Embed Size (px)
Citation preview

Accelerating Drug
Development using
Biomarkers
Presented by Nabiilah, Naailah & Svenia
Date: 27th Jan 2015
• Introduction on:
– Biomarkers
– Diabetes Type 2
• Application of Biomarkers in drug development
– Sitagliptin
• Preclinical trials
• Clinical trials
• Conclusion
• References
BIOMARKERS
What is a biomarker? A biomarker is a substance in the body that can be measured and used
to tell doctors and scientists something about the state or health of a
person.
Imagine two individuals; each will have a slightly different
composition of substances in their blood; these substances include
protein or small molecules that circulate around the body.
The aim is to measure the substances and build up a fingerprint of the
composition of someone’s blood.
These biomarkers fingerprints are then investigated for specific
substances that may show clear differences between two people or
which mark a difference between groups of people; if one of these
people is a healthy volunteer and the other with a chronic disease
such as diabetes, then we will have to see whether a specific
substance is higher or lower in people with the disease.
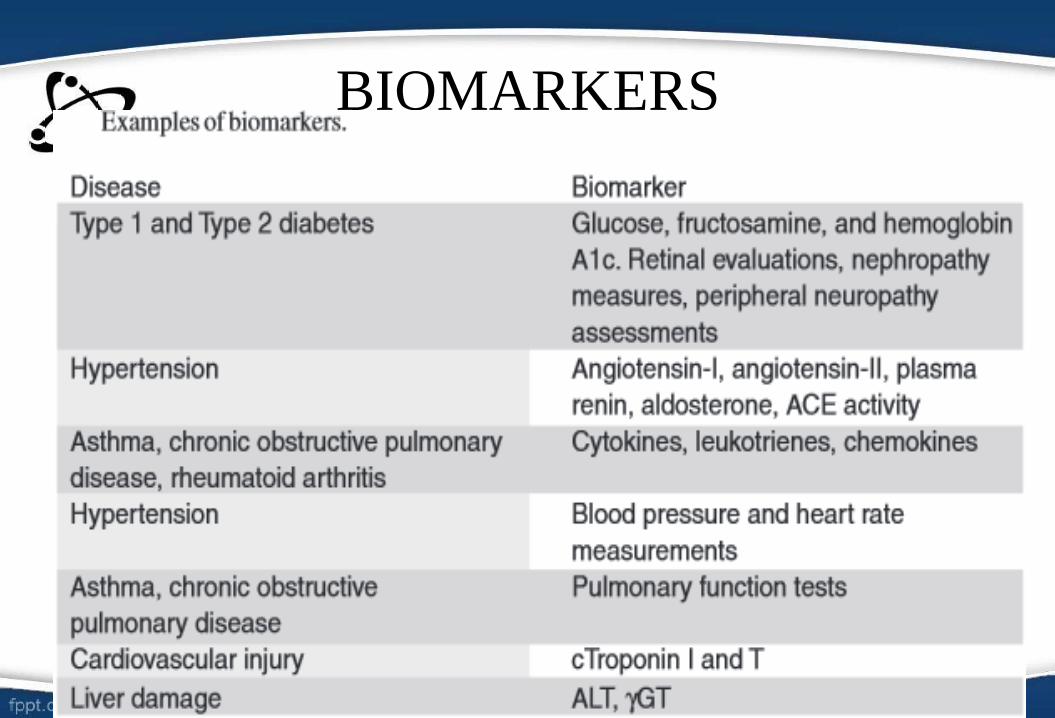
BIOMARKERS
If this is the case, this substance can be used as a biomarker
to help doctor with diagnosis and predicting disease stage
or severity or whether it will respond to treatment.
Furthermore, we can look to see whether by bringing the
level of this substance back to the healthy patient’s level,
we can help treat their disease.
If this proves successful, we can use this substance as a
basis for new medicines.
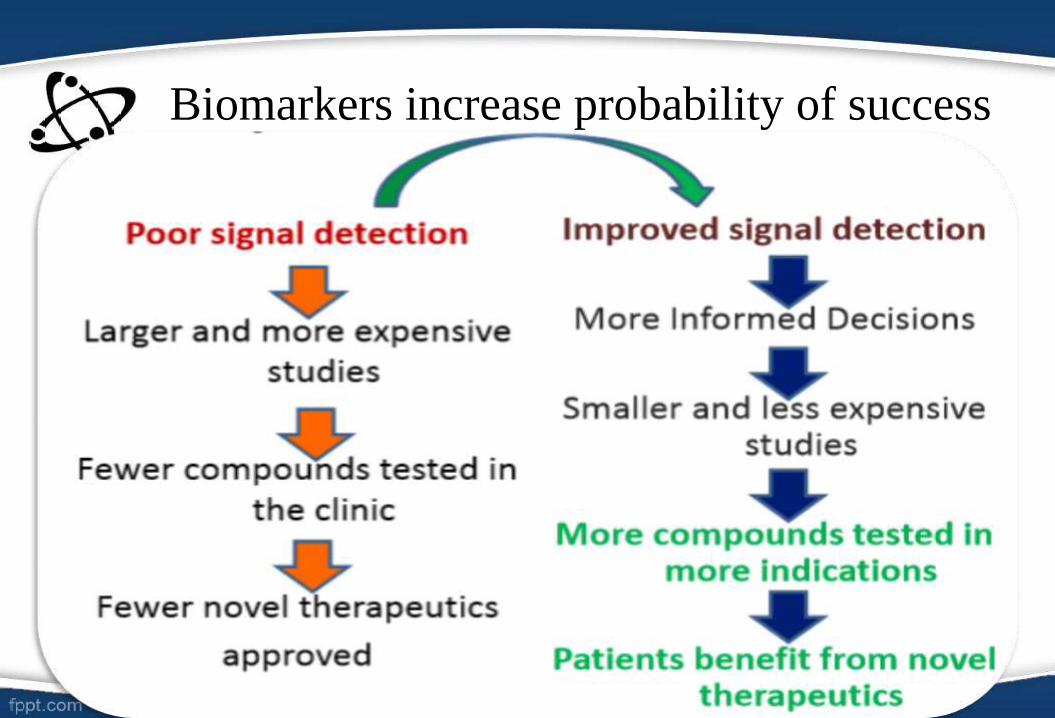
Biomarkers increase probability of success
Biomarkers
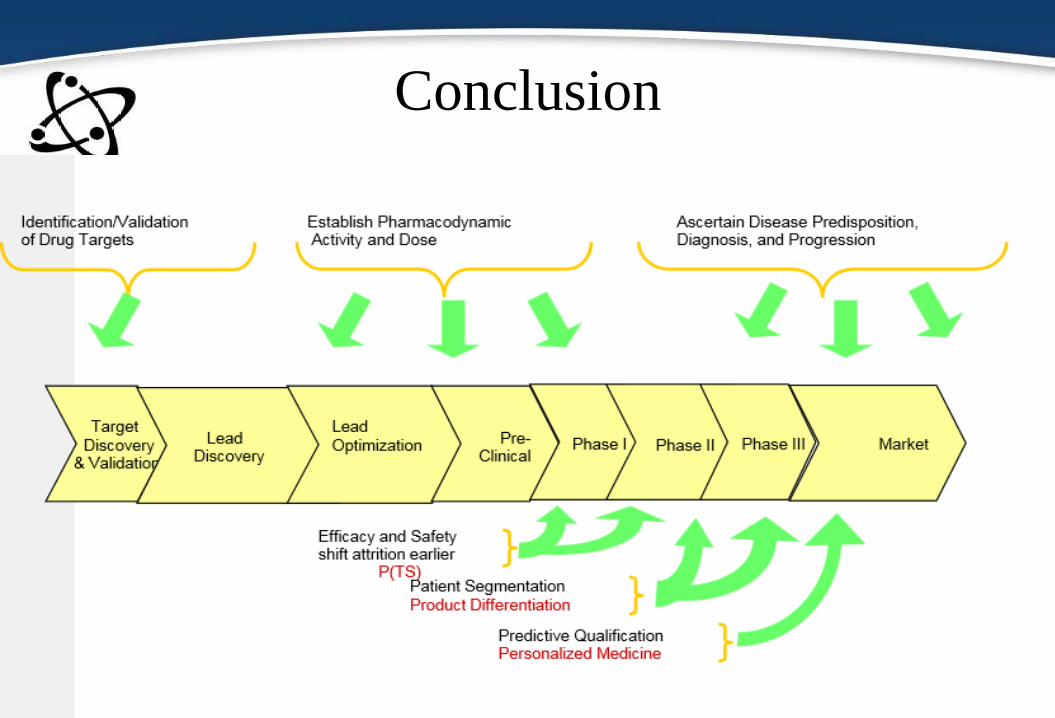
• In this review, focus is on
– Proximal and
– Distal markers
• In general, distal biomarkers are closer to disease
symptoms magnification for efficacy and off-target
indirect effects while;
• Target and proximal biomarkers are closer to the direct
exposure effect.
• Thus establishment of PD to PK is usually simpler for
proximal markers.
DIABETES TYPE 2
• Type 2 diabetes mellitus (T2DM)
– global epidemic characterized by high blood sugar (hyperglycemia)
– insulin deficiency and
– tissue resistance to insulin-stimulated glucose uptake and utilization.
• It is estimated that at least 170 million people worldwide have
diabetes, and this number is expected to double by 2030.
• In type 2 diabetes, the body becomes resistant to its insulin and
attempts to compensate by producing a higher quantity of insulin.
• Research has shown that chronically elevated blood glucose levels
(chronic hyperglycemia) over a long period of time can lead to
beta cells wearing out, referred to as beta cell turnover or beta
burnout.
• The mechanisms underlying loss of pancreatic B-cell
function in T2D is poorly understood.
• Defects in incretin hormone contribute to diminished B-cell
function.
• Incretin response due to
– Glucagon-Like Peptide-1 (GLP-1)
– Glucose-Dependent Insulinotropic Peptide (GIP)
DIABETES TYPE 2
DIABETES TYPE 2• DPP-4 is a Key Regulator of Incretin Activity; it inactivates the
hormone Incretin.
• Thus DPP-4 inhibitors (Gliptins) are used to block the action on
DPP-4.
• Sitagliptin is an orally active, potent and selective DPP-4 inhibitor.
• Advantages:
– oral administration;
– low incidence of hypoglycemia, similar to that of a placebo
– low incidence of adverse events, consisting of stomach
discomfort, diarrhea, upper respiratory infection, stuffy or runny
nose, sore throat and headache
– does not cause weight gain.
Application of Biomarkers
in Sitagliptin Clinical
Development Strategy
Sitagliptin - Januvia®
Mechanism of Action
• Used in diabetic patients
• Exert action by slowing the inactivation of incretin hormones.
• GIP and GLP-1 released by intestine in response to meal.
• These hormones are rapidly inactivated by the enzyme, DPP-4.
• Sitagliptin increases concentrations of GLP-1 and GIP thereby
increasing and prolonging the action of these hormones.
• Increased insulin release and decreased glucagon levels in the
circulation.
• Sitagliptin demonstrates selectivity for DPP-4 and does not inhibit
DPP-8 or DPP-9 activity in vitro at concentrations approximating
those from therapeutic doses.

Sitagliptin Activity
Sitagliptin - Januvia®
Preclinical studies• Studies in mice examined the decrease of blood level upon
administration of Sitagliptin.
• Maximun efficacy was obtained at a dose of 1mg/kg which
approximated to 46% inhibition.
• DPP-4 inhibition resulted in
– a 2- to 3-fold increase in circulating levels of active GLP-1 and
GIP,
– decreased glucagon concentrations, and
– increased responsiveness of insulin release to glucose
• From this, end points were obtained in clinical studies with
healthy subjects and patients with T2D.
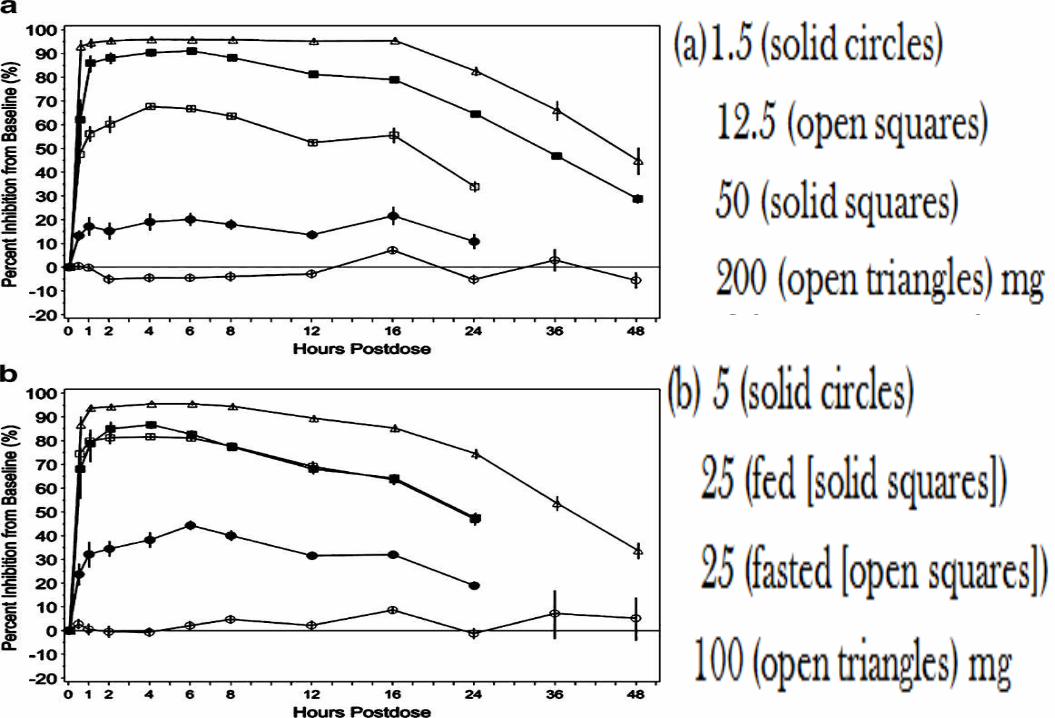
• The objective in this part of study was to investigate the
DDP4 inhibition of sitagliptin and GLP-1 stabilization.
• Sitagliptin was administered to normoglycemic healthy
subjects.
• Different single doses of sitagliptin were administered with
placebo acting as control (open circles).
• The extent of inhibition of plasma DPP4 activity was
analysed with respect to time in hours.
• A dose of at least 100mg has to be administered to obtain
80% or more inhibition over 24 hours A dose of at least.
Sitagliptin - Januvia®
Single dose clinical studies
• Sitagliptin increases levels of ACTIVE GLP-1 without increasing the
total levels of GLP-1; the ratio of active GLP-1 to total GLP-1 levels
increases.
• It stabilizes the active form of GLP-1 rather than increasing its secretion.
• Sitagliptin did not exert any effect on glucose, insulin, glucagon and C-
peptide.
• In healthy subjects, the decrease in blood glucose level was
insignificantly very small.
• It was reviewed that in diabetic patients, sitagliptin increases the level of
active GLP-1 leading to insulin secretion and thus reducing the blood
glucose level until normal.
Sitagliptin - Januvia®
Single dose clinical studies
• Sitagliptin improves glucose concentrations by causing
inhibition of DPP4 by more than 80% and in turn activating
more incretins.
• Sitagliptin increases post OGTT (oral glucose tolerance test)
levels of active GLP-1 and GIP and the ratio of active to total
GLP-1 levels and active to total GIP levels.
• Sitagliptin increased post glucose challenge insulin and C-
peptide levels and decreased post-glucose challenge glucagon
levels.
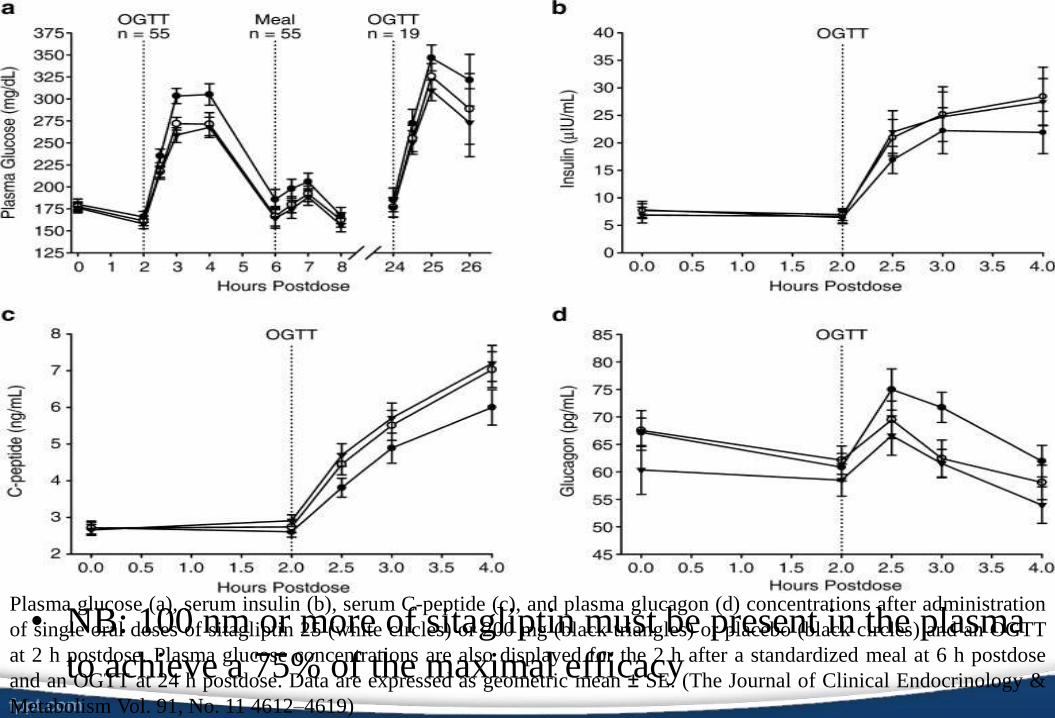
• NB: 100 nm or more of sitagliptin must be present in the plasma
to achieve a 75% of the maximal efficacy
Sitagliptin - Januvia®
Single dose clinical studies
Plasma glucose (a), serum insulin (b), serum C-peptide (c), and plasma glucagon (d) concentrations after administration
of single oral doses of sitagliptin 25 (white circles) or 200 mg (black triangles) or placebo (black circles) and an OGTT
at 2 h postdose. Plasma glucose concentrations are also displayed for the 2 h after a standardized meal at 6 h postdose
and an OGTT at 24 h postdose. Data are expressed as geometric mean ± SE. (The Journal of Clinical Endocrinology &
Metabolism Vol. 91, No. 11 4612–4619)
• During the multiple dose study in normal cases, both proximal and distal
biomarkers of DPP4 pathway were used.
– Proximal biomarkers indicate the immediate effect of the drug in its
target while
– Distal biomarkers demonstrate the effect of the drug downstream the
molecular target.
• It was found that the presence of Sitagliptin causes dose and concentration
dependence on the inhibition of plasma DPP4 activity but the inhibitory
level remains constant in both pre-clinical and clinical trials.
• Moreover, the relationship between Sitagliptin plasma concentrations and
inhibition of plasma DPP4 activity was not modified after multiple doses
as the EC50 values did not change.
Sitagliptin - Januvia®Multi dose clinical studies
Sitagliptin - Januvia®Multi dose clinical studies
• The pharmacodynamics effects of Sitagliptin with multiple doses
were also estimated in obese patients.
• The latter were treated twice daily with 200 mg Sitagliptin and this
led to a maximum inhibition of plasma DPP4 activity (90%).
• This means that the inhibition of DPP4 was maintained over a long
dosing period.
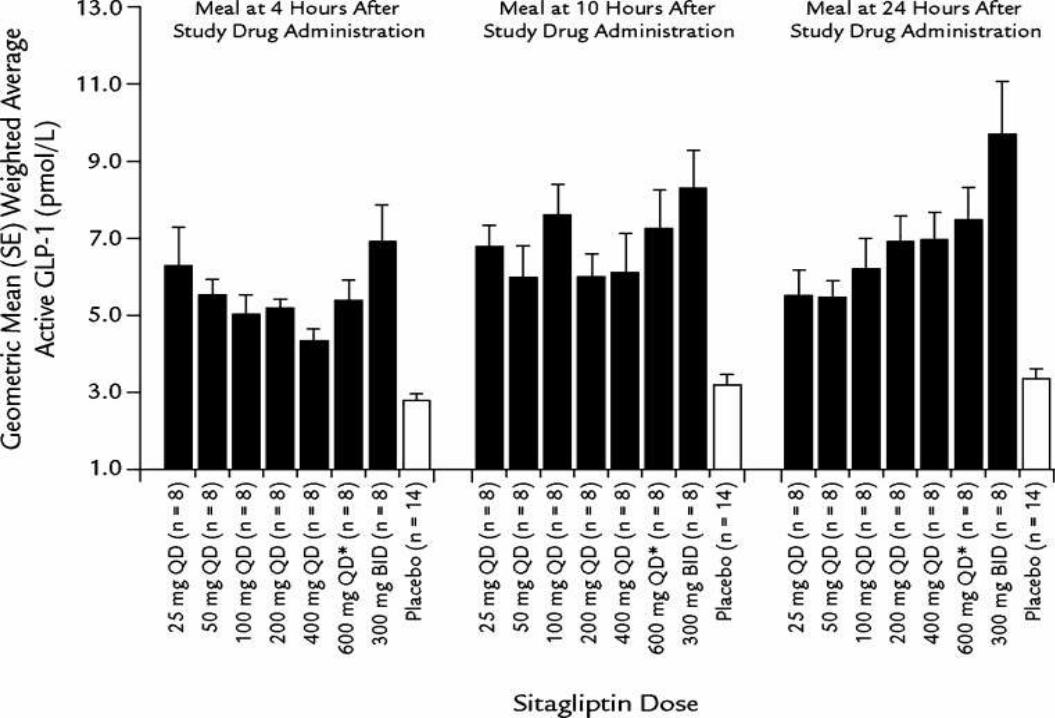
• Results show that the activation and rise in the level of GLP-1
increases OGTT by 2-3 times when compared to the placebo.
• Besides, the ratio of Sitagliptin: GLP-1 also increases by the same
amount.
• Concerning the patients, no weight gain was observed after a
treatment of 28 days.
Sitagliptin - Januvia®Special population
• DPP-4 proved to be a successful proximal and distal biomarkerto treat T2D.
• This biomarker helped in early clinical drug development fromwhich Sitagliptin was discovered.
• 100mg dose daily 80% inhibition reduction in HBA1c
• 50mg twice daily have benefits of achieving higher plasmaconcentration of Sitagliptin.
• The use of biomarker allowed Sitagliptin to reach Phase III in2.1 years instead of 3.5 years.
• Use of biomarker :- Simple exposure and increase efficiency ofdrug development.
Sitagliptin - Januvia®Acceterating Early Development
Conclusion
• The use of biomarker is advantageous for drug
development towards novel therapies.
• Sitagliptin can selectively act on DPP-4 to stimulate
insulin production.
• Sitagliptin is used along with diet and exercise and
sometimes with other medications to lower blood
sugar levels in patients with type 2 diabetes.
References• http://www.diabetes.co.uk/body/beta-cells.html
• Biomarkers in Drug Development: A Handbook of Practice,
Application, and ...by Michael R. Bleavins, Claudio Carini, Mallé
Jurima-Romet, Ramin Rahbari
• http://www.currentseparations.com/issues/21-1/cs21-1e.pdf
• http://www.globalrph.com/DPP-4-inhibitors.htm
• FASOLO, A. and SESSA, C., 2001. European Society for Medical
Oncology. The use of biomarkers for treatment decisions in oncology
[online]. Available from:
http://oncologypro.esmo.org/content/download/22272/368716/file/The-
use-of-Biomarkers-for-Treatment-Sessa-Fasolo.pdf [Accessed on 24
January 2015].






























