Embed Size (px)
Citation preview

Radiological Signs in Chest Medicine
Gamal Rabie Agmy MD FCCP Professor of chest Diseases Assiut university
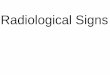
S Curve of
Golden
When there is a mass
adjacent to a fissure the
fissure takes the shape
of an S The proximal
convexity is due to a
mass and the distal
concavity is due to
atelectasis Note the
shape of the transverse
fissure
This example represents
a RUL mass with
atelectasis
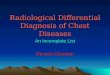
Pulmonary Artery
Overlay Sign
This is the same concept
as a silhouette sign If
you can recognize the
interlobar pulmonary
artery it means that the
mass seen is either in
front of or behind it
This is an example of a
dissecting aneurysm
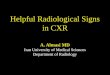
Achalasia of esophagus
Inhomogeneous cardiac density
Right half more dense than left
Density crossing midline (right black
arrow)
Right sided inlet to outlet shadow
Right para spinal line (left black
arrow)
Barium swallow below Dilated
esophagus
Feeding vessel sign
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

S Curve of
Golden
When there is a mass
adjacent to a fissure the
fissure takes the shape
of an S The proximal
convexity is due to a
mass and the distal
concavity is due to
atelectasis Note the
shape of the transverse
fissure
This example represents
a RUL mass with
atelectasis
Pulmonary Artery
Overlay Sign
This is the same concept
as a silhouette sign If
you can recognize the
interlobar pulmonary
artery it means that the
mass seen is either in
front of or behind it
This is an example of a
dissecting aneurysm
Achalasia of esophagus
Inhomogeneous cardiac density
Right half more dense than left
Density crossing midline (right black
arrow)
Right sided inlet to outlet shadow
Right para spinal line (left black
arrow)
Barium swallow below Dilated
esophagus
Feeding vessel sign
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Pulmonary Artery
Overlay Sign
This is the same concept
as a silhouette sign If
you can recognize the
interlobar pulmonary
artery it means that the
mass seen is either in
front of or behind it
This is an example of a
dissecting aneurysm
Achalasia of esophagus
Inhomogeneous cardiac density
Right half more dense than left
Density crossing midline (right black
arrow)
Right sided inlet to outlet shadow
Right para spinal line (left black
arrow)
Barium swallow below Dilated
esophagus
Feeding vessel sign
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Achalasia of esophagus
Inhomogeneous cardiac density
Right half more dense than left
Density crossing midline (right black
arrow)
Right sided inlet to outlet shadow
Right para spinal line (left black
arrow)
Barium swallow below Dilated
esophagus
Feeding vessel sign
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Feeding vessel sign
Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Radiographic Signs of Pneumomediastinum
Subcutaneous emphysema
Thymic sail sign
Pneumoprecardium
Ring around the artery sign
Tubular artery sign
Double bronchial wall sign
Continuous diaphragm sign
Extrapleural sign
Air in the pulmonary ligament
Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Incomplete Border Sign
(Pregnant Lady Sign) The incomplete border sign is
useful to depict an
extrapulmonary mass on
chest radiograph
An extrapulmonary mass will
often have a inner well defined
border and an ill-defined outer
margin This can be attributed
to the inner margin being
tangential to the x-ray beam
and has good inherent
contrast with the
adjacent lung On the other
hand the outer margin is
enface or partially enface with
the x-ray beam and merges
with the pleural or chest wall
thus the border is obscured
Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Ginkgo leaf sign bull The ginkgo leaf sign is a chest plain radiography
appearance which is seen at extensive subcutaneous
emphysema of the chest wall Air outlines the fibers of
the pectoralis major muscle and creates a branching
pattern that resembles the branching pattern in the
veins of a ginkgo leaf
Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Juxtaphrenic peak sign
The juxtaphrenic peak sign refers to the peaked or
tented appearance of a hemidiaphragm which can
occur in the setting of lobar collapse It is caused by
retraction of the lower end of diaphragm at an inferior
accessory fissure (most common) major fissure
or inferior pulmonary ligament It is commonly seen
in upper lobe collapse but may also be seen in middle
lobe collapse
CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

CT angiogram Sign
Identification of vessels within an
airless portion of lung on contrast-
enhanced CT
The vessels are prominently seen
against a background of low-
attenuation material
Associated with
bronchoalveolar cell carcinoma
lymphoma
infectious pneumonias
Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Fallen Lung Sign
This sign refers to the appearance
of the collapsed lung occurring
with a fractured bronchus
The bronchial fracture results in
the lung to fall away from the
hilum either inferiorly and laterally
in an upright patient or posteriorly
as seen on CT in a supine patient
DD
Pneumothorax causes a lung to
collapse inward toward the hilum
Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Luftsichel Sign
bullGerman for sickle of air (luft air sichel
crescent)
bullParamediastinal lucency due to
interposition of lower lobe apex between
mediastinum and shrunken upper lobe
bullOccurs more commonly on the left than in
the right
Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Halo Sign
CT shows nodular consolidation associated with a halo of ground-glass
opacity (GGO) in both apices resulting from invasive pulmonary
aspergillosis
This halo represents hemorrhage
When seen in leukemic patients is highly suggestive of the diagnosis of
invasive pulmonary aspergillosis
CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

CT Halo Sign
Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Reverse Halo Sign
bullCentral ground-glass opacity surrounded
by denser consolidation of crescentic or
ring shape at least 2 mm thick
bullFirst described by Voloudaki in 1996
bullKim in 2003 used the term reverse halo
bullFound to be relatively specific for crypto-
genic organizing pneumonia (COP)
Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Reverse Halo Sign
Seen in other conditions
bullWegenerrsquos granulomatosis
bulllymphomatoid granulomatosis
bullparacoccidiodomycosis
bullneoplastic (metastasis)
bullinvasive aspergillosis
bulllipoid pneumonia
Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Tree-in-Bud Sign
bull
Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Pearl ring sign
Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Steeple sign
The steeple sign (also called wine bottle
sign) refers to tapering of the
upper trachea on a frontal chest
radiograph reminiscent of a church
steeple The appearance is suggestive
of croup which should be obvious
clinically A corresponding lateral x-ray
would show narrowing of the subglottic
trachea and ballooning of the
hypopharyn
Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Cancer Breast
Larger right breast Inverted nipple
Radiation Fibrosis of
Lung
Right lung smaller
Right hemithorax smaller
Paramediastinal fibrosis
Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Primary lobule
A primary pulmonary lobule is defined
as the lung unit distal to the respiratory
bronchioles It is significantly smaller
than an acinus and is composed of
alveolar ducts alveolar sacs and
alveoli
It has been estimated that
each secondary pulmonary lobule is
composed of 30-50 primary lobules
Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Pulmonary Acinus
Pulmonary acinus is commonly defined
as the portion of lung distal to
a terminal bronchiole and supplied by a
first-order respiratory bronchiole or
bronchioles
Each secondary pulmonary
lobule contains 3-12 acini and adjacent
acini are separated by
incomplete intralobular septae
Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Secondary lobule
Basic anatomic unit of pulmonary
structure and function
1-2 cm and is made up of 5-15
pulmonary acini
Supplied by a small bronchiole
(terminal bronchiole) in the
center that is parallelled by the
centrilobular artery
Pulmonary veins and lymphatics
run in the periphery
Two lymphatic systems
central network
peripheral network
The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

The terminal bronchiole in the center divides into respiratory bronchiolies with acini that contain alveoli Lymphatics and veins run within the interlobular septa
Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular area in blue perilymphatic area in yellow
Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Raoof S CHEST 2006 129805
Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Perilymphatic distribution
Centrilobular distribution
Random distribution
Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Random distribution distribution pattern of
pulmonary nodules where
there pattern of involvement
with respect to the lung lacks
a an architectural
prdominance These nodules
affect the fissures
peribronchovascular
structures and the center of
the secondary pulmonary
nodules They can range from
a number of pathologies
They can have variable
density and may or may not
be uniformly distributed
Some may have
haematogenous origin
Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular distribution Centrilobular lung
nodules refer to an HRCT
chest imaging descriptor for
lung nodules which are
anatomically located centrally
within secondary pulmonary
lobules The term is applied on
the basis of position of the
nodule and not its morphology
Centrilobular nodules can
therefore well defined or poorly
defined
Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular distribution
infection with endobronchial
spread
airway spread
of tuberculosis
airway spread of non
tuberculous mycobacterial
infection
airway invasive
aspergillosis
bronchoalveolar
carcinoma with airway spread
subacute hypersensitivity
pneumonitis
bronchiolitides
obliterative bronchiolitis
respiratory bronchiolitis
interstitial lung disease
pulmonary vasculitides
Churg Strauss syndrome
Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Perilymphatic distribution Perilymphatic lung
nodules refer to type of lung
nodules dependent on their
distribution in relation to
anatomical structures of the
lung These nodules follow
perilymphatic channels and
on imaging are typically
subpleural occur along
fissures interlobular septae
and adjacent to the
bronchovascular bundles
Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Perilymphatic distribution Nodules in a perilymphathic
distrubution are classically found
with pulmonary sarcoidosis1 but
can also rarely occur with other
conditions such as
silicosis
coal workers pneumoconiosis 3 -
usually simple coal workers
pneumoconiosis
lymphangitis arcinomatosis tends
to be interspersed with
interlobular septal thickening
nodular pulmonary myloidosis
lymphocytic interstitial
pneumonia
ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

ARE NODULES IN CONTACT WITH PLEURA
NO
CENTRILOBULAR
YES
PERILYMPHATIC RANDOM
Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Hypersensitivity
pneumonitis
HRCT at the level of the
upper lobes reveals an ldquoill-
defined centrilobular nodular
patternrdquo characterised by
micronodules of ground-
glass opacity that are
diffusely distributed
characteristically in the
centre of the pulmonary
lobules
RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

RBILD
HRCT at the level of the upper
lobes exhibits an ldquoill-defined
centrilobular nodular patternrdquo
characterised by micronodules of
ground-glass opacity that are
diffusely distributed
characteristically in the centre of
the pulmonary lobules In this case
the history of smoking favours the
diagnosis of respiratory
bronchiolitis interstitial lung disease
Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Miliary TB HRCT at the level of the upper
lobes exhibits a ldquomiliary nodular
patternrdquo characterised by random
micronodules diffusely and
symmetrically distributed within the
lungs having approximately the
same size
Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Miliary metastatic disease
HRCT at the level of the upper lobes
shows a ldquomilary nodular patternrdquo
characterised by random and
perilymphatic micronodules diffusely
distributed throughout the lungs that
have a more variable size compared
Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Differential diagnosis of a nodular
pattern of interstitial lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial fungal viral)
Metastases Miliary TB
Microlithiasis alveolar
Pneumoconioses (silicosis coal
workers berylliosis)
Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Ground Glass Nodule
Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Ground Glass Nodule A ground glass density nodule is a circumscribed area of
increased pulmonary attenuation with preservation of the
bronchial and vascular margins A GGN can be
partly solid (part of the ground-glass opacity completely obscures
the parenchyma)
nonsolid (no completely obscured areas) - pure ground glass
nodules
Although encountered regularly the incidence of cancer in these
nodules has been reported as high as 63 (for partly solid
nodules in one study) Histologically these may represent
cancer - (eg bronchoalveolar carcinoma (BAC) adenocarcinoma
in situminimally invasive adenocarcinoma and invasive
adenocarcinoma)
atypical adenomatous hyperplasia
focal interstitial fibrosis
aspergillosis
focal pulmonary haemorrhages
A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

A 27-year-old man is referred to you for evaluation of an abnormal chest radiograph About 5 months ago he consulted
a doctor because of excessive thirst Evaluation resulted in the diagnosis of diabetes insipidus which responded favorably to desmopressin administered nasally Recently he started to notice shortness of breath when climbing stairs and a chest radiograph was obtained
bullPatient history reveals significant tobacco smoking up to two packs daily for at least 14 years The patient noticed the shortness of breath for at least 2 years and recently he noted a point of tenderness over the chest wall lateral to the
posterior axillary line on the left bullOxygen saturation is 94 while breathing room air and the rest of his vital signs were normal Auscultation reveals only rare crackles without prolongation of the expiratory phase
There is a point of tenderness over the left sixth and seventh ribs in the posterior axillary line and a chest CT scan is obtained
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

The most likely diagnosis is A Metastatic tumor of unknown primary site B Sarcoidosis C Langerhans cell histiocytosis D Idiopathic pulmonary fibrosis
DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

DECREASED LUNG
ATTENUATION
Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Lung Cysts
Pulmonary fibrosis (Honeycombing)
Lymphangiomyomatosis
Langerhanscell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)
Differential Diagnosis
Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP
Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Usual Interstitial Pneumonia UIP
HRCT Findings
Reticular opacities thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance
Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Basal and subpleural distribution
UIP
Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women
Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Lymphangioleiomyomatosis (LAM)
Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Tuberous Sclerosis (young man)
Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (lt 1cm)
Bizarre and confluent
Ground glass opacities
Late signs irreversible parenchymal fibrosis Honey comb lung septal thickening
bronchiectasis
1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
Langerhans Cell Histiocytosis
Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

after cessation of smoking
Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP
= Lymphocytic Interstitial Pneumonia
Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Sjoumlgren LIP
LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

LIP
= Lymphocytic Interstitial Pneumonia
Rarely idiopathic
In association with Sjoumlgren‟s syndrome
Immune deficiency syndromes AIDS
Primary biliary cirrhosis
Multicentric Castlemean‟s disease
Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Sjoegren disease
Dry eye and dry mouth
Fibrosis bronchitis and bronchiolitis
LIP
Overlap
Sarcoid DMPM MXCT
SLE RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma
Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Young woman Dry mouth Smoker
LAM LIP Histiocytosis
Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Wegenerbdquos disease
Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Rheumatoid Arthritis
Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Emphysema
histopathological definition
hellippermanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
hellipdestruction of the walls of the involved
airspaces
Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular Emphysema
Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Panlobular Emphysema
CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

CLE and PLE in one Patient
Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Fibrosis and Emphysema
LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

LAM Emphysema Fibrosis
LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

LCH Emphysema
Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Fibrosis Emphysema
Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Emphysema
Emphysema typically presents as
areas of low attenuation without
visible walls as a result of
parenchymal destruction
EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

EMPHYSEMA
Permanent abnormal enlargement of air
spaces distal to the terminal bronchiole
and accompanied by the destruction of
the walls of the involved air spaces
110
Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular emphysema
Most common type
Irreversible destruction of alveolar
walls in the centrilobular portion of the
lobule
Upper lobe predominance and
uneven distribution
Strongly associated with smoking
Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular (proximal or
centriacinar) emphysema
Found most commonly in the upper lobes
Manifests as multiple small areas of low attenuation without a
perceptible wall producing a punched-out appearance
Often the centrilobular artery is visible within the
centre of these lucencies
112
Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Centrilobular emphysema due to smoking The periphery of
the lung is spared (blue arrows) Centrilobular artery (yellow
arrows) is seen in the center of the hypodense area
Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Panlobular emphysema
Affects the whole secondary lobule
Lower lobe predominance
In alpha-1-antitrypsin deficiency but
also seen in smokers with advanced
emphysema
PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

PANLOBULAR EMPHYSEMA
Affects the entire secondary pulmonary
lobule and is more pronounced in the lower
zones
Complete destruction of the entire pulmonary
lobule
Results in an overall decrease in lung
attenuation and a reduction in size of
pulmonary vessels
115
PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

PANLOBULAR EMPHYSEMA
116
Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Panlobular emphysema
Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Paraseptal (distal acinar)
emphysema
Affects the peripheral parts of
the secondary pulmonary lobule
Produces subpleural lucencies
118
Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Paraseptal emphysema
Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Cystic lung disease
Lung cysts are defined as radiolucent areas with a
wall thickness of less than 4mm
Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Langerhans cell histiocytosis
Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Lymphangiomyomatosis complicated by pneumothorax
Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Bronchiectasis
Bronchiectasis is defined as localized bronchial
dilatation (signet-ring sign)
bronchial wall thickening
lack of normal tapering with visibility of airways
in the peripheral lung
mucus retention in the broncial lumen
associated atelectasis and sometimes air
trapping
ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

ABPA glove-finger shadow due to mucoid impaction in central
bronchiectasis in a patient with asthma
Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Signet-Ring Sign
A signet-ring sign represents an axial cut of a dilated bronchus
(ring) with its accompanying small artery (signet)
Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Tram Tracks
Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Bronchial dilation with lack of tapering
HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

HONEYCOMBING
Defined as - small cystic spaces with
irregularly thickened walls composed of
fibrous tissue
Predominate in the peripheral and subpleural
lung regions
Subpleural honeycomb cysts typically occur
in several contiguous layers DD- paraseptal
emphysema in which subpleural cysts usually
occur in a single layer
Indicates the presence of ldquoEND stagerdquo
disease regardless of the cause
129
Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Honeycombing
Honeycombing is defined by the presence of small cystic
spaces with irregularly thickened walls composed of
fibrous tissue
Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Causes
Lower lobe predominance
1 UIP or interstitial fibrosis
2 Connective tissue disorders
3 Asbestosis
4 Drug induced
5 NSIP (rare)
Upper lobe predominance
1 End stage sarcodosis
2 Radiation
3 Hypersensitivity Pneumonitis
4Silicosis
4 End stage ARDS
131
Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Honeycombing
HRCT showing
subpleural
broncheolectasis
Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Honeycombing and traction bronchiectasis in UIP
Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Typical UIP with honeycombing and traction
bronchiectasis in a patient with idiopathic
pulmonary fibrosis (IPF)
Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Inconsistent with UIP
pattern (any one of
seven features)
Possible UIP
pattern (all
three features)
UIP pattern (all
four features)
bullUpper or mid lung
predominance
bullperibronchovascular
predominance
bullextensive ground glass abnormality (extent gt
reticular abnormality)
bullprofuse micronodules
(bilateral predominantly
upper lobes) bulldiscrete cysts (multiple
bilateral away from areas of
honeycombing)
bulldiffuse mosaic
attenuationair trapping (bilateral in three or more
lobes)
bullsubpleural basal
predominance
bullreticular abnormality
bullAbsence of features listed as inconsistent
with UIP pattern
bullsubpleural basal
predominance
bullreticular abnormality
bullhoneycombing with
or without traction
bronchiectasis
bullAbsence of features
listed as inconsistent
with UIP pattern
Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Mosiac pattern
Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Where is the pathology
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping
Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Pathology in black areas
Airtrapping Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic connective tissue diseases drug reaction
after transplantation after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma Bronchiectasis Airway diseases
Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Airway Disease
what you seehelliphellip
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration bdquoblack‟ areas remain in volume and density
bdquowhite‟ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING
Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Bronchiolitis
obliterans
Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Early Sarcoidosis
Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Chronic EAA
Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Hypersensitivity pneumonitis
Extr Allerg Alveolitis (EAA) HRCT
Morphology
chronic fibrosis
Intra- interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)
Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Pathology in white Areas
Alveolitis Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES
DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

DI
P
Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Cellular
NSIP
Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic cardiac disease pulmonary
disease
CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

CTEPH =
Chronic thrombembolic
pulmonary hypertension
Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Hydrostatic pulmonary
oedema
ldquoseptal patternrdquo characterised by
thickened smoothly interlobular
septae in the right parahilar area
Right pleural effusion is also seen
Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure

Lymphangitic carcinomatosis
HRCT of the right lung shows a
ldquoseptal patternrdquo characterised by
diffuse nodular thickening of the
interlobular septae and the right
major fissure