Embed Size (px)
Citation preview


Definition
“Pain is whatever the experiencing person says it is, existing where
he/she says it does”
McCaffery (1980)

Physiology of pain
In its simplest form, the pain circuit in the body can be described as follows• pain stimulates pain receptors, and this
stimulus is transferred via specialised nerves to the spinal cord and from there to the brain.
• The pain stimulus is processed in the brain, which then sends an impulse down the spinal cord and via appropriate nerves which command the body to react, for instance by withdrawing the hand from a very hot object.

Pain Receptors
• Pain receptors are present everywhere in the body;
• Pain receptors are free nerve endings. • There are three types of pain receptor
stimuli: mechanical, thermal and chemical. • A mechanical stimulus e.g. high pressure
or stretching; thermal pain stimulus would be extreme heat or cold.
• Chemical pain receptors can be stimulated by chemicals from within and outside the body.

Pain nerve fibres
• Pain stimulus is transmitted from the receptors through peripheral nerves to the spinal cord and from there to the brain.
• This happens via two different types of nerve fibre: “fast pain” and “slow pain” fibres
• Fast pain is well localised, sharp and “cutting” and do not radiate.

Fast Pain Nerve Fibres
• They are thick nerve fibres called A-delta fibres. Because of their relative thickness.
• Pain stimulus are transferred very fast at a speed of 2-5s/m
• This allows the body to withdraw immediately from the painful and harmful stimulus in order to avoid further damage

Slow Pain Nerve Fibre
• They are thin nerve fibres called c nerve fibres.
• Pain impulse are transmitted slowly to the brain, at a speed of less than 2 m/s.
• The body responds by holding the affected part immobile (guarding, spasm or rigidity), so that healing can take place.

Pain transmission in the spinal cord and the brain
• The peripheral nerves carry the pain impulse to the spinal cord.
• In the spinal cord, fast pain and slow pain are carried up to the brain via different pathways
• The impulse of the fast pain goes to the cortex, allowing for the relatively precise localisation of the pain stimulus.
• The impulse from slow pain is distributed diffusely in the brain, with each area eliciting a different response

Characteristics of fast pain and slow pain
Slow Pain• Transmitted by very thin
nerve fibres• Poorly localised• All internal organs (except
the brain)• Body wants to be immobile
to allow healing (guarding, spasm, rigidity)
• Pain often radiates, or is referred
Fast Pain• Transmitted by relatively
thicker (and therefore faster conducting) nerve fibres
• Well localised• Mainly skin, mouth, anus• Immediate withdrawal of
stimulation to avoid further damage
• Pain does not radiate• Little relief from opioids
11/04/2023
Reviewed by Prof CL Odendal, senior specialist at the
department of anaesthesiology at the University of the Free State, April 2010.

Pain in the Elderly
• Effects of aging on pain sensation, perception, and behaviour are not well established
• Compared with younger adults, elderly persons rely more on slow/second pain (C fibre) than on fast/ first pain (A fibre).
• Another well-documented finding in the elderly is a slower response time to pain
• No evidence exists that pain intensity lessens with age

• Altered reactions to painful events may be due to loss of communications skills, cognitive abilities, or the failure of basic reflexes due to aging
• Additionally, pain in the elderly may be manifested as something other than pain, such as delirium

Pain in Children
• Children and young people have a right to appropriate prevention, assessment and control of their pain
• Historically, pain has been underestimated and under treated in children and particularly babies.
• Evidence shows that pain is inadequately dealt with for children, requiring better prevention, assessment and treatment.
• In order to treat children's pain effectively, a thorough pain assessment is necessary; a number of guides are available to do this

• British association for Emergency MedicineClinical Effectiveness committee: Guideline for the management of pain in children

How do we assess pain?
• Self report• Use pain rating tools• Non-verbal signs• Assess on movement• Document

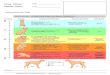
Pain Assessment
No Pain (0)‘Happy because I
don’t hurt at all’
Mild Pain (1)
‘Hurts just a little bit’
Moderate Pain (2)
‘Hurts more’
Severe Pain (3)‘Hurts as much
as I can imagine
“Pain is whatever the patient says it is”
Always assess on movement

Other Pain tools
• Intensity scores - VAS, Categorical• Pain relief scales• Cognitively impaired• Paediatric• Critical care• Chronic Pain
– McGill Questionnaire– Quality of Life Questionnaire– Brief Pain Inventory– Pain Self Efficacy Questionnaire

What do we assess?
• Location • Duration• Type• Intensity

What needs to be considered when assessing pain?
• Subjective• Age• Communication• Psychiatric factors• Cognitively
impaired• Culture• Knowledge of pain
treatments
• Expectations of pain treatments
• Language barriers

Barriers to pain assessment in the older person
• Failure to recognise• Failure to assess• Assume stoicism• Patients & carers expectations of
pain in ageing• May use different words e.g.
discomfort, ache, soreness • Time consuming

Inadequate pain management can cause:• physiological effects (increased HR, BP,
delayed gastric emptying, increased adrenaline production)
• post-operative complications (respiratory infection, VTE, PE)
• delayed discharge • mobilisation difficulties• restlessness, irritability, aggression• raised levels of anxiety• sleep disturbances• distress and suffering
(Sjostrom et al 2000, Macintyre & Ready 2002, Carr et al 2005)

Pain Management and the role of
Psychology

Acute Vs Chronic Pain
Acute Pain– Short Term– Less than 3
months– Natural Healing
Occurs
Chronic Pain– Long Lasting– Longer than 3
months– Natural Healing
occurs– but huge IMPACT– Pain as a result
of Central NS changes- local, spinal cord, brain

Why do people react so differently to Pain?
Leventhal’s Common Sense Model
PainAction Taken /
CopingBeliefs About
Pain

Chronic Pain and Psychological Distress
Chronic PainAnxiety &
Depression
How does psychological distress affect pain experience and management?
?

The BioPsychoSocial Model

Psychological Interventions
Cognitive Behavioural Therapy shown to be effective – Has impact on biopsychosocial variables
However, psychological interventions for chronic pain most effective when incorporate other treatment components– e.g. physiotherapy, education– Pain Management Programmes

Impact of Chronic Pain
Pain
Reduction in activity
Failed Treatmentseg physio, med
Loss of Job, Financial Stress
Relationships
Being Blamed/Faking it
PhysicalDeconditioning
DepressionHopelessness, Helplessness
AnxietyFear re Future
FrustrationAnger
Loss of Independence
Boom and Bust
ExcessSuffering

Pain Management Aims
NOT cure or pain reduction
Change the person’s relationship with pain– Reduce disability and distress – Manage increases in pain (flare-ups)– Develop confidence in ability to carry out
activities despite pain– Reduce unhelpful encounters with public and
private health systems– Self-Management

Aims of Pain Management
Pain
• Education re Pain Model
• Pacing
• Communication
•Identifying unhelpful thoughts
Improve Fitness
Improve daily functioning
Reduce anxiety/depression
Increase confidence
Reduce dependence
Reduce incidence of Flare-Ups
ReduceDistress
• Goal Setting &Practice
• Flare-up Planning
• Exercising
• Relaxation

MDT Consultants, physios, psychologists,
nurses Pain Management Programmes
– Good evidence base, improve functioning NICE guidance 88, May 2009
– Outpatient Programmes PMP @ Whittington, COPE @ UCH
– Inpatient Programmes INPUT Pain Management Unit @ St Thomas’ Bath Pain Management Unit

References Sharp & Keefe (2006). Psychiatry in Chronic Pain: A review and
Update. Focus, American Psychiatric Association.
Turk & Okifuji (2002). Psychological factors in chronic pain: Evolution and revolution. Journal of Consulting and Clinical Psychology.
Vlaeyen & Linton, (2006). Are we ‘fear avoidant’. Pain.
Vlaeyen & Morley (2005). Cognitive-Behavioural Treatments for Chronic Pain: What works for whom? Clinical Journal of Pain.
Morley, Eccleston & Williams (1999). Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain.
Nicholas M, Molloy A, Tonkin I and Beeston L (2000) Manage your Pain ABC Books, Sydney
Nice, Nice Guideline 88 (2009) – Early management of persistent non-specific low back pain, http://www.nice.org.uk/CG88