Embed Size (px)
Citation preview
BORNEO NEUROSURGERY CONFERENCE 2014 • “CRANIAL & SPINAL EMERGENCIES” • 17-18 OCT • PALACE HOTEL, SABAH
Dr. Wan Najwa Zaini Wan Mohamed Radiologist, HQE 2


1. INTRODUCTION2. IMAGING TECHNIQUES3. TYPES OF HEAD INJURIES
A. PRIMARY HEAD INJURY
B. SECONDARY HEAD INJURY
4. SEQUELAE OF HEAD TRAUMA5. CONCLUSION
Traumatic brain injury (TBI) – leading cause of death in children and young adults.
Peak age – 15 -24 yrs. Secondary peak > 50 years of age. Twice as often among males compared to
females. Generally caused by motor vehicle accidents,
fall, assaults, violence and sports & recreation
Can be classified into primary and secondary injuries.
By location – Intra or extra-axial. By mechanism – penetrating/open or
blunt/closed. By severity – minor, mild, moderate, or
severe using Glasgow Coma Scale score.
1. SKULL RADIOGRAPH Poor predictors. Normal SXR does not exclude major
intracranial injuries.

2. CT SCAN Most important step in evaluation of head
trauma. Modality of choice – fast, widely available,
and highly accurate in the detection of skull fractures and intracranial hemorrhage.
Goal of imaging is to identify treatable injuries to prevent secondary damage.

Indications – severe TBI (GCS ≤8)
persistent neurologic deficit
antegrade amnesia
unexplained asymmetric pupillary response
LOC > 5 minutes
depressed skull fracture
penetrating injury
bleeding diathesis or anticoagulation therapy.
In a typical TBI, CT images must be reviewed using multiple windows and levels:
1) Brain window (W: 80, L: 40)
2) Intermediate window : to exaggerate contrast between extra-axial blood and the adjacent skull (W: 150, L: 75)
3) Bone window : to evaluate the osseous structures (W: 2500, L: 500).

3. MRI Recommended for patients with acute TBI
when the neurologic findings are unexplained by CT.
Valuable to show small/subtle extra-axial blood collections, diffuse axonal injury, brainstem injuries.
Higher sensitivity in the sub-acute and chronic stages of head trauma.
A. PRIMARY HEAD INJURY
1. Scalp injury, skull vault, base of skull fracture.
2. Primary haemorrhages:
a) Extra-axial – epidural, subdural, subarachnoid, intraventricular
b) Intra-axial – diffuse axonal injury (DAI), cortical contusions, intracerebralhaematoma, deep/ brainstem injury
3. Primary vascular injuries:
a) Traumatic arterio–venous fistula (AVF)
b) Carotid-cavernous fistula (CCF)
c) Arterial pseudo-aneurysm
d) Arterial dissection/ laceration/ transaction/ occlusion
e) Dural sinus laceration/thrombosis/occlusion
f) Cortical vein rupture/thrombosis
4. Other : cranial nerve injury.
B. SECONDARY INJURY
a) Cerebral herniation
b) Traumatic ischemia, infarction
c) Diffuse cerebral swelling
d) Diffuse hypoxic injury
e) Secondary “delayed’’ hemorrhage
f) Secondary brain stem injury or haemorrhage
g) Others e.g. fatty embolism , infection
1. SCALP INJURY, SKULL FRACTURE
SCALP INJURY Soft-tissue lacerations Subgaleal hematoma most common manifestation
focal soft-tissue swelling beneath subcutaneous tissue and above the temporalis muscle and skull.
Cephalohematoma Residual foreign bodies

SKULL VAULT FRACTURE Could be linear, depressed or diastatic Depressed fracture usually associated with
intracranial injury Diastatic fracture/ sutural diastasis
Seperation of cranial bones at suture site
Width of the suture > 3 mm (normal < 2 mm)
In adults, most common site is lambdoid suture
BASE OF SKULL FRACTURE Should be sought when blood behind
tympanic membrane, otorrhoea, rinorrhoea, echymosis surrounds the orbits without direct orbital trauma, intracranial air, air fluid level in PNS or mastoid air cells.
Basilar fracture cause compression or entrapment of cranial nerves.
Fracture of optic canal cause loss of vision.
Sphenoidal fractures can cause disruption of intra- cavernous internal carotid artery, leading to pseudo- aneurysm or a carotid cavernous fistula.
Petrous temporal bone fracture Transverse or longitudinal (relative to long axis of
bone) Longitudinal – direct temporal impact, 70% Transverse – occiput or frontal impact Can cause hearing loss from ossicular bone fracture/
dislocation, otorhinorrhoea from CSF leak, facial nerve palsy, vascular injury, perilymphatic fistula

2. PRIMARY HEMORRHAGES
a) EXTRA-AXIAL HEMORRHAGES
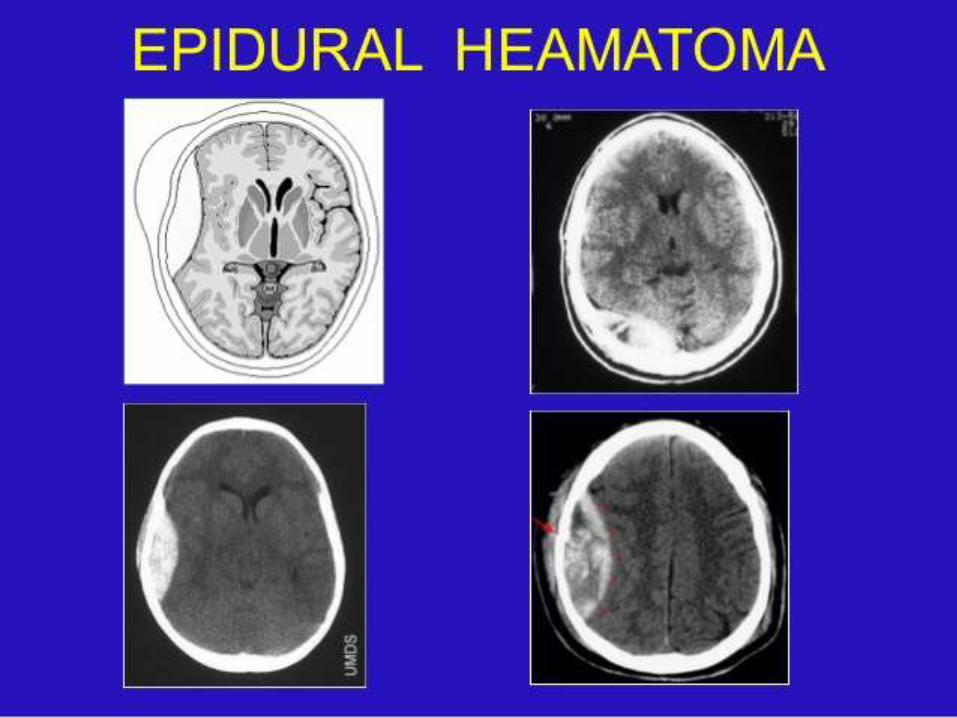
EXTRA/EPIDURAL HEMATOMA (EDH) Usually within first 24-48 H. Occurs between the inner table of the skull and
the dura with a biconvex configuration. Etiology – disruption of middle meningeal
artery, laceration of diploic veins or dural sinus.
May cross dural attachments but not sutures. Usually associated with overlying skull fracture
and secondary intracranial mass effect/ injuries. Can be acute, subacute and chronic. Hypodense area within indicates active bleed. Imaging criteria where EDH may be treated
conservatively:(1) Diameter less than 1.5 cm
(2) Minimal mid line shift < 2 mm
(3) Neurologically intact without focal deficit.

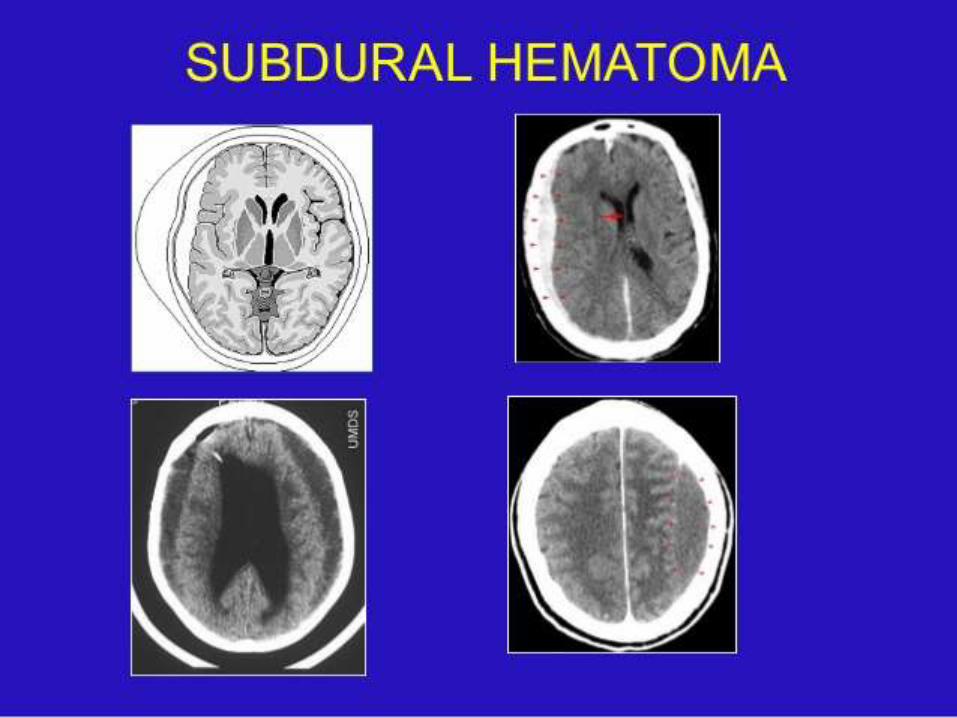
SUBDURAL HEMATOMA (SDH) Interposed between the dura and arachnoid. Typically crescent shaped with concave
medial and convex lateral border. May cross suture lines but not dural (falx or
tentorial) attachments. Common sites: over the fronto-parietal
convexities, middle cranial fossa, para- falcialarea, inter- hemispheric fissure.

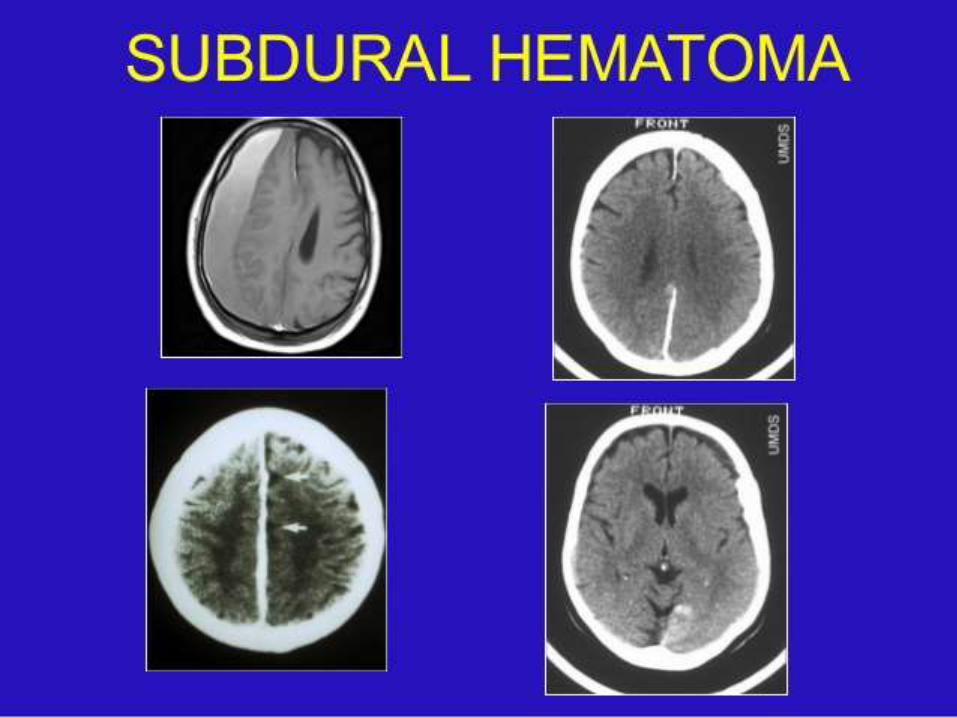
Acute SDH – homogenously hyperdense, up to 40% mixed hyper/ hypodense due to unclottedblood - serum extruded during clot retraction.
Subacute SDH – isodense within a few days to a few weeks, may be difficult to diagnose, wider window helpful.
Chronic SDH – typically low attenuation, mixed density in 5% due to recurrent haemorrhage, enhancement in post contrast, calcification in 0.3 to 2.7% cases.

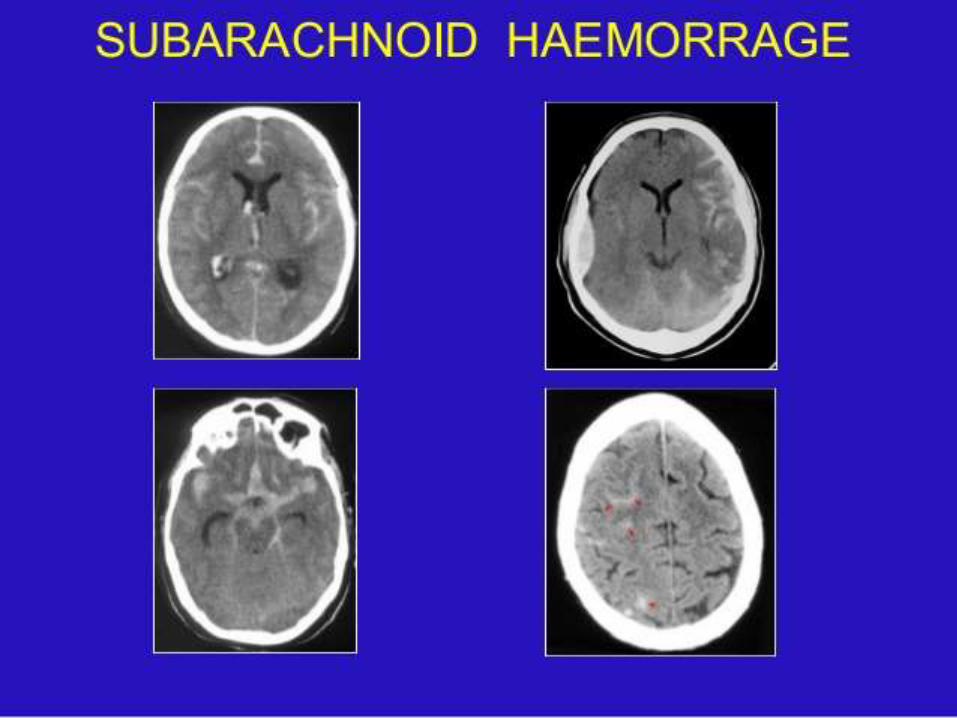
SUBARACHNOID HAEMORRHAGE (SAH) Can result from the disruption of small pial
vessels, extension into the subarachnoid space by a contusion or hematoma or diffusion of intraventricular hemorrhage.
Very common, but rarely causes mass effect. Typically appears as linear or serpentine area
of hypendensity in the basal cisterns, the sulci, the Sylvian fissure and inter-hemispheric fissure.
Normal calcified or ossified falx may be mistaken for parafalcine SAH in older adolescents.
“Pseudo sub-arachnoid haemorrhage” is seen in cases of severe diffuse cerebral oedema.
Posterior parafalcine or inter-hemispheric SAH can mimic the “Empty delta sign’’ of superior sagittal sinus thrombosis.
Rapidly cleared within 1 week.

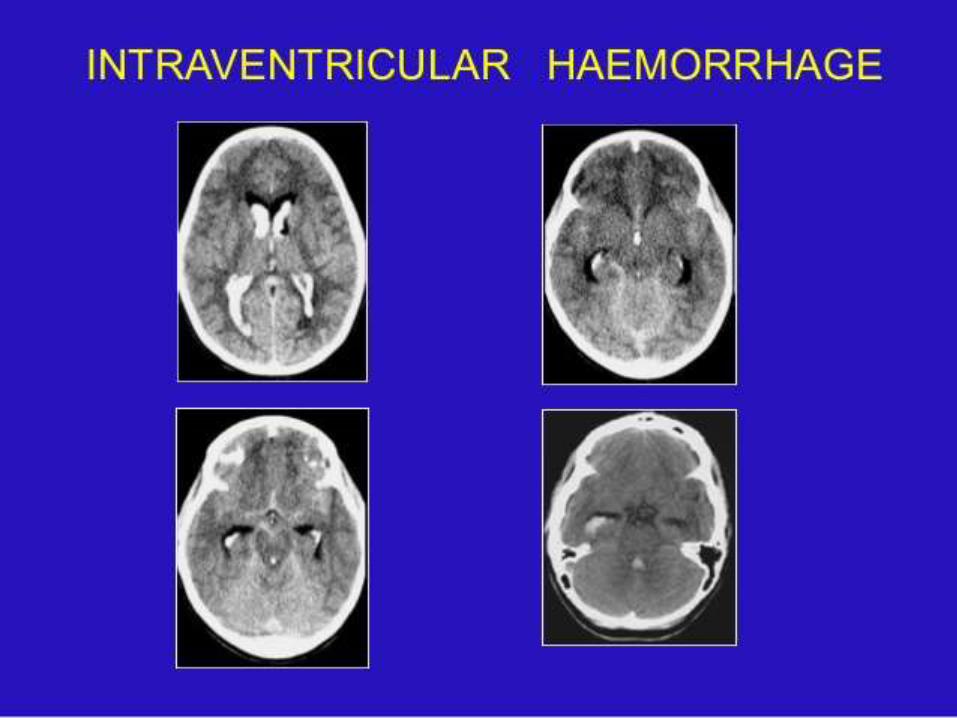
INTRAVENTRICULAR HEMORRHAGE (IVH) Can result from rotationally induced tearing
of subependymal veins along the surface of the ventricles, by direct extension of a parenchymal hematoma into the ventricular system or from retrograde flow of SAH into the ventricular system via the fourth ventricular outflow foramina.
Shows high density intraventricular bloodwith or without a fluid level.
Occasionally focal choroid plexus hematoma noted.
At risk for developing both communicating and non communicating hydrocephalus secondary to obstruction and ependymitisfrom the irritant effects of the blood.
2. PRIMARY HEMORRHAGES
b) INTRA-AXIAL HEMORRHAGES
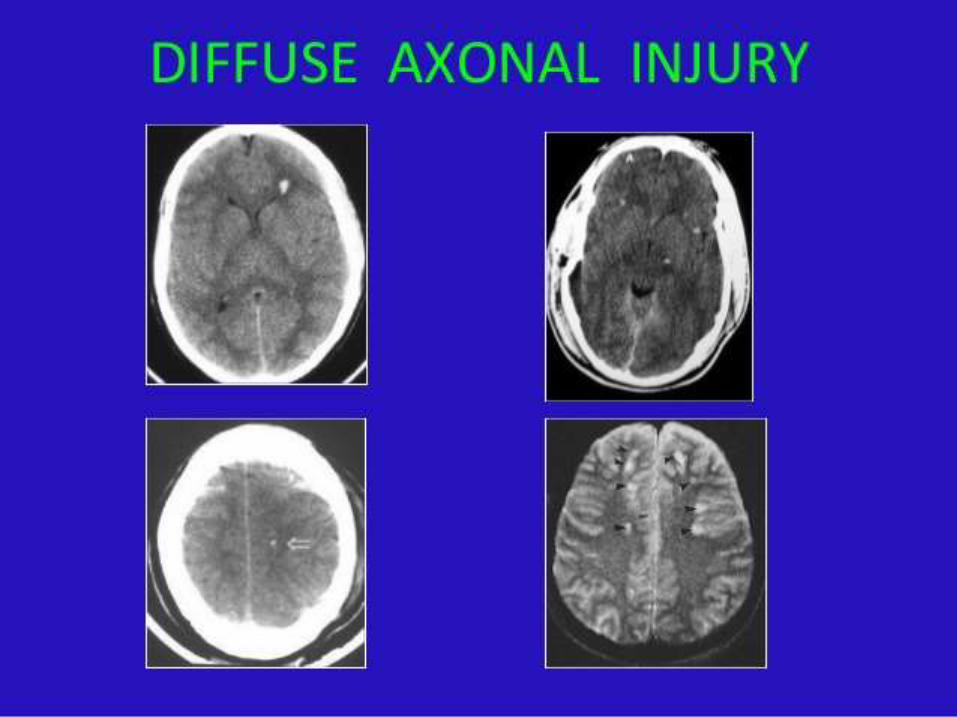
DIFFUSE AXONAL INJURY (DAI) Most common type of primary traumatic
injury. Results from rotational acceleration and
deceleration forces that produce shearing deformations of brain tissue.

Disruption of accompanying blood vessels show numerous small hemorrhage foci.
Diffuse & bilateral. Clinically, characterized by loss or severe
impairment of consciousness beginning at the moment of direct impact.
In chronic stage can result in overwhelming cognitive and psychiatric problems.
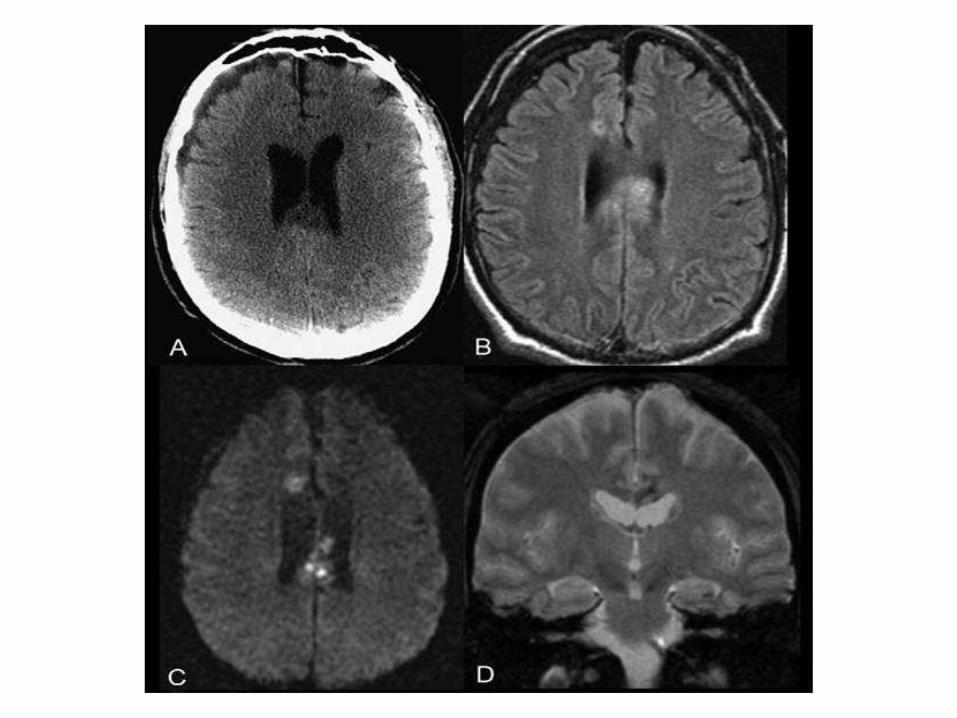
MRI more superior to CT to detect DAI.
CT findings: Early imaging may be subtle or normal.Foci of decreased density.May show some degrees of cerebral swelling.May show small focal hemorrhage or small
petechial haemorrhage particularly at the gray-white junction and corpus callosum.
May show extensive injury.
Locations ( according to severity of trauma):Peripheral lobar white matter at cortico-
medullary junction.Common at the parasagital regions of frontal
lobe, periventricular regions of temporal lobe. Internal & external capsules, corona radiata,
cerebral peduncles. Corpus callosum.Brain stem – posterolateral quadrants of mid
brain and upper pons.
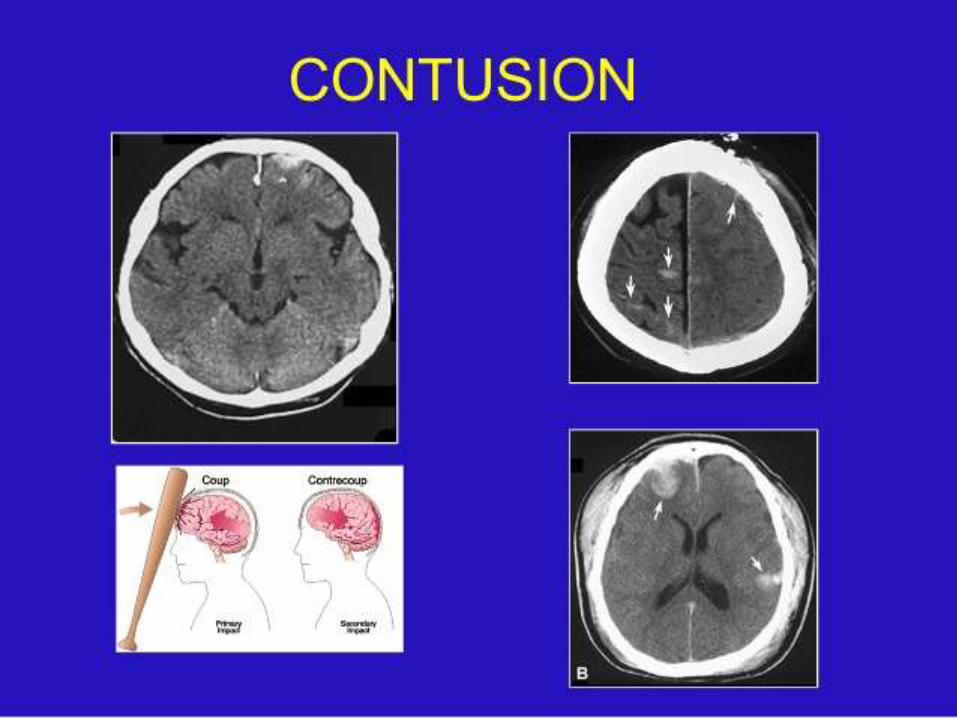
CORTICAL CONTUSION Common type, in 21% of TBI patients. Mechanism: linear acceleration-deceleration
forces /penetrating trauma /direct impaction. Tissue necrosis, capillary disruption, petechial
hemorrhage followed by liquefaction and oedema after 4 to 7 days.
May be hemorrhagic or non-hemorrhagic.
Coup: Direct impact to stationary brain. Injury at the site of impaction.
Counter coup: Impact of moving brain on stationary clavarium opposite to the site of the coup and produced injury.
Focal lesion primarily involving superficial gray matter, with relative sparing of the underlying white matter.
Location – orbitofrontal and temporal lobesmost frequently involved.
Beneath an acute subdural hematoma or a depressed skull fracture.
Associated with a better prognosis than DAI, unless accompanied by brainstem injury or significant mass effect.
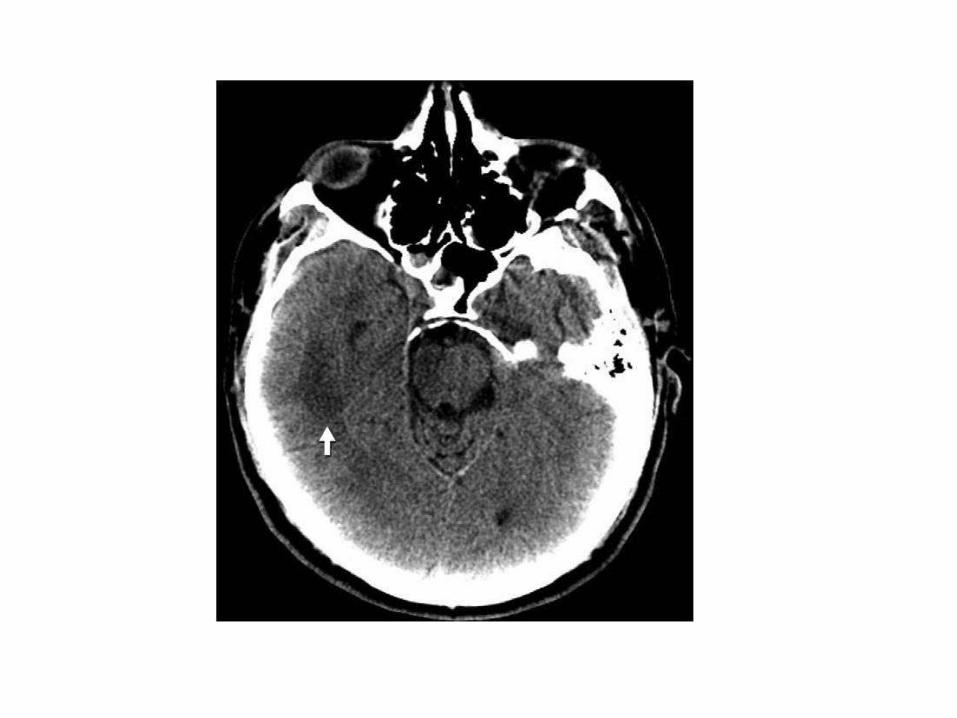
CT findings: Initially may be subtle or absent. Early findings –characteristic “salt and pepper”
pattern of focal /multiple poorly defined mixed areas of hypodensity and hyperdensity(petechial hemorrhage).
Diffuse oedema and mass effect in immediate post-traumatic period, then gradually diminish over time.
Some degree of contrast enhancement. Isodense to brain after 2 – 3 weeks.

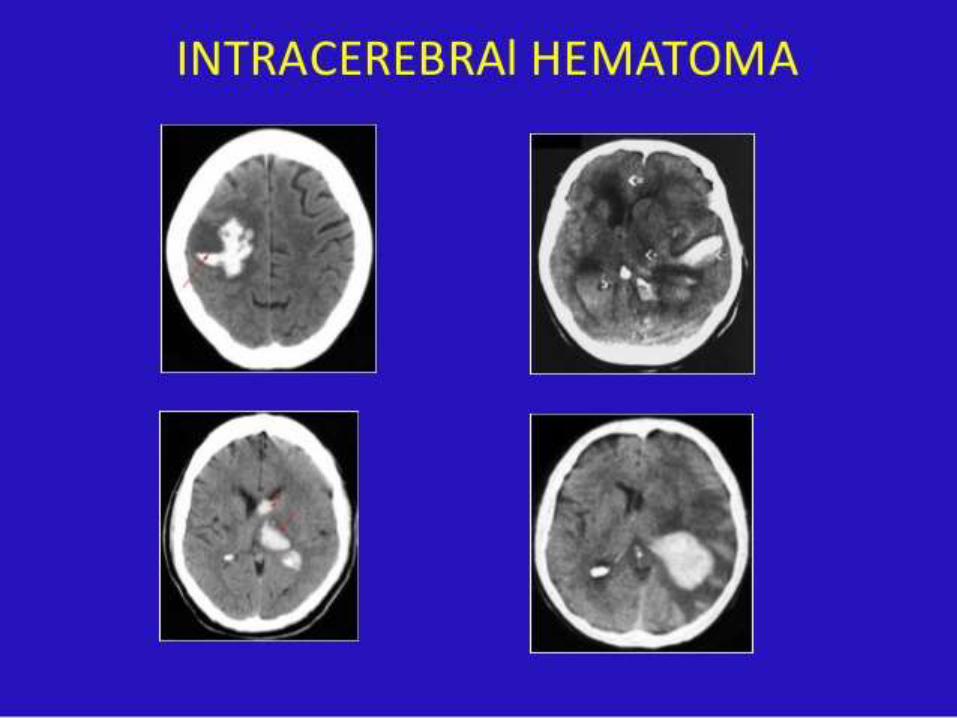
INTRACEREBRAL HEMATOMA Frequently associated with other primary
extra- and intra-axial injuries. May be delayed with 48 hours (lucid) interval. Due to shear-induced hemorrhage from
rupture of small intraparenchymal vessels. Differentiated from hemorrhagic contusion
by sharply marginated margin, perifocalhypodensity and mass effect.
Mostly located in the frontotemporal white matter, other site basal ganglia
Acute hematoma (< 3 days):CT: Homogenous high density lesion (50 -70
HU) with irregular well-defined margins. Usually surrounded by low attenuation area (oedema, contusion) with mass effect.

Subcute Hematoma (3 – 14 Days):NCCT: Gradual decrease in density from
periphery inward and becomes isodense to brain parenchyma.
CECT: Peripheral rim enhancement at inner border of perilesional lucency.

Chronic Hematoma (> 14 Days):CT: Gradual decreased attenuation/
hypodensity.Later – lucent hematoma (cephalomalacia
due to proteolysis and phagocytosis & surrounding atrophy) with adjacent sulcalenlargement and ventricular dilation with ring blush ( DDX : tumor )

3. PRIMARY VASCULAR INJURIES Traumatic arterio–venous fistula (AVF). Carotid cavernous fistula (CCF). Arterial pseudo-aneurysm. Location: branches
of ACA+MCA, Cavernous portion of ICA. Arterial dissection/laceration/ transection/
occlusion. Dural sinus laceration/ thrombosis / occlusion. Cortical vein rupture / thrombosis.
Most often injured artery is the internal carotid artery (ICA) especially at sites of fixation – in the carotid canal at the base of the petrous bone, and at its exit from the cavernous sinus beneath the anterior clinoidprocess.
Conventional angiograms is the gold standard for confirmation and delineation of the vascular injuries.
MRA, CTA serve as important screening tools.
CCF:Results from full-thickness arterial injury.Leads to communication between the
cavernous portion of ICA and the surrounding venous plexus.
Resulting in venous engorgement of the cavernous sinus and its draining branches: the ipsilateral superior ophthalmic vein and inferior petrosal sinus.


Diffuse cerebral swelling Brain herniation Traumatic ischemia , infarction Diffuse hypoxic injury Secondary “delayed’’ hemorrhage Secondary brain stem injury or haemorrhage Others --e.g. fatty embolism , infection
DIFFUSE CEREBRAL SWELLING Due to an increase in cerebral blood volume
(hyperemia), vasogenic edema, or increase in tissue fluid (cerebral or cytotoxic edema).
CT – effacement of the cerebral sulci and cisterns and compression of the ventricles.
In cerebral edema, the gray–white matter differentiation is lost.
In cerebral hyperemia, the gray–white matter differentiation is preserved.


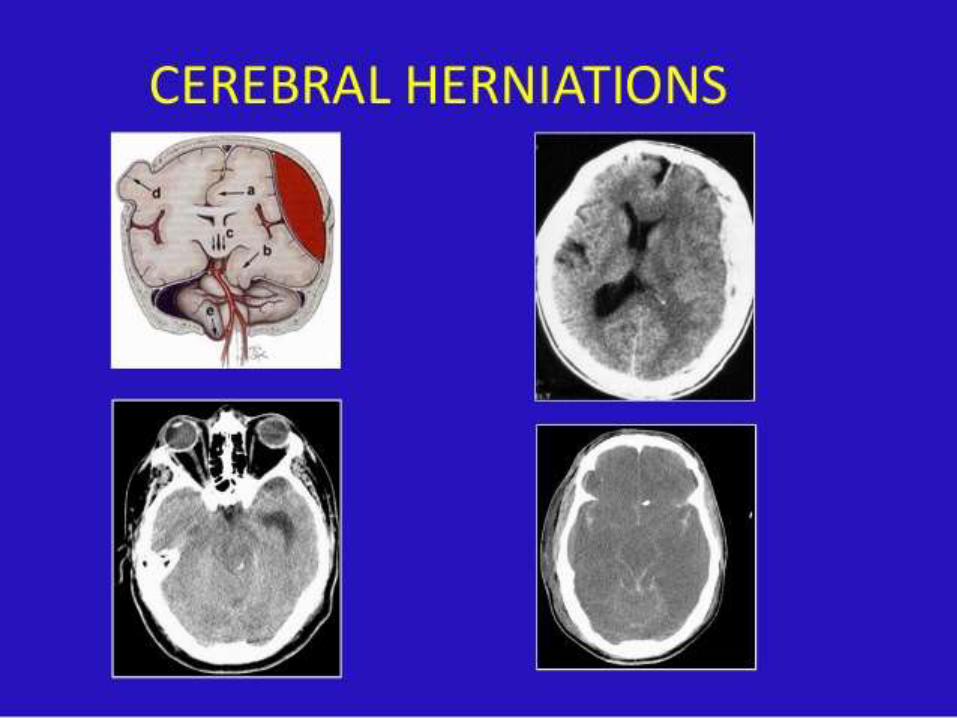
BRAIN HERNIATION Occurs secondary to mass effect produced by
other causes. Subfalcine herniation: most common form, the
cingulate gyrus displaced across midline under the falx cerebri.
Uncal herniation: the medial temporal lobe is displaced over the free margin of tentorium. Important clue - effacement of ambient and lateral suprasellar cisterns.

Transtentorial herniation – downward or upward herniation in cerebellum/cerebrum.
Translar ( trans sphenoidal ) herniation –downward or upward herniation.
Tonsilar herniation. Miscellaneous - trans dural / trans cranial
herniation.
ISCHAEMIA OR INFARCTION Occurs as a result of increased intracranial
pressure or mass effect on cerebral vasculature by herniation or hematoma.
ACA infarction – secondary to subfalcineherniation which displaces the ACA to the contralateral side, trapping the callosomarginal branches of the ACA.

Uncal herniation can cause ischaemia in the posterior cerebral artery territory.
Tonsillar herniation can cause ischemia in the posterior inferior cerebellar artery territory.

Encephalomalacia and atrophy. Pneumocephalus, pneumatocele formation. CSF leaks and fistula. Acquired encephalocoele or leptomeningeal
cyst. Cranial nerve injuries. Diabetes incipidus. Hydrocephalus. Subdural hygroma. Post traumatic abscess.

The goal of imaging in the management of head trauma is to identify treatable injuries to prevent secondary damage.
CT continues to be the modality of choice in the evaluation of acute head injury.
CT is preferred in the acute setting because it is accurate, fast, widely available and can easily accommodate life-support and monitoring equipment.
MRI is indicated for patients with acute TBI when the neurologic findings are unexplained by CT.
MRI is also the modality of choice for subacute or chronic injury.