Embed Size (px)
Citation preview

Relationship between Whole-Grain Intake, Chronic Disease Risk Indicators, and Weight Status among AdolescentsLaura Simonitch
B.S. University of Nebraska-Lincoln
Dietetic Intern, MS Student
University of Kansas Medical Center

Introduction• Whole grains: dietary fiber, phytoestrogens,
minerals, antioxidants, vitamin E, folate1, 2
• Past studies contradictory3
• Little data for adolescents
• Inverse association between whole-grain intake and BMI4
• Failed to account for other dietary factors1,5,6

Introduction
• Increased prevalence of obesity– Type 2 diabetes, CVD risk factors7,8,9
• Future public health efforts about whole grain intakes for adolescents
7. Ogden et al (2010) 8. Tybor et al (2011) 9. Freedman eta l (1999)

Research Question
What is the relationship among chronic disease risk factors, weight status, and whole-grain intake among adolescents ages 12-19 years by sex?
Reicks et al. Relationship between whole-grain intake, chronic disease risk indicators, and weight status among adolescents in the National Health and Nutrition Examination Survey, 1999-2004. Journal of the Academy of Nutrition and Dietetics. 2012;112:46-55.

Study Methods
• Cross-sectional data from the National Health and Nutrition Examination Survey from years 1999-2004 (NHANES)
• Stratified, multistage probability sample of the non-institutionalized US population
• NHANES surveys from 1999-2000, 2001-2002, and 2003-2004 combined

Participants
• Age 12 to 19 years old
• Boys and girls of various ethnicities and anthropometrics
6,418 adolescents screened
2,495 boys 2,433 girls
4,928 adolescents
included

Exclusion Criteria
• Extreme energy intakes
• Currently breastfeeding or pregnant
• Taking insulin, oral medication for diabetes, or medication for hypertension
• Missing data for disease risk factors, C-reactive protein, systolic blood pressure, total cholesterol, HDL cholesterol, serum folate, or homocysteine

Data Collection
• Dietary Intake:
– NHANES 1999-2000 and 2001-2002 data
sets based on a single 24-hour dietary recall
– NHANES 2003-2004 data based on 2 days of
dietary recall

Data Collection
• Anthropometrics– Height– Weight – Waist, arm, and thigh circumferences– Subscapular skinfold thickness– BMI and BMI z scores

Data Collection
• Chronic disease risk factors/laboratory measures– Blood and urine samples– complete blood count and pregnancy analyses
– standard clinical assays
– Friedewald formula
– Fluorescence polarization immunoassay– Mercury sphygmomanometer– CDC used standard assay procedures

Data Collection
• Whole grain intake– MyPyramid Equivalents Database for USDA
Survey food codes show food group information:
• total grain
• whole-grain• non-whole grain• total vegetables, fruits, milk, and meat and beans

Results
• Dietary Intake– 52% boys and 50% girls did not consume
whole grains on days that intake was measured
– Fiber intake below recommendations for boys and girls
– Positive association between whole-grain intake and daily energy intake for boys and girls

Dietary Intake
Significance level: P < 0.05

Results
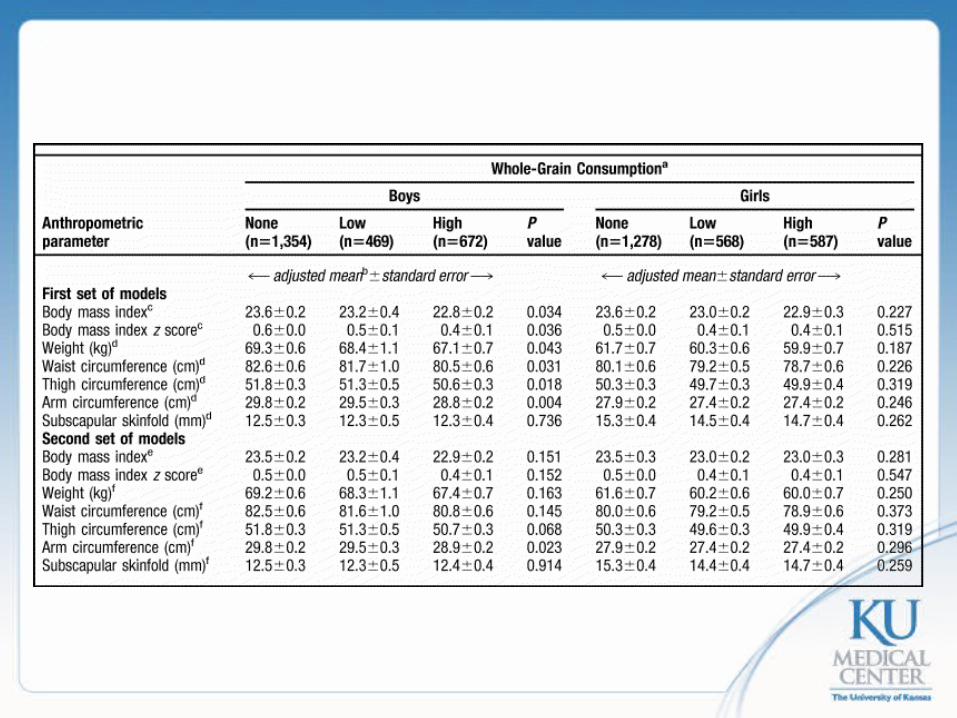
• Anthropometric Measures– Whole-grain intake inversely related among
boys with BMI, BMI z score, weight, and waist, thigh, and arm circumferences
– Only a significant inverse association between whole-grain intake and arm circumference in boys once adjusted for food group intake in the second set of models

Anthropometric Parameter

Results• Chronic disease risk factors/laboratory
measures– Fasting insulin levels inversely related to
whole-grain intake for boys– C-peptide inversely related to whole-grain
intake for girls– Positive association between whole-grain
intake and HDL levels for girls – Boys had an inverse association between
homocysteine levels and whole-grain
intake.
• Chronic disease risk factors/laboratory measures– Boys and girls had a positive association
between serum and red blood cell folate levels and whole-grain intake
– Inverse association between whole-grain intake and fasting insulin levels in girls
– C-reactive protein levels were higher for girls who had low whole-grain intake compared to those with no or high intake
Results

Chronic disease risk factors/laboratory measures
Boys Girls None Low High P value None Low High P value
1st set of models
Homocysteine (µmol/L)
6.8 ± 0.1 6.7 ± 0.2 6.3 ± 0.1 0.002 5.8 ± 0.1 5.9 ± 0.1 5.8 ± 0.2 0.844
Folate, serum (ng/mL)
12.5 ± 0.2 12.4 ± 0.3 14.3 ± 0.3 < 0.001 12.6 ± 0.3 13.6 ± 0.5 14.8 ± 0.5 < 0.001
Folate, red blood cell (ng/mL)
236 ± 3 248 ± 4 259 ± 6 < 0.001 247 ± 5 244 ± 6 269 ± 6 < 0.001
2nd set of models
Folate, serum (ng/mL)
12.6 ± 0.2 12.5 ± 0.2 14.1 ± 0.3 < 0.001 12.7 ±0.2 13.7 ± 0.5 14.5 ± 0.4 < 0.001
Folate, red blood cell (ng/mL)
237 ± 3 249 ± 4 256 ± 5 < 0.001 248 ± 5 244 ± 6 266 ± 5 < 0.001

Discussion/Implications
• Whole-grain intake was not found to be associated with BMI in the second set of models (adjusted for food group intake)
• Positive results between whole-grain intake, nutrient intake, and chronic disease risk indicators for protection against chronic disease in the second set of models
• Sex differences may be due to differences in body composition, weight-gain patterns, hormone involvement in growth
• Inconsistent results from very low overall whole-grain intake
• Overall, this study supports current recommendations that promote high whole grain intake for adolescents
Discussion/Implications
Study Limitations
• Missing data in non-fasting blood samples
• Self-reported 24-hour and 2-day dietary
recalls
• High category scoring misconception

Thank you!
Questions?
Laura Simonitch
B.S. University of Nebraska-Lincoln
Dietetic Intern, MS Student
University of Kansas Medical Center