Embed Size (px)
DESCRIPTION
Collection of cases I saw during my residency.
Citation preview

Radiology of Tuberculosis
Mohit Goyal
Under the guidance of: Sr. Prof. Dr. V.K. Goyal
Department of Medicine, R.N.T. Medical College, Udaipur
13th February, 2014

Radiology of Tuberculosis
Common Roentgenograms
Summary of Roentgenographic manifestations of TB
An extremely rare case
Some CT and MRI findings in TB

XR01 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
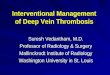
This patient, a 32-year-old male presented with insidious onset,
progressive, productive cough for 3 months; feverish feeling for a
month and loosening of clothes over time.
Past history: No history of any other illnesses.
Over the counter medications taken on and off over the past month
for cough and fever.
The patient had difficulty producing sputum for the examination.
The sample mainly contained saliva and was found negative for AFB.
The patient was referred to Dept. of TBCD. BAL sample was taken,
subjected to microbiological examination and found positive for AFB.
XR01

Miliary shadows/mottling
Millet seed sized opacities ~ 2mm
Miliary densities are seen in: Miliary TB, Anthracosis, Sarcoidosis,
Tropical eosinophilia, Fibrosing alveolitis, Allergic alveolitis,
Histoplasmosis, Coccidioidomycosis, Blastomycosis, Cryptococcosis.
Pulmonary haemosiderosis and Silicosis are also seen as milliary
mottling but the radiodensity is more than soft tissue.
Carcinomatosis, lymphoma and sarcoidosis have discrete but slightly
larger shadows (> 2mm).
Some pneumonias, fat emboli and pulmonary oedema can present as
shadows > 2mm that tend to coalesce.

Metastasis from Papillary ca Miliary Tuberculosis
XR01

XR02 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
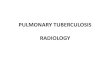
This patient, a 23-year-old male presented with fever, productive
cough and weight loss for one month.
Past history: No history of any other illnesses.
Over the counter medications taken over the past month for fever.
The patient’s sputum was sent for examination and found to be
positive for acid fast bacilli.
XR02

Cavity
A gas containing space in the lungs surrounded by a wall whose
thickness is >1mm.
In bullae, the wall thickness is <1mm.
Thin walled cavities may be seen in tuberculous cavity, infected
bullae, staphylococcus, Klebsiella, post-traumatic cysts,
Coccidioidomycosis, Mycobacterium kansasii infection, metastatic
cavitating squamous cell ca of cervix.
Thick walled cavities may be seen in lung abscess, metastatic
carcinoma, bronchogenic carcinoma, Wegener’s granulomatosis,
fungal cavity, necrotising squamous cell carcinoma, Blastomycosis.
XR02

Cavity
The cavity wall is irregular or nodular in carcinoma, rugged or
shaggy in acute lung abscess and smooth in other cavitating lesions.
Cavity with wall thickness <5mm is likely to be benign; 5-15mm may
be benign or malignant and >15mm is likely to be malignant.
Lung abscess - superior segment of the lower lobe and axillary sub
segments of anterior and posterior segment of the upper lobe.
Tubercular – superior segments of upper and lower lobes.
Klebsiella, SCC – upper lobes.
Cystic bronchiectasis, hydatid cyst – lower lobes
Note: when a cavity in the anterior segment is encountered, strong
suspicion for lung cancer should be raised.

XR03 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
This patient, a 70-year-old male presented with insidious onset,
progressive shortness of breath. No history of cough, expectoration.
Past history: Taken ATT 10 years back for pulmonary TB.
The patient’s sputum was sent for examination and was found to be
negative for acid fast bacilli. CT imaging of thorax was planned but
the patient refused.
XR03

XR04 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
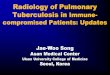
This patient, a 60-year-old male presented with difficulty breathing,
pain on the right side of chest and dry cough on and off.
Past history: Taken ATT 8 years back for pulmonary TB with possibly
pleural effusion. Documents not available but the patient describes
both parenchymal disease as well as pleural effusion.
The patient’s sputum was sent for examination and was found to be
negative for acid fast bacilli. CT imaging of thorax revealed pleural
thickening and calcification. There was not evidence of activity.
XR04

XR05 Ra
dio
log
y o
f Tu
be
rcu
losi
s

XR05 Ra
dio
log
y o
f Tu
be
rcu
losi
s

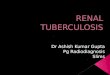
Presentation
This patient, a 20-year-old male presented with insidious onset,
progressive shortness of breath for 2 months.
Past history: No history of any chronic illnesses.
Pleural fluid was sent for analysis. It was found to have 800 cells,
with 90% lymphocytes. Proteins were 6 g% and the fluid was positive
for ADA. Patient’s ESR was 63.
The patient’s sputum was sent for examination and was found to be
negative for acid fast bacilli.
XR05

XR06 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
This patient, a 57-year-old male presented with acute onset
shortness of breath.
Past history: Two years back he took ATT for 6 months.
Emergency management was done. The patient’s sputum was sent
for examination and was found to be negative for acid fast bacilli.
XR06

XR07 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
This patient, a 40-year-old male presented with insidious onset,
progressive edema and shortness of breath.
Past history: He was diagnosed to have pericardial effusion an year
back, which was found to be tubercular, and he was given ATT for it.
The patient’s sputum was sent for examination and was found to be
negative for acid fast bacilli.
ECHO revealed pericardial calcification, constrictive pericarditis. The
patient was taken over by the Dept. of Cardio-Thoracic-Vascular
surgery for further management.
XR07

XR08 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Radiology of Tuberculosis
Common Roentgenograms
Summary of Roentgenographic manifestations of TB
An extremely rare case
Some CT and MRI findings in TB

Consolidation in primary infection
This may involve any part of the lung, and the appearance is non-
specific unless there is coincidental lymphadenopathy.
The area involved may be small or affect an entire lobe, and an air
bronchogram may be visible. Occasionally consolidation appears as a
well-defined nodule or nodules.
Healing is often complete without any sequelae on the chest
radiograph although fibrosis and calcification may occur.
Tuberculous bronchopneumonia may occur in both primary and
post-primary infection, causing patchy, often nodular, areas of
consolidation.

Consolidation in post-primary infection
This usually appears in the apex of an upper or lower lobe, and
almost never in the anterior segments of the upper lobes.
The consolidation is often patchy and nodular and may be bilateral.
A minimal apical lesion can easily be overlooked because of
overlapping shadows of ribs and clavicle. Comparison with the
opposite side is then helpful, looking for asymmetries of density. The
apical projection was designed to overcome this difficulty, but is
rarely useful.
Progressive infection is indicated by extension and coalescence of the
areas of consolidation, and the development of cavities.

Consolidation in post-primary infection
Simultaneously there may be fibrosis and volume loss indicating
healing.
Cavities may be single or multiple, large or small and thin or thick
walled. Fluid levels are sometimes visible within cavities.
With fibrosis there is often obliteration of cavities; however, larger
cavities may persist and areas of bronchiectasis and emphysema
may develop. Healed lesions often calcify.
Because the upper lobes are predominantly involved, the effects of
fibrotic contraction are seen as the trachea being pulled away from
the midline, elevation of the hila and distortion of the lung
parenchyma.

XR02 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Miliary tuberculosis
This is due to haematogenous spread of infection and may be seen in
both primary and post-primary disease. In the former the patient is
often a child, and in the latter case the patients are often elderly,
debilitated or immunocompromised.
At first the chest radiograph may be normal, but then small, discrete
nodules, 1-2 mm in diameter, become apparent, evenly distributed
throughout both lungs.
These may enlarge and coalesce, but with adequate treatment they
slowly resolve. Occasionally, some may calcify.

XR01 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Tuberculoma
This is a localized granuloma due to either primary or post-primary
infection. It usually presents as a solitary well-defined nodule, up to
5 cm in diameter. Calcification is common but cavitation is unusual.
Lymphadenopathy
Hilar and mediastinal lymphadenopathy is a common feature of
primary infection and may be seen in the presence or absence of
peripheral consolidation. Following healing, involved nodes may
calcify. Lymphadenopathy is usually unilateral but may be bilateral
where the differential diagnoses of lymphoma and sarcoidosis come
in. It is often more pronounced in children.

Pleural changes
Pleural effusion complicating primary infection is usually unilateral
and due to subpleural infection. Pulmonary consolidation and/or
lymphadenopathy may or may not be apparent.
At presentation the effusion may be large and relatively
asymptomatic. These effusions usually resolve without complication.
Pleural effusion in post-primary infection, however, often progresses
to empyema. Healing is then complicated by pleural thickening and
often calcification. Uncommon complications of tuberculous
empyema are bronchopleural fistula , osteitis of a rib,
pleurocutaneous fistula and secondary infection. Previous
thoracoplasty may also complicate the appearances.

XR05 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Pleural changes
Pleural thickening over the apex of the lung often accompanies the
fibrosis of healing apical tuberculosis. Pneumothorax may complicate
subpleural cavitatory disease.
Airway Involvement
This may be secondary to lymphadenopathy or endobronchial
infection and may therefore complicate both primary and post-
primary disease. Compression of central airways by enlarged nodes
may cause pulmonary collapse or air trapping. Healing of
endobronchial infection with fibrosis may result in bronchostenosis.
The lung distal to bronchial narrowing may develop bronchiectasis.

XR04 Ra
dio
log
y o
f Tu
be
rcu
losi
s

Radiology of Tuberculosis
Common Roentgenograms
Summary of Roentgenographic manifestations of TB
An extremely rare case
Some CT and MRI findings in TB

Rare Case Ra
dio
log
y o
f Tu
be
rcu
losi
s

Presentation
This patient, a 48-year-old male presented with insidious onset,
progressive dysphagia for 5 months.
Past history: ATT taken 1 year back for pulmonary TB.
Endoscopic biopsy and CT thorax and abdomen were planned.
Biopsy examination revealed casseating epitheloid granuloma and
positive acid fast staining.
The oesophagus was dilated and the patient has been put on ATT.
Rare Case


Rare Case Ra
dio
log
y o
f Tu
be
rcu
losi
s

Radiology of Tuberculosis
Common Roentgenograms
Summary of Roentgenographic manifestations of TB
An extremely rare case
Some CT and MRI findings in TB

XR08 Ra
dio
log
y o
f Tu
be
rcu
losi
s

CT08

CT08

CT08

CT09

Presentation
This patient presented with fever for one month, altered behavior for
3 days and loss of consciousness for 6 hours.
Past history: No history of any chronic illnesses.
CSF examination revealed 100 cells, mainly lymphocytes. Proteins
were 6.4 g% and the fluid was positive for Adenosine deaminase.
CT09

CT09

Neuroimaging findings in TB
Hydrocephalus – seen in 50-80% cases
Enhancement of basal meninges – 60%
Cerebral infarctions – 28%
Tuberculomas – 10%
Mass effects due to tuberculomas and abscess
Vasculitis
Thrombosis

MR10

MR10

MR10

MR10

THANK YOUfor the patience
Department of Medicine, R.N.T. Medical College, Udaipur
Acknowledgements:
Dept. of Radiodiagnosis, R.N.T. Medical College
Dr. Rambir Singh, MRI Centre, M.B. Govt. Hospital
Dr. Vinita Goyal, M.D. Radiodiagnosis
Sources:
Harrison’s Principles of Internal Medicine
Textbook of Radiology and Imaging, David Sutton
Tuberculosis, Surendra K. Sharma