Embed Size (px)
Citation preview

Topic presentation- POAG
Dr.Lhacha WangdiR3, JDWNRH/KGUMSB
2016

Objectives Aqueous formation and drainage systemGlaucoma overviewPOAG: Pathophysiology of raised IOP Glaucomatous optic neuropathy Clinical manifestation Investigations and interpretation of the results Management principles

Aqueous humor
Formation: Aqueous is secreted by the bilayer ciliary epithelium
at the pars plicata of ciliary body

Aqueous productionThree Mechanism
1. Ultrafiltration ultrafiltration of plasma through the fenestrated capillaries into the ciliary stroma
2. Active transport (main mechanism)Number of solutes are actively transported from ultrafiltrated across the CE(PE+NPE) into the PC
3. Simple diffusionPassive transport of H2O to PC facilitated by the Osmotic gradient created by active transport

Active transport Three mechanism:
1. Loading of major ions/solutes occurs through the Basolateral membrane (BLM) of PE
Na-K-2cl and Na-HCO3 cotransporter / Na/H+ counter exchanger= uptake of of Na+, K+, CL- from stroma to PE coupled with anti-transport of H+ and HCO3- by Na/H+ and CL-/HCO3 antiports located in BLM of PE
2. Active transport of Na+ by Na+,K+ ATPase located at the BLM of NPE
3. Shifting of fluid and solutes from PE to PC is facilitated by the concentration gradient


Aqueous dynamics Secretion of aqueous balanced with drainage Secretion flow rate:2-3 uL/min. Aqueous volume(AC+PC)= (200ul+60ul)=260ul Maintains IOP of 11-21mmHg (average=16mmHg)
Diurnal variation – morning rise( 7.mmHg is considered normal upper limit)
Asymmetry of IOP >4mmHg is significant

Aqueous flow
1. Passes from PC to AC via pupil
2. About 90% of aqueuos flows through Trabecular meshwork which drain through Schlemm canal to episcleral vein
10% of aqueuos drain through Uveoscleral route across the face of ciliary body into the suprachoroidal spaces

Ctn..Angle structure
1. Schwalbe line (SL)2. Trabecular meshwork(TM)3. Schlemm’s canal(SC)4. Scleral spur(SS)5. Anterior border of the ciliary
body(CB)1. (where its longitudinal fibers insert
into the scleral spur)
6. Iris (I)

Trabecular meshwork (TM)
TM Circular spongework of connective tissue lined by
trabeculocytes Triangular in cross section. Apex at Schlemm’s canal Base formed by the scleral spur and the Ciliary body

Trabecular meshwork3 parts:
1. Uveal Contains large and circular cordlike trabeculae Diameter of pores-70pm in diameter
2. Corneoscleral Series of thin, flat, perforated connective tissue sheets arranged in
a laminar pattern Pores-35pm in diameter (moderate resistance
3. Juxtacanalicular Pericanalicular connective tissue-a multilayered collection of cells
forming a loose network- Pores -7pm in diameter (highest resistance to flow)

Glaucoma Definition:
Glaucoma is a group of acute and chronic, progressive, multifactorial optic neuropathies in which intraocular pressure (IOP) and other contributing factors are responsible for a characteristic, acquired loss of retinal ganglion cell axons leading to atrophy of the optic nerve with demonstrable visual field defects
The word glaucoma came from the ancient Greek word glaucosis, meaning clouded or blue-green hue, most likely describing a patient having corneal edema or rapid evolution of a cataract precipitated by chronic elevated pressure

Glaucoma
When to suspect?1. Glaumatous optic neuropathy2. Characteristic visual field loss3. Raised IOP
Other clinical signs will depend on the Type of glaucoma

Glaucoma
Classification
Congenital Acquired
Angle closure Open angle
Primary Secondary
Acute Chronic


Primary open angle glaucoma(POAG)
Definition: Multifactorial optic neuropathy that is chronic and
progressive with a characteristic acquired visual field loss in presence of open anterior chamber angle.
Commonly bilateral disease of adult onsetCharacteristics:
1. Primary glaucomatous optic neuropathy2. >IOP 21mmHG at some stage3. Characteristic visual field loss4. Absence of secondary cause of glaucoma
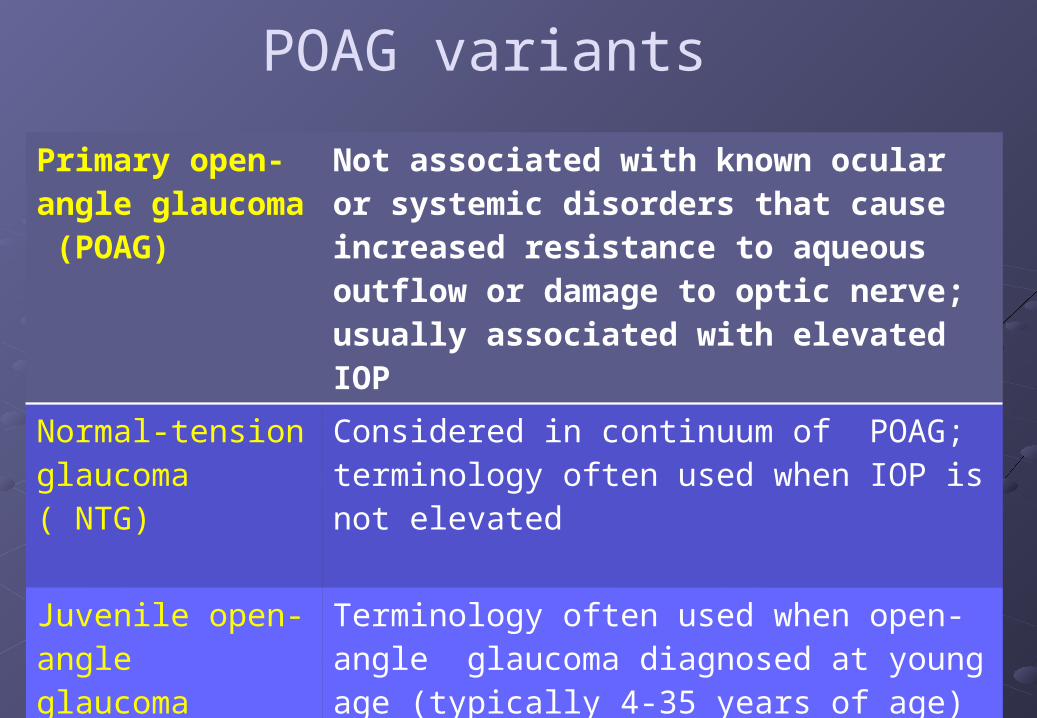
POAG variants
Primary open-angle glaucoma (POAG)
Not associated with known ocular or systemic disorders that cause increased resistance to aqueous outflow or damage to optic nerve;usually associated with elevated IOP
Normal-tensionglaucoma ( NTG)
Considered in continuum of POAG; terminology often used when IOP is not elevated
Juvenile open-angleglaucoma (JOAG)
Terminology often used when open-angle glaucoma diagnosed at young age (typically 4-35 years of age)
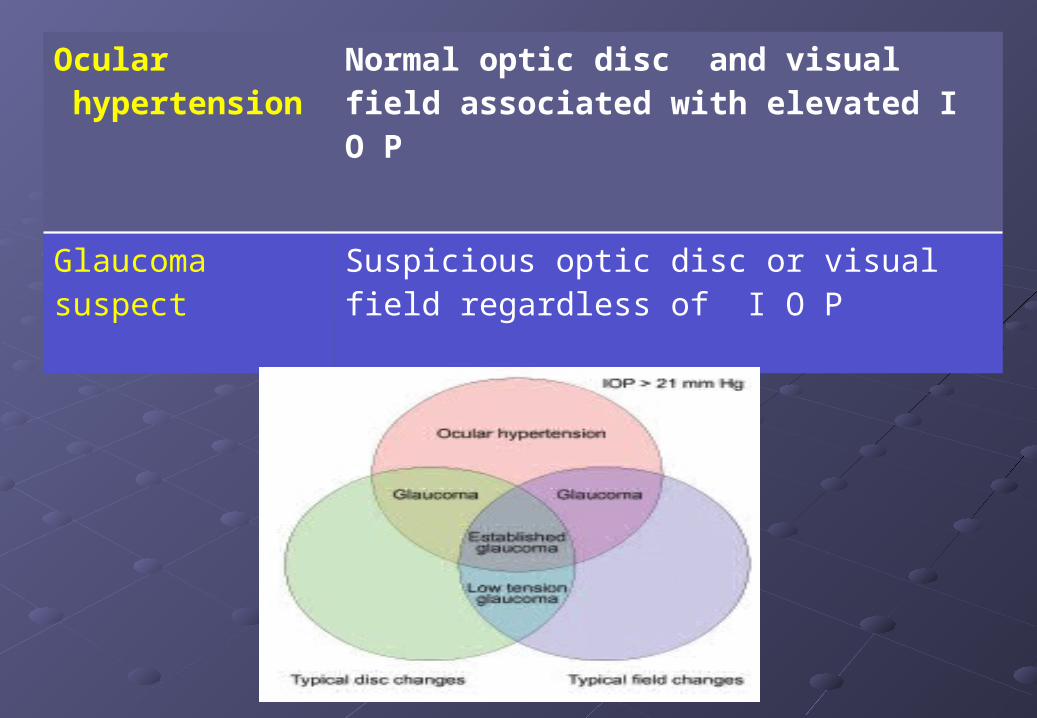
Ocular hypertension
Normal optic disc and visual field associated with elevated I O P
Glaucoma suspect
Suspicious optic disc or visual field regardless of I O P
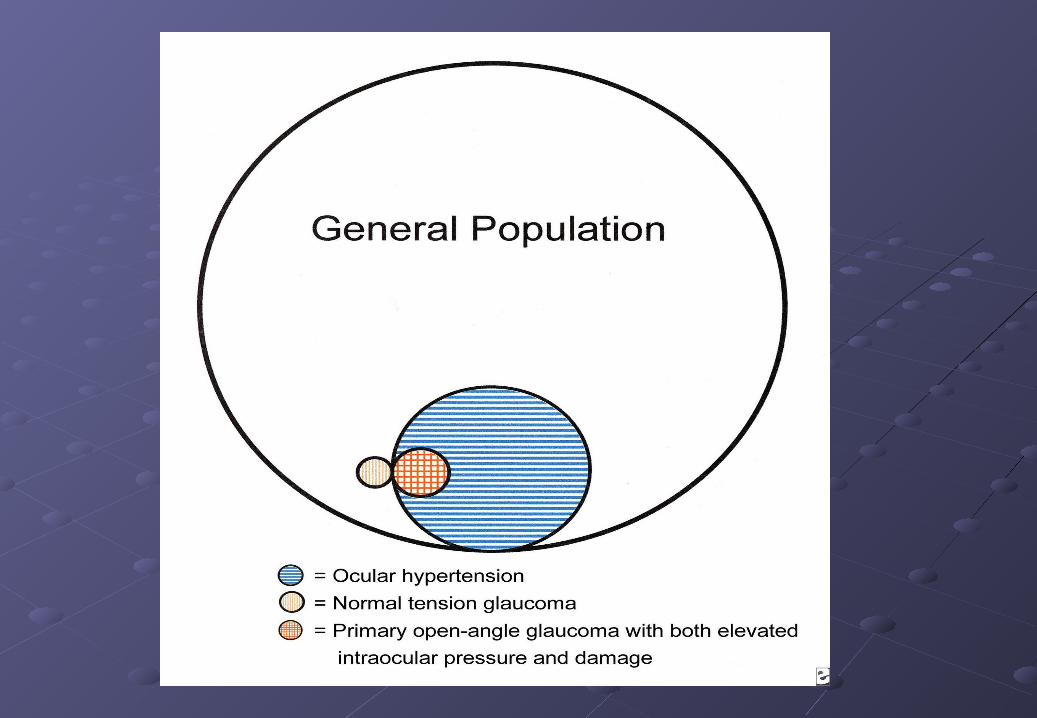
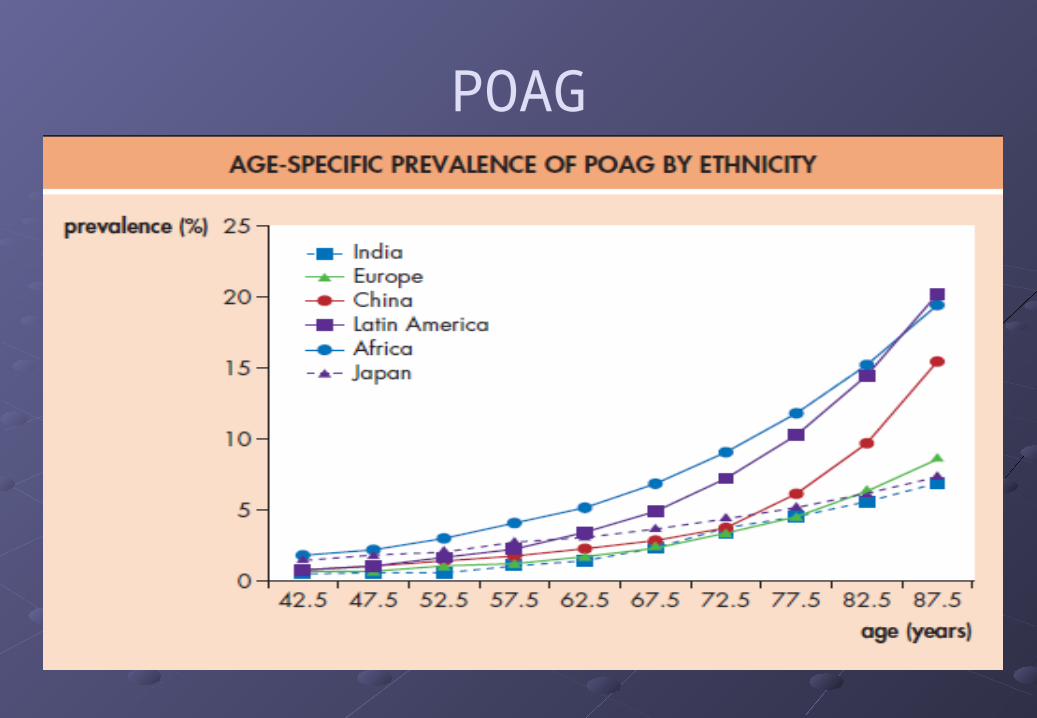
POAGEpidemiology: Prevalence of 6% in white populations, 16% in black
populations and around 3% in Asian populations. Most common type of glaucoma
Globally:Glaucoma affects more than 67 million persons worldwide10%, or 6.6 million, are estimated to be blind Glaucoma is responsible for 14% of all blindness
POAGRisk factors: The higher the IOP/Asymmetry of IOP of 4 mmHg or more Older age More common in black individuals than in whites Genetics Steroid usages Diabetes mellitus Myopia Contraceptive pill Vascular disease Translaminar pressure gradient. Large discs

Genetics of POAG Inheritance:
Most POAG pedigrees do not show a simple Mendelian pattern of inheritance- largely unknown
A minority of POAG pedigrees do demonstrate a Mendelian pattern of inheritance:
1. Autosomal recessive- commonest type2. Autosomal dominant pedigrees have also been described, with
a degree of penetrance varying from 60% to 100%3. Rare pedigrees showing possible sex linked inheritance have
been reported

Genetics of POAGMolecular genetic: Gene expression analysis has found out 26 genetic
loci in the region of the long arm of chromosome 1, 1q21-q31 associated with POAG
Out of these only three gene has been discovered till date:
1. Myocilin (MYOC)2. Optineurin3. WDR36


Ctn..MYOC(myocilin)-Most studied gene:
Also called TIGR(trabecular meshwork induced glucocorticoid response protein)Normally myocilin protein is secreted by TM cells into aqueous
Mutated myocilin protein is not secreted and retained within TM cells:
Interferes with TM function Causes TM cell death Obstruction of aqueous drainage- raised IOP

Ctn…
Optineurin &WDR36:
It is expressed in a variety of ocular tissues, including the ciliary body, TM, and retina.
Itsrole in glaucoma pathogenesis is still unclear

Pathogenesis of raised IOP in PAOG Mechanism:
ComplexMain mechanism:
Obstruction of aqueous through open angle Pathological changes in the angle structures
Cause of aqueous obstruction: Multifactorial: Genetic Aging Race Ocular risk systemic risk factors Drugs

Ctn…
Thickening and sclerosis of trabecular meshwork with faulty collagen tissue
Narrowing of intertrabecular spacesDeposition of amorphous material in the
juxtacanalicular space
Collapse of schlemm’s canal and absence of giant vacuoles in the cells lining it
Reduced aqueous outflow facility occurs due to failure of aqueous outflow pump mechanisms:

Pathogenesis of raised IOP in POAG
obstruction of aqueous outflow
High risk groups
Transforming growth factors (TGFs)• Inhibition of epithelial cell growth• excessive amounts of extracellular matrix
materials - GAGs
Alteration of TM:• increase in extracellular matrix and
an accumulation of “plaque material.”
• Thickening of basement membrane
• disrupt TM cell actin microfilaments
Thickening of juxtacanalicular connective tissue
Decreased in Pores and giant vacuoles in the inner wall endothelium of the Schlemm canal Collapse of the Schlemm Canal
Alterations of the Intrascleral Channels• due to a swelling of
glycosaminoglycans in the adjacent sclera

Steroid responsiveness
“Steroid Responder” Around one in three individuals develop some
degree of elevation of IOP in response to a course of potent topical steroid
“Non-responders” IOP is not affected by steroid

Steroid responderMechanisms:
1. Glycosaminoglycans Theory:Cortico — steroids stabilize the lysosome membrane of TM cells► reduced catabolic enzyme►reduces GAGs catabolism► increased polymerised form of GAGs► increases resistance to aqueous outflow.
2. Phagocytosis Theory:Suppress the phagocytic activity of endothelial cells lining the trabecular►buildup of material that could account for the amorphous layer in the juxtacanalicular connective tissue meshwork
3. Cyclic-Adenosine Monophosphate Theory:Altering cyclic-adenosine monophosphate- mechanism poorly defined

Glaucomatous optic neuropathyPathogenesis:
1. Direct mechanical damage to retinal nerve fibres
2. Ischaemic damage3. Common pathways of
damage
1 2
3

MECHANICAL
mechanical pressure on the lamina cribrosa
mechanical pressure on the lamina cribrosa
altering capillary blood flow backward displacement and
compaction of the laminar plates narrows the openings through which
the axons pass
GANGLION CELL DEATH

VASCULAR
rise in intraocular pressure
mechanical pressure on the lamina cribrosa
decrease the capillary blood flow
mechanical compression of vessels at the lamina
cribrosa
GANGLION CELL DEATH

POAG- clinical menefestation
The Silent thief of sight

Clinical features Symptoms:
Insidious and asymptomatic disease Gradual painless loss of vision Mild headache, eye ache Visual field defect(SCOTOMA) Frequent change in presbyopic glasses Delayed dark adaptation Significant loss of vision and blindness

Ctn…Specific enquiry:
Refractive status(e.g myopia)Causes of secondary glaucoma (trauma/surgery/inflammation/tumour)Family history- glaucomaPast medical history-Asthma, heart failure/migraine and Raynaud phenomenon, DM/HTN.Drugs -Steroids/OCP/beta blockersSocial history- smoking/alcohol/nutrition-dietAllergies

Examination Work up:
1. Visual acuity2. Pupils-regularity/reaction/asymetry/RAPD/
APD3. Color vision assessment4. Visual field- confrontation test5. Slit lamp examination- detail examination of
anterior segment/fundus

Visual field examination
Screening tests …Confrontational visual field testing Amsler grid (assesses the central 10° the visual field ) .
Quantitative measurements using manual or automated perimetry

Cnt..
Anterior segment:
Corneal haze AC depth and any reaction Pupil- syniechae Evidences of secondary
cause


Ctt..The van Herick method: gross estimation
Uses the slit lamp alone to estimate the AC angle width:

Funduscopy
• Fundus :1. Optic disc
assessment2. Parapapillary
changes3. Vessels 4. Nerve fiber

Optic disc- surface anatomy
Around the optic cup is neuroretinal rim (NRR):• Pink and sharp peripheral margin• Contain nerve axon• Broad inferior rim followed by superior> nasal>temporal ( ISNT
rule)
Disc: Vertically oval Vertical diameter-1.8mm
Horizontal diameter- 1.5 mm Pale center area-physiological cup Horizontally oval Free of nerve axon(cup)-0.3mm Normal CDR= 0.4
Inferior
superior
Nasal temporal

Glaucomatous Optic neuropathy
Glaucomatous damages in three regions:(a) the optic nerve head(b) the peripapillary area and (c) the retinal nerve fibre layer.
There are specific sings and non specific signs

Ctn…
Optic nerve:
Specific signs: Focal ischaemic discs Myopic disc with glaucoma Sclerotic discs Concentrically enlarging discs

Focal ischaemic – inferior notch and disc haemorrhage
myopic;scleroticconcentrically enlarging

Glaucomatous ON
Nonspecific signs glaucomatous damages: Disc haemorrhages Baring of circumlinear blood vessels Bayoneting Collaterals Loss of nasal NRR The laminar dot sign ‘Sharpened edge’ or ‘sharpened rim’

baring of inferior circumlinearblood vessel
bayoneting of blood vesselscollateral vessels
loss of nasal neuroretinal rim and laminar dot sign

Ctn…Peripapillary changes
1. Alpha (outer) zone is characterized by superficial retinal pigment epithelial changes
2. Beta (inner) zone is characterized by chorioretinal atrophy

Ctn..
Retinal nerve fibre layer1. Localized wedge-shaped defects and
2. Diffuse defects that are larger and have indistinct borders

INVESTIGATIONS1. Tonometry2. Central corneal thickness(CCT)3. Diurnal variation test4. Gonioscopy5. Perimetry to detect the visual field defects6. Nerve fibre layer analyzer (NFLA)7. Provocative tests
Water drinking test

TONOMETRYThe intraocular pressure (IOP) is measured with the help of an instrument called tonometer
Indentation tonometerySchiotz tonometer
Applanation tonometryGoldmann tonometerPerkin’s applanation tonometerPneumatic tonometerPulse air tonometerTono-Pen
Rebound tonometry - icare Schiotz tonometer

Technique of Schiotz tonometry
Technique of applanation tonometry
End point of applanation tonometry. (A) too small; (B) too large; (C) end point.

Gonioscopy
The technique of biomicroscopic examination of the angle of the anterior chamber using a goniolens.
The angle structures seen from behind forward are:1. Root of the iris2. Ciliary body band3. Scleral spur4. Trabecular meshwork5. Schwalbe’s line

Schaffer’s grading
Grade 0
Grade 1Grade 2
Grade 3
Grade 4
Grade 4 (35–45°) is the widest angle, the ciliary body can be visualized. Grade 3 (25–35°) is an open angle, scleral spur is visible. Grade 2 (20°) is an angle in which the trabeculum but not the scleral spur can be seen. Grade 1 (10°) is a very narrow angle in which only the Schwalbe line and perhaps the top of the trabeculum can be identified. Slit angle is one in which there is no obvious iridocorneal contact but no angle structures can be identified. Grade 0 (0°) is closed due to iridocorneal contact.

Visual field defects
Relative paracentral scotoma
Roenne’s nasal step
Seidel scotoma
Arcuate scotoma
Double arcuate / ring scotoma
End stage / near total field defect

A paracentral scotoma- loss of nerve fibers ininferotemporal retina
The arcuate scotoma-10-20° from fixation-Bjerrum scotoma
Nasal stepAltitudinal defectAdvanced glaucomatous V. Field loss

SEIDEL SCOTOMAstarts at the poles of the blind spot , arches over the macular area without reaching the horizontal meridian nasally
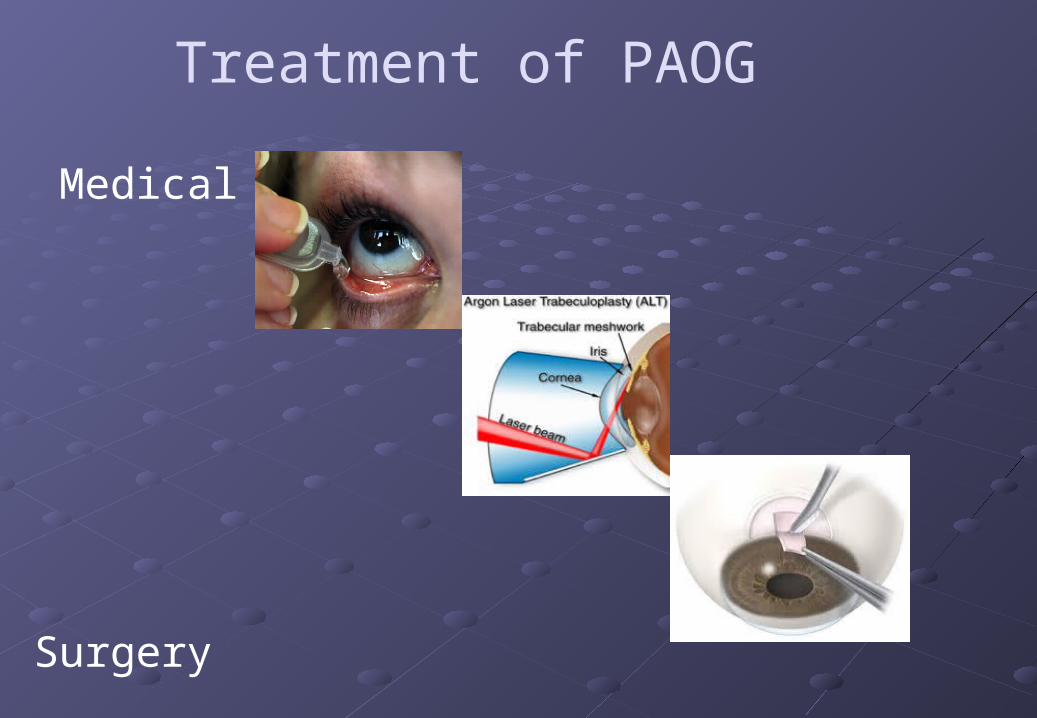
Treatment of PAOG
Medical
LASER
Surgery

ManagementPrinciple:
Determine TARGET PRESSURE – Reduction of IOP by at least 30% appears to have the best chance of preventing optic nerve damage
Starting drugs-Monocular Therapeutic Trial (MTT) Reexamination in 3 to 6 weeks to check for
effectiveness. Exception to MMT:
IOP > 40 mm Hg impending loss of central fixation),

MEDICAL
MECHANISM
Decreased aqueous production
Increased facility of outflow (trabecular / uveoscleral)
Intraocular osmotic fluid reduction

Anti-glaucoma drugs# Agents Mechanism of action Drugs
1 Prostaglandins enhancementof uveoscleral aqueous outflow
Latanoprost(0.005%) - ODTravoprost(0.04%) -ODBimatoprost(0.03%) -ODTafluprost(0.04%) -OD
2 Beta-blockers
block β receptors in ciliary processes aqueous production
Timolol (0.25%/0.5%)-BDBetaxolol(0.25%,0.5%) -BDLevobunolol(0.5%)-BD Carteolol(1%, 2%) -BDMetipranolol(0.1%, 0.3%, 0.6%)-BD
3 carbonic anhydrase inhibitors
Inhibition of carbonic anhydrase- reduce aqueous production
Dorzolamide(2%) –BD-TDSBrinzolamide (1%)-BD-TDST-Acetazolamide (250mg),BD-QIDT-Dichlorphenamide(50mg) BD-TDST-Methazolamide(50 mg) BD-TDs

# Agents Mechanism of action Drugs 4 Alpha-2
agonistsOcular alpha-2 receptor stimulation decreases aqueous synthesisvia an effect on the ciliary epithelium, and increases uveoscleral outflow.
Brimonidine(0.2%)BD-TDS dosageApraclonidine (0.5%,1%)BD-TDSClonidine (0.125%,0.25%) BD
5 Miotics cholinergic agonists-reduce IOP by contraction of the ciliary muscle, also opens angle by miosis
Pilocarpine 0.5%, 1%, 2%, or 4% solution as four timesCarbachol(0.75%,1.5%,3%)BD-TDS dosage
6 Osmotic agents
lower IOP by creating an osmotic gradient so thatwater is ‘drawn out’ from the vitreous into the blood
Mannitol IV(20% solution1-2g/kg over 20-30 minutes,Glycerol is an oral agent (1 g/kg body weight or 2 ml/kgbody weight of a 50% solution)Isosorbide is a metabolically inert oral agent

Prostaglandin Side affects
Systemic :1. Upper respiratory tract symptoms (flu like )2. Headache and precipitation of migraine in
susceptible individuals3. Muscle and joint pains4. Skin rash

Prostaglandin side affects Ocular Side Effects
1. Conjunctival hyperaemia and foreign body sensation2. Eyelash lengthening, thickening, hyperpigmentation, increase
in number3. Iris hyperpigmentation4. Increase in severity and recurrence of herpetic keratitis5. Anterior uveitis6. Cystoid macular edema

Beta- blocker side effects Systemic
1. Cardiovascular effects – bradycardia, arrhythmia, heart failure, syncope
2. Respiratory reactions – bronchospasm and airway obstruction, especially in asthmatics
3. CNS effects – depression, anxiety, confusion, drowsiness, disorientation
4. Others – nausea, diarrhoea, decreased libido, skin rashes, alopecia
Beta-bockers Ocular side affects:
Conjuctival hyperaemia Superficial punctate keratopathy Corneal anaesthesia
1. Contraindications: Bronchial asthma Chronic obstructive pulmonary disease Heart blocks Congestive heart failure Cardiomyopathy

Carbonic anhydrase inhibiters Systemic side affects:
1. Paraesthesias, numbmness, lethargy, depression, malaise2. Metabolic acidosis, hypokalemia, increased serum urate
level3. Urinary frequency4. Anorexia, cramps, flatulence, weight loss, diarrhoea5. Sulfonamide related – blood dyscrasias, renal calculi,
steven-Johnson syndrome
Topical agents are less likely to induce systemic side effects
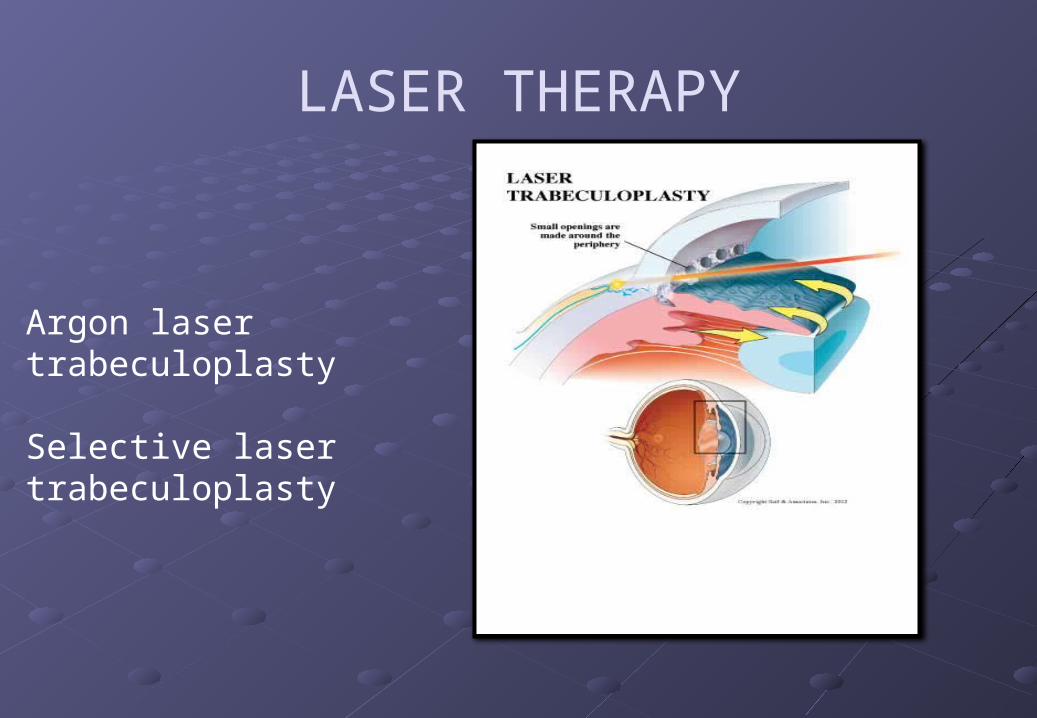
LASER THERAPY
Argon laser trabeculoplasty
Selective laser trabeculoplasty

Surgical
TRABECULECTOMY:
Involves creation of fistula between angle of anterior chamber and sub Tenon’s space

Trabeculectomy
Indications:Failure of conservative therapy to achieve adequate IOP control.Avoidance of excessive polypharmacyProgressive deterioration despite seemingly adequate IOP control (including poor compliance with medical treatment).Patient preference

DRAINAGE SHUNTSShunts using episcleral explantsGlaucoma Drainage Devices(GDD)= creates communication between AC and sub tenon space

THANK YOU












![[ON-SCREEN OVERLAY COPY] This Continuing Medical …...NO and the Pathophysiology of POAG [ON SCREEN: DR. TSAI] The pathophysiology of POAG is not yet fully elucidated, but it has](https://img.pdfslide.net/doc/110x75/5e83541ed5d6137cea698220/on-screen-overlay-copy-this-continuing-medical-no-and-the-pathophysiology.jpg)














