Embed Size (px)
Citation preview
Preterm Labor
Saeed esmailian
Kerman University of Medical Sciences
DefinitionDefinition
regular uterine contractions
by progressive cervical dilation and/or effacement at less than 37 weeks
Significance
Preterm birth is the leading direct cause of neonatal death (death in the first 28 days of life).
It is responsible for 27 percent of neonatal deaths worldwide, comprising over one million deaths annually
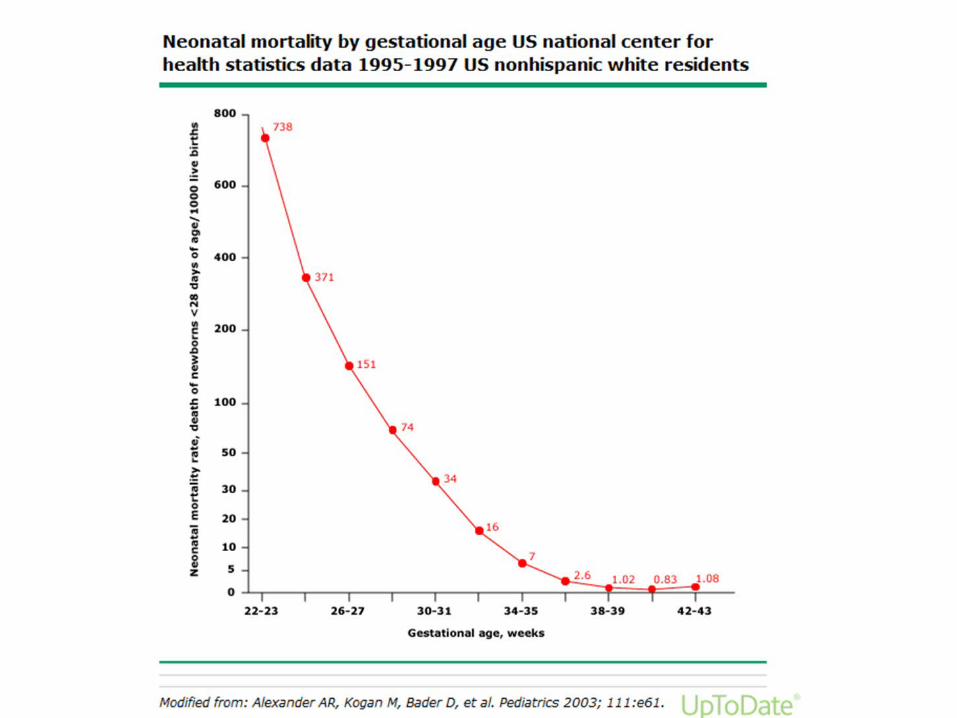
The risk of neonatal mortality decreases as gestational age at birth increases, but the relationship is nonlinear (figure 1
preterm birth is the second most common cause of-death (after pneumonia) in children younger than 5 years.

Survival in Premature Infants
survival chance is directly proportional to the maturity
26 wks – 80%27 wks – 90%28-31 wks – 90 to 95%
32-33 wks – 95%34-36 wks – approaches term survival rates
Complications of PrematurityComplications of Prematurity RDS IVH Feeding difficulties/NEC Apnea PDA Infection Jaundice Hypothermia Neurobehavioral ROP Anemia
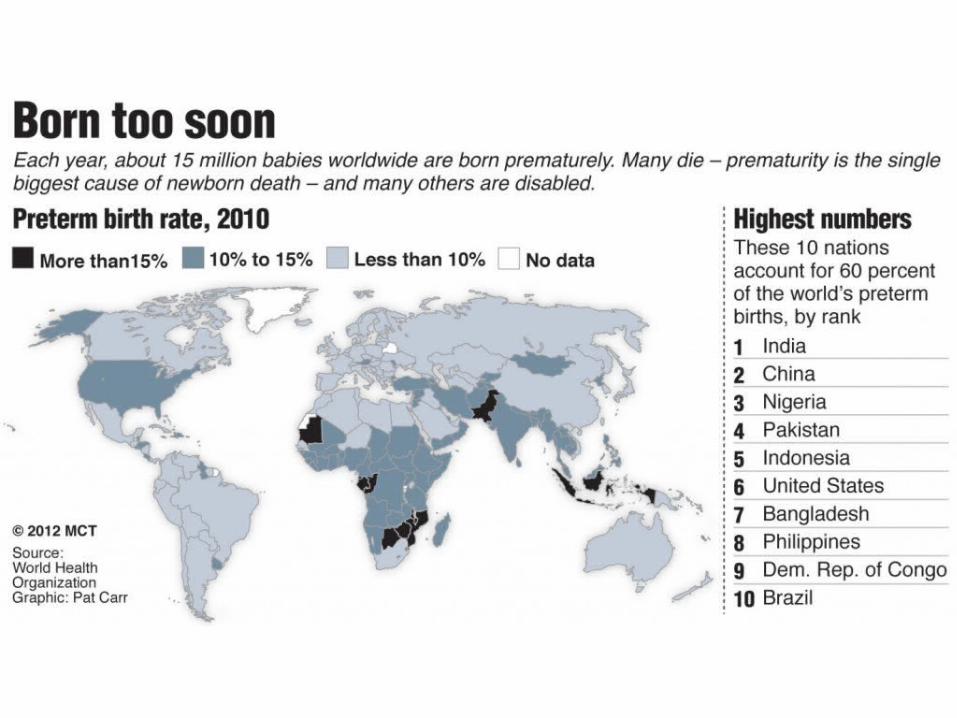
Prevalence
Worldwide11 percent (range 5 percent [parts of Europe] to 18 percent [parts of Africa]),
15 million children each year (range 12 to 18 million)
United States in 2011, 11.73 percent


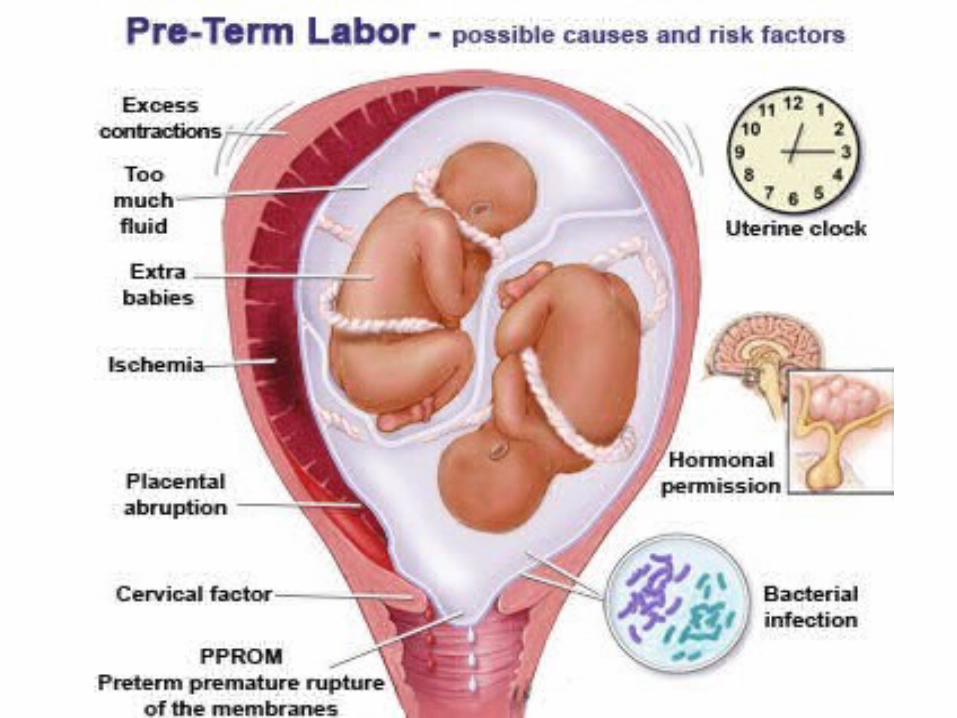
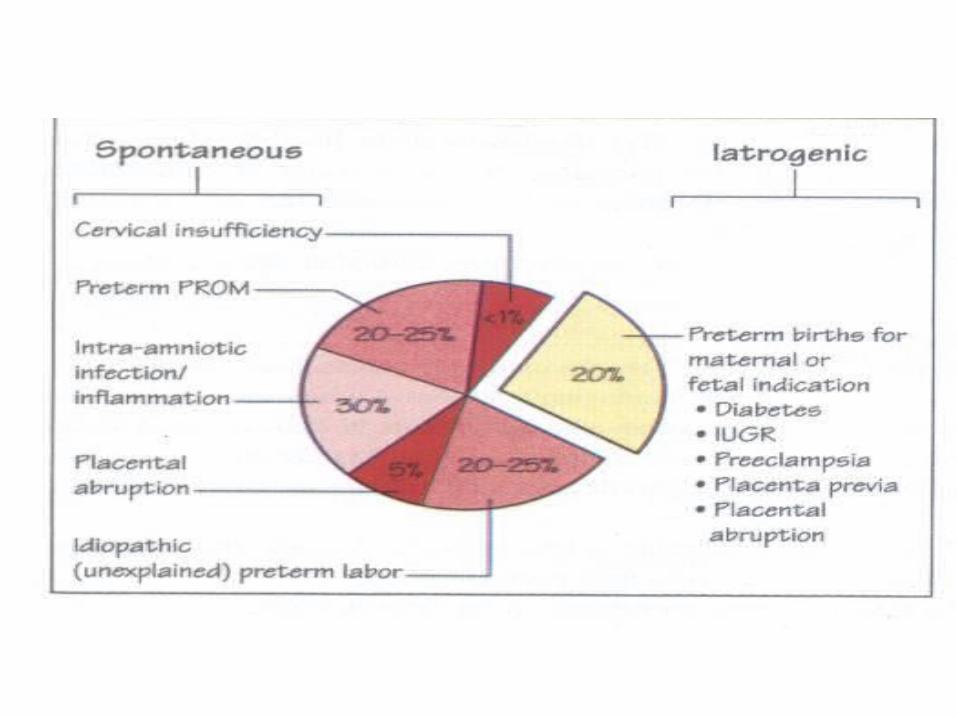

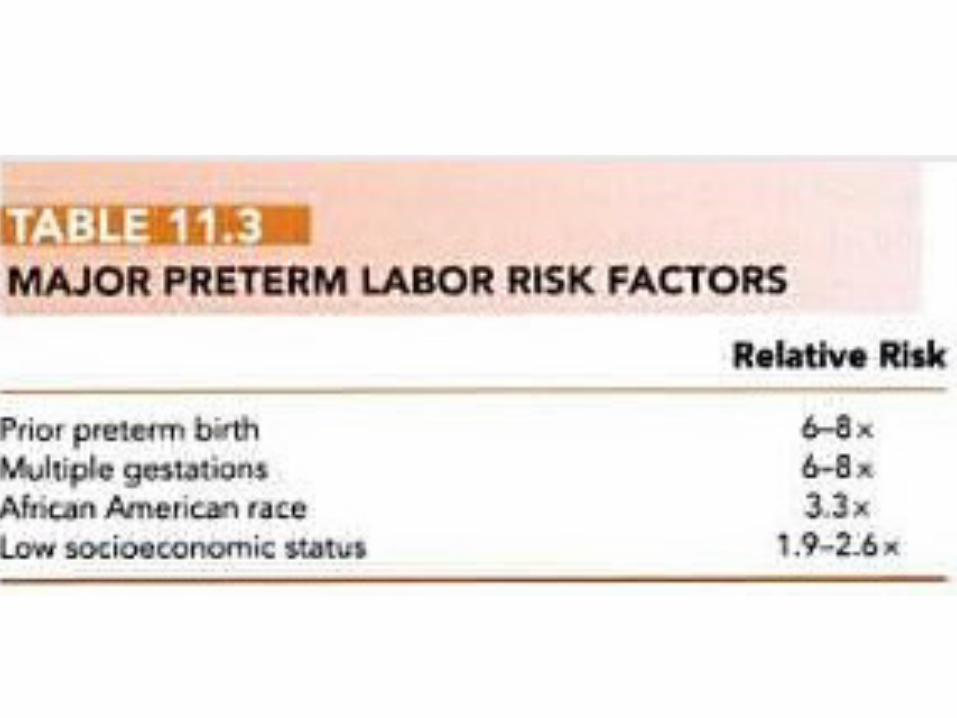
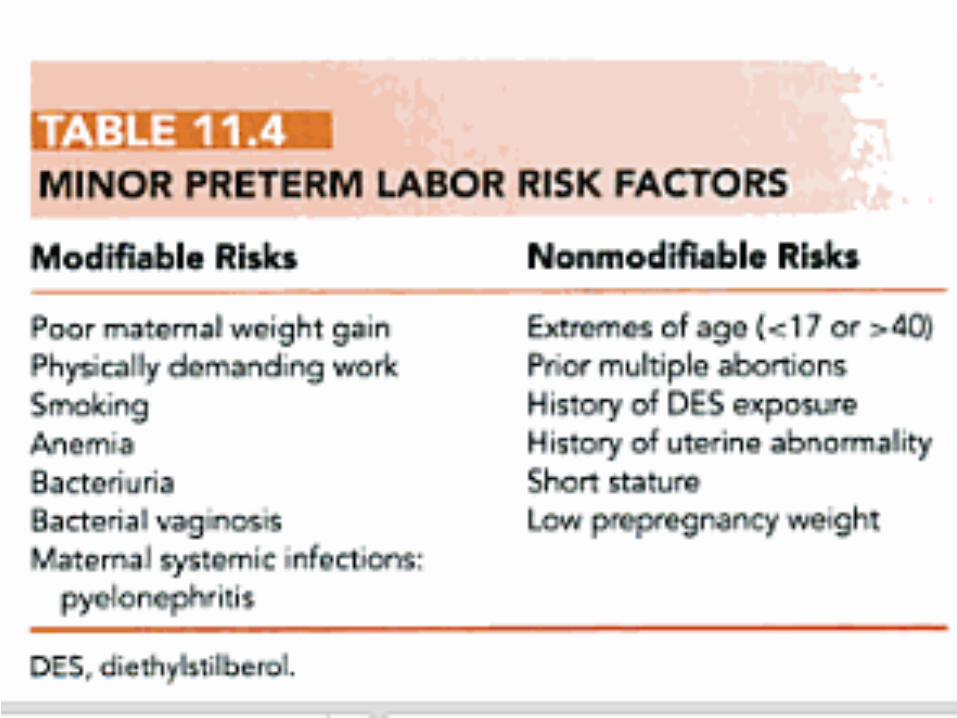
Risk Risk factorsfactors

Signs and symptomsSigns and symptoms
1. Painful or painless uterine contractions
2. Menstrual-like cramping3. Mild, irregular contractions4. Low back ache5. pressure sensation in the vagina6.6. Vaginal discharge Vaginal discharge of mucus, which
may be clear, pink, or slightly bloody (ie, mucus plug, bloody show)
Diagnostic critiriaDiagnostic critiria
Uterine contraction Uterine contraction 4 in 20 mins8 in 60 mins with cervical change
Cervical dilatation > 1 cmCervical effacement > 80%
Initial evaluation
Maternal vital signs:(temperature, blood pressure, heart rate, respiratory rate) Fetal monitoring:
fetal heart rate and contraction (frequency /duration /intensity)
Uterine contractions are evaluated continuously using a contraction monitor, palpation, and the patient’s subjective assessment.
patient’s past and present obstetrical and medical history and GA
Examination of the uterusfirmness, tenderness, fetal size, and fetal position.
Initial evaluation
Speculum examination using a wet non-lubricated speculum
cervical dilation and effacement uterine bleeding (abruptio placenta or placenta previa) fetal membranes, ( intact or ruptured) fetal fibronectin (fFN). bactrial culture (B streptococcal,gonorrhea and
chlamydia)
Fetal FibronectinFetal Fibronectin (fFN)- it is a glue like protein binding choriodecidual membrane
Present in vaginal secretions between 23-34 weeks and signifies onset of labor
Bedside test can be done – if negative it rules out preterm labor in next two weeks
P/V examination gives false positive result for 24 hours
Between 24-32 weeksfFN – 25ng/ml + cervical length of 25 mm shows significant risk
Initial evaluation
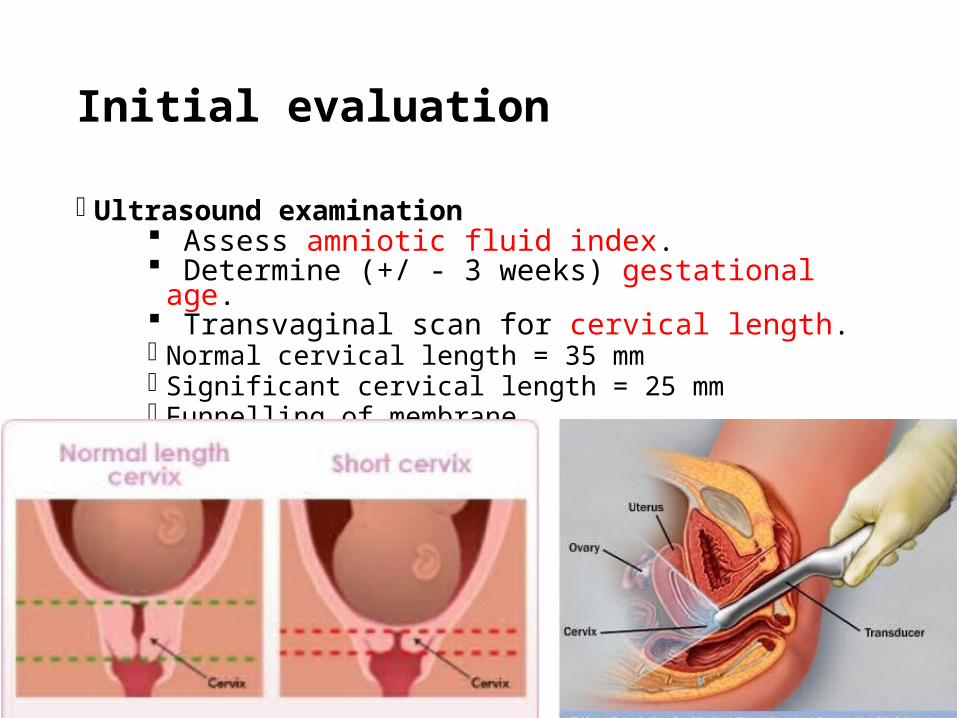
Ultrasound examination Assess amniotic fluid index. Determine (+/ - 3 weeks) gestational age. Transvaginal scan for cervical length. Normal cervical length = 35 mm Significant cervical length = 25 mm Funnelling of membrane

Management
1. BBetamethasone (24- 34w)etamethasone (24- 34w)
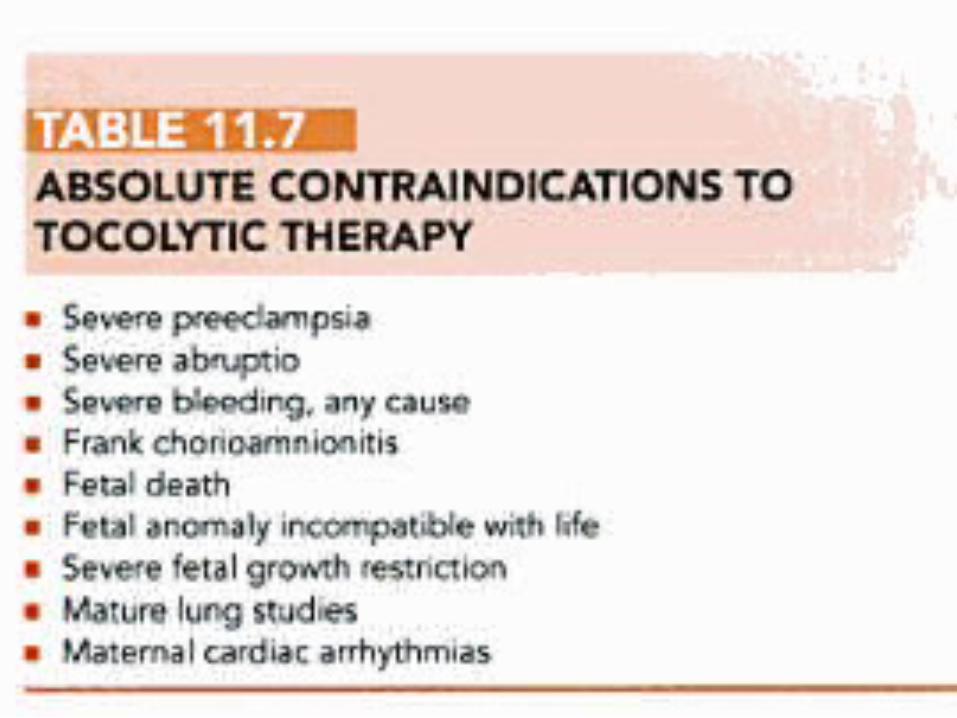
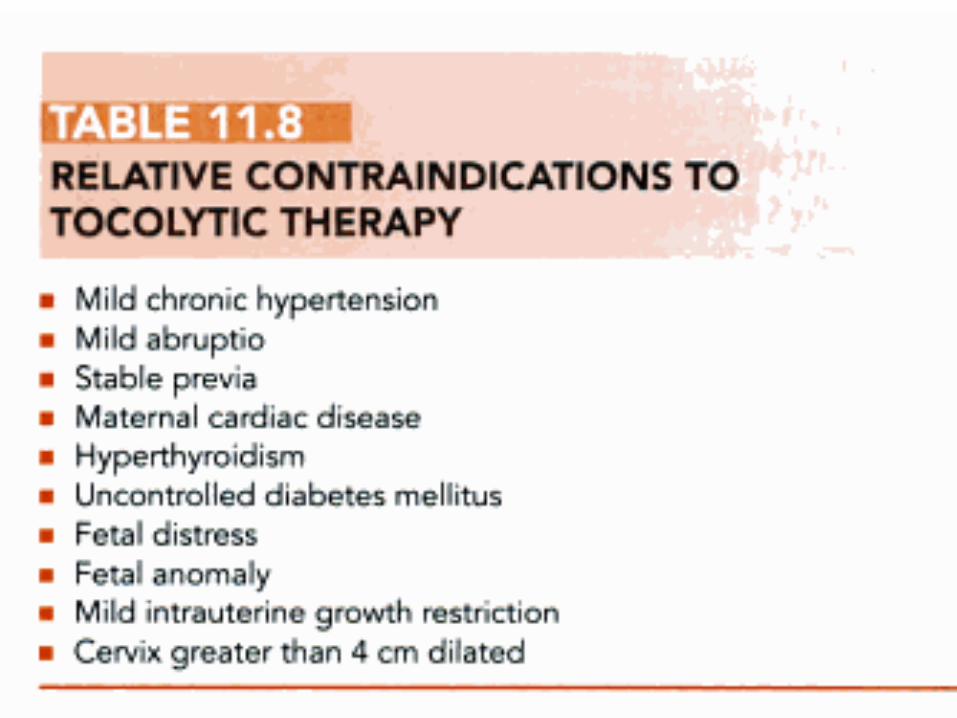
2.2. Tocolytic drugs (before 34w)Tocolytic drugs (before 34w) for up to 48 hours
3.3. AntibioticsAntibiotics ( GBS chemoprophylaxis, Appropriate antibiotics to women with positive urine culture results)
Bed rest (+) Hydration (-) Emergency cerclage (+)
Glucocorticoid
BetamethasoneBetamethasone
12mg IM stat and 24 hours later
Effective: 24 hours after initial doseEffect up to 7 days
Adverse effect: Pulmonary edema Infection Difficult glucose control in DM women
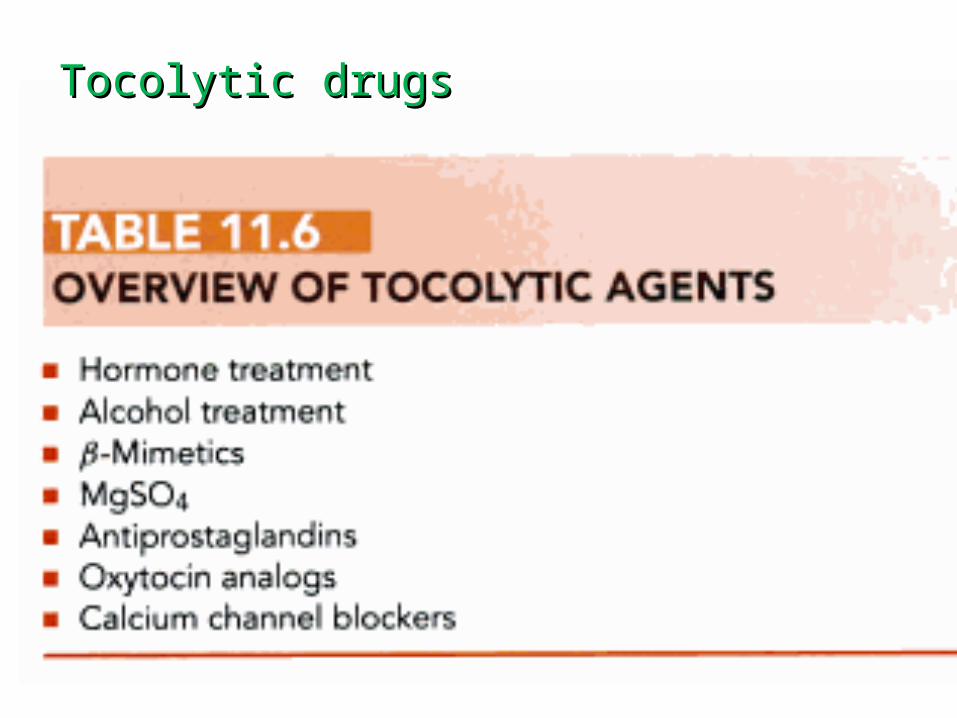
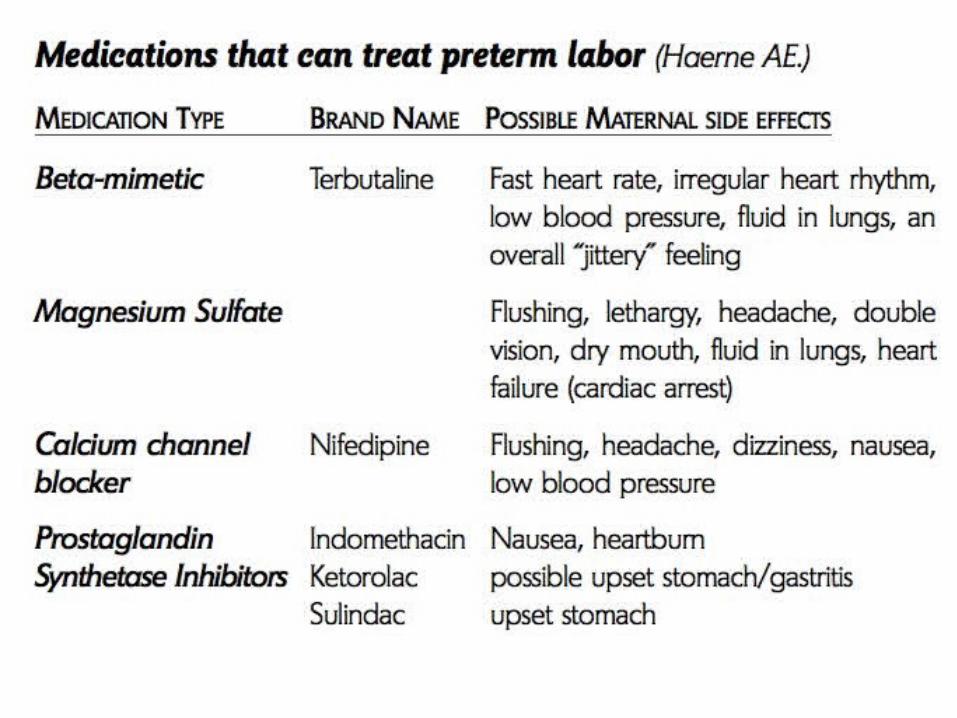
Tocolytic drugsTocolytic drugs
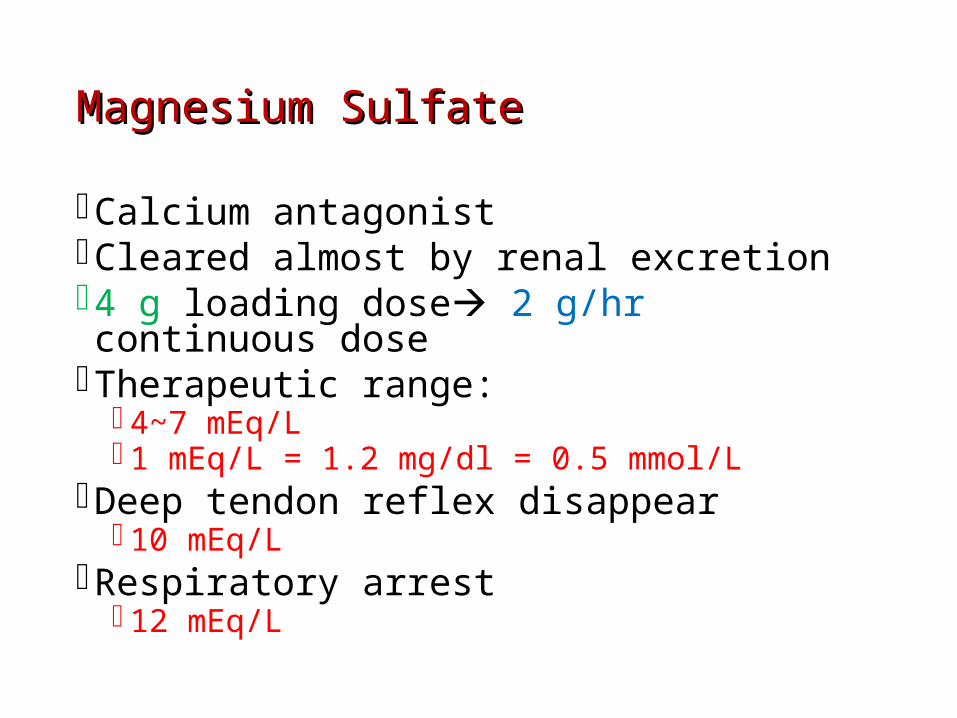
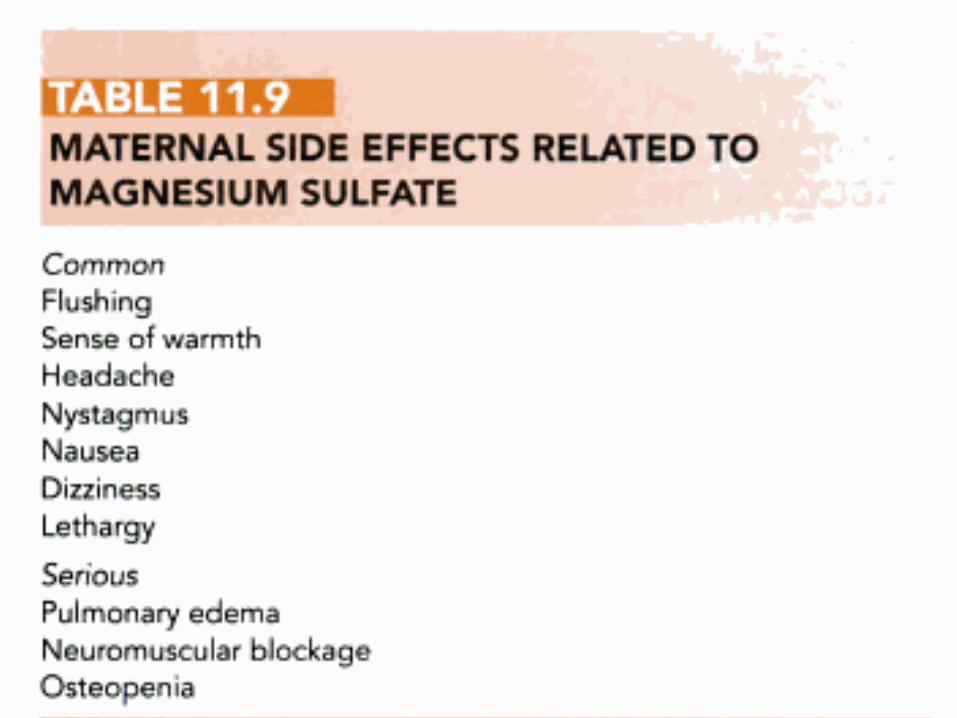
Magnesium SulfateMagnesium Sulfate
Calcium antagonistCleared almost by renal excretion4 g loading dose 2 g/hr continuous doseTherapeutic range:
4~7 mEq/L 1 mEq/L = 1.2 mg/dl = 0.5 mmol/L
Deep tendon reflex disappear 10 mEq/L
Respiratory arrest 12 mEq/L

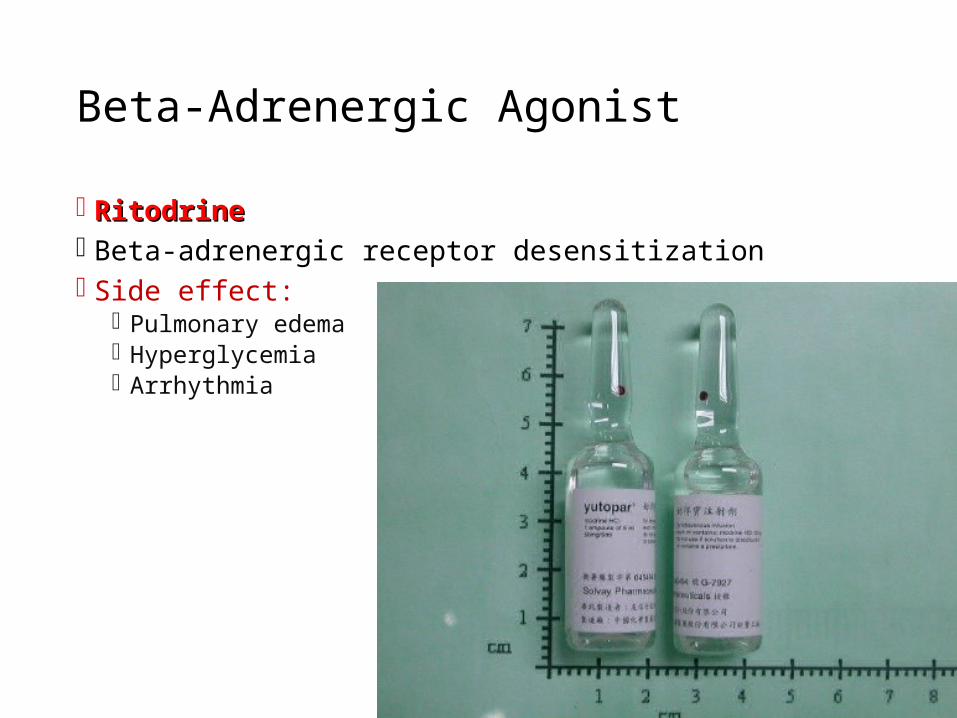
Beta-Adrenergic Agonist
RitodrineRitodrine Beta-adrenergic receptor desensitization Side effect:
Pulmonary edema Hyperglycemia Arrhythmia
Prostaglandin Inhibitors (Nsaid)
IndomethacinIndomethacin< 48 hours
< 30-32 weeks' gestation)
Not > 200mg/day.
Side effect: Oligohydramnios (reversible)
Prostaglandin Inhibitors (Nsaid)
Capsule 25mg oral Amp 50mg
Rectal Supp 100 mg
50 mg Loading dose
Then 25-50mg /6hs
Calcium Channel Blockers
Nifedipine (adalat)Nifedipine (adalat)
Higher delaying of delivery for >48 H.
Lower risk of RDS &Neonatal jundice.
Lower admission to NICU
Fewer maternal adverse effects
Side effect: Hypotension Decrease uteroplacental perfusion
Dose:
20mg initial
10-20 mg /4-6 h
Available forms
Adalate capsule : 10mg
Adalate retard Tablet: 20 mg
Atosiban
Nonapeptide oxytocin analogue Competitive antagonist of oxytocin-induced
contractions Side effect:
Nausea, vomiting, headache, dizziness, money loss 18000 NTD/day

Reffrences
thanks