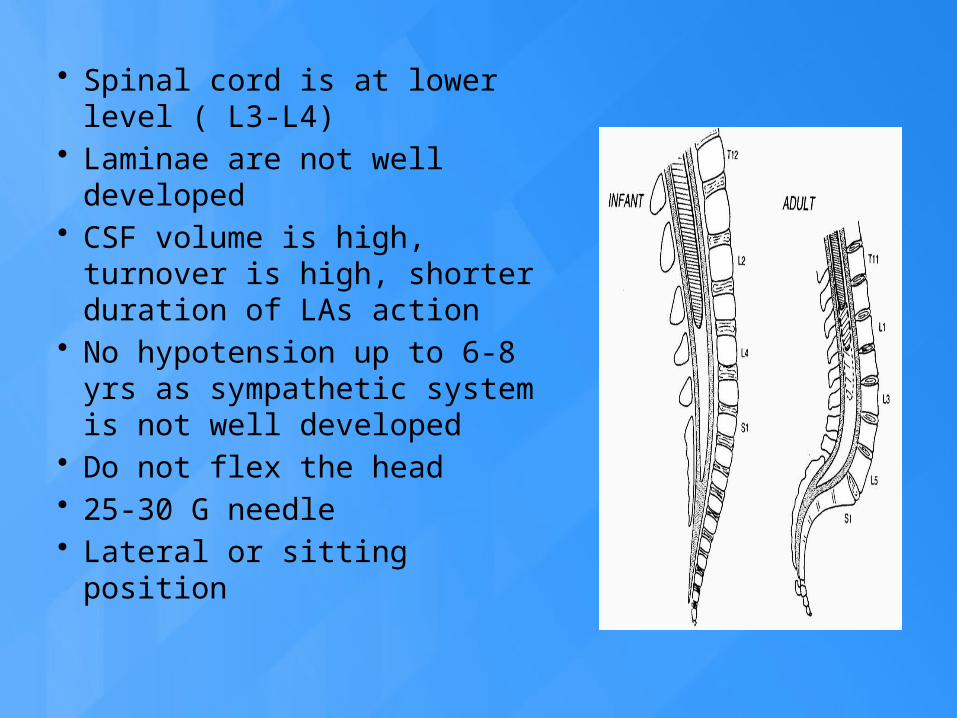
• Spinal cord is at lower level ( L3-L4)
• Laminae are not well developed
• CSF volume is high, turnover is high, shorter duration of LAs action
• No hypotension up to 6-8 yrs as sympathetic system is not well developed
• Do not flex the head• 25-30 G needle• Lateral or sitting position

• Combined spinal epidural (CSE):
• This overcomes shorter duration of action.
• Major procedures can done and
• post-operative analgesia well maintained.

PERIPHERAL BLOCKS
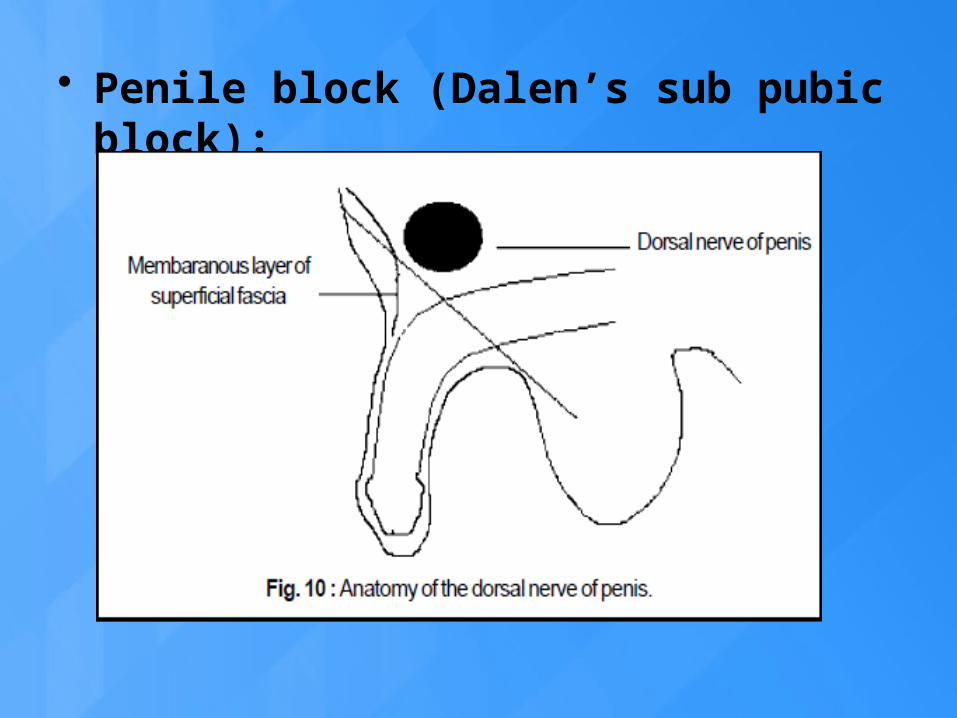
• Penile block (Dalen’s sub pubic block):

Simple subcutaneous ring block at the root of the penis is sufficient but duration is only for 2-4 hrs.
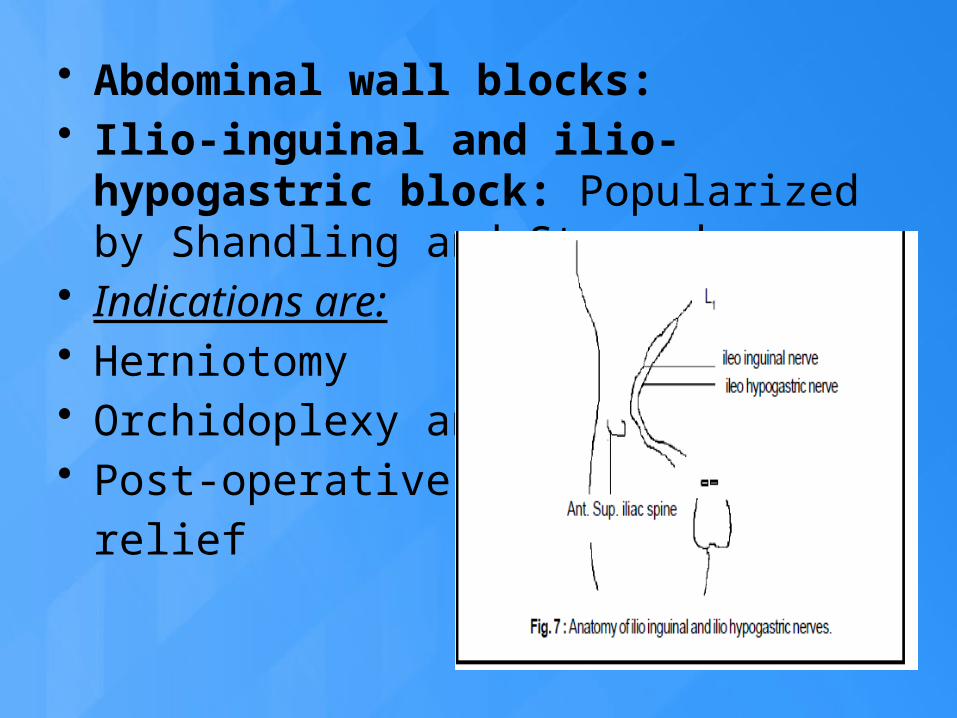
• Abdominal wall blocks: • Ilio-inguinal and ilio-hypogastric block:
Popularized by Shandling and Steward. • Indications are:• Herniotomy• Orchidoplexy and • Post-operative pain
relief


• Rectus sheath block• First described in 1899, better done with ultra sound
guidance• This block is used for umbilical hernia repair or
umbilical incision for lap procedures. • Blocking nerves in the posterior part of the sheath
deep to rectus muscle. • Anterior an posterior blocks are available.• A need is inserted lateral to umbilicus and advanced
through the fascia which can be detected by loss of resistance.
• LA is injected bilaterally, 0.2 to 0.3 ml/kg, 0.25 % Bupivacaine. At least 6 minutes needed to get anaesthesia.

• Transverse abdominal plane block (TAP)• Blind injection at the triangle of DE PETIT.
Now ultrasound guided injections are done between transverse and internal oblique muscles. This gives good post operative analgesia after appendectomy.


UPPER LIMB BLOCKS

• Brachial plexus block: • It can be sole anaesthetic or as an adjuvant to
GA or for post OP analgesia or for sympathetic blocks. It should not be used for trivial reasons. Age is not a contra-indication for this block. Must be associated with GA. PNS or USG can be used to locate the nerves.

• Inter scalene block:

• Supra clavicular block:

• Axillary block:

• Para Scalene approach (DALENES):• Patient supine with a role under the
shoulder, arm by the side and head turned to opposite side.
• The injection site is the junction of upper ⅔with lower of the line joining the mid ⅓point of the clavicle and transverse process of sixth vertebra.
• Less complication.

LOWER LIMB BLOCKS

• Femoral nerve block:

• LATERAL CUTANEOUS NERVE OF THIGH (LCNT) BLOCK:
COMPLICATIONS

• Complications due to the needle:• Wrong needle• Imprudently inserted• Symptoms can be delayed by
several hours• Spinal haematoma

• Complications related to technique:
• Location of nerve and space – electrical burns
• LOR syringe • Saline• Air
• Accidental PDPH
• Complications due to catheters:• Misplacement• Kinking• Knotting• Migration• Delayed lumbar stenosis• Shearing• Bacterial contamination

• Complications due to LA solutions:
• Local toxicity :• Injection of wrong solutions• Continuous infusions• Preservatives and additives• High concentrations
• Systemic toxicity• CNS toxicity• Cardiac• Methhaemoglobinemias
• Most LAs are anticonvulsants (1-5 mcg)• High concentartions convulsant and
respiratory arrest• Drug interactions – digoxin , bilirubin,
cimetidine and propronolol.
• Methaemoglobinemia :• Can occur after several hours• With prilocaine and benzocaine and
rarely lidocaine.• Predisposing factors
• G6p deficiency• Aniline dyes• Oxidants
• Treatement – inj methyline blue 1-5 mg/kg

• Complications due to adjuvants:• Preservatives like metabisulfate,
antioxidants can produce severe toxicity
• Narcotics can produce respiratory depression , pruritis , bladder distension.
• Complications resulting from inadequate management:
• Bacterial contamination• Unsafe technique of injection –
high pressure epidural injection• Injection in the wrong space
• Complications wrongly attributed to regional blocks:
• Hypotension , blood loss, position, surgical manipulation
• Sickle cell disease • Sudden infant death syndrome

CONCLUSIONS• All blocks can be given like adults• Differences from adult in various body systems
must be known• PNS or ultrasound guidance is advisable• Blocks are given under GA, be careful about
injuring the nerves and intravascular injections• Continuous catheters with infusion can be used• Correct dose and correct drug must be selected• Be careful with narcotics in pre-mature
children• Be careful with adjuvants

Conclusions……….• Emergency equitment for CPR, if required should
be available• Necessary monitoring systems should be present• IV access• Starvation guideline • Proper equipment and needles• Adequate exposure to regional anaesthesia in
adults• PACU and DSU facilities• Recovery room facilities • Discharge guidelines

THANK YOU