Embed Size (px)
Citation preview

Approach to Renal Diseases

Outline
•Types of renal syndromes
•Causes
•Diagnostic approach to each syndrome
•Approach to renal allograft

Types of renal syndromes
Hematuria
Proteinuria
Nephrotic syndrome
Nephritic syndrome
Acute renal failure
Chronic renal failure
Urinary tract infections
Nephrolithiasis

HEMATURIA
• Red or brown urine
• Substances other than RBCs can also produce red or
brown urine.
• Urine test strip or dipstick (dark green)
color change in a chromogen (to blue)
hemoglobin peroxidase-like activityfree
In RBCs
microscopic examination of the urine

Causes of Red or Brown Urine Endogenous Substances Foods Drugs
Red blood cells Hemoglobin Myoglobin Bilirubin Porphyrins Melanin
Artificial food coloring Beets Blackberries Blueberries Fava beans Paprika Rhubarb
Adriamycin Chloroquine Deferoxamine Levodopa Methyldopa Metronidazole Nitrofurantoin PhenazopyridinePhenolphthalein Phenytoin Prochlorperazine Quinine Rifampin Sulfonamides

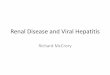
Differentiation of Glomerular from Urologic Bleeding Feature Glomerular Hematuria Urothelial
Hematuria
Urine color Dark red, brown, cola-colored, smoky
Bright red
Clots - +Proteinuria + -Red blood cell morphology
Dysmorphic (especially acanthocytes)
Isomorphic
Hypertension + -Edema + -Urinary voiding symptoms
- +
Back pain, flank pain + +Renal function Reduced normalFamily history + +Trauma - +Upper RTI + -
Fever, rash + -

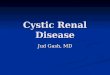
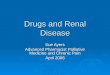
RBC castsC
o
m
p
r
e
s
s
i
o
n
o
f
t
h
e
R
B
C
s
t
o
g
e
t
h
e
r
w
i
t
h
u
r
i
n
e
p
r
o
t
e
i
n
s
Dysmorphic RBCsv
a
r
y
i
n
g
s
h
a
p
e
a
n
d
s
i
z
e
s
w
i
t
h
b
l
e
b
s
,
b
u
d
d
i
n
g
AcanthocytesM
i
c
k
e
y
M
o
u
s
e
e
a
r
s
S
p
e
c
i
f
i
c
w
h
e
n
>
5
%
Co-existing significant proteinuria (
>
0
.
5
g
/
d
o
r
>
0
.
5
g
/
g
o
f
C
r
)
Hematuria



Causes of hematuriaGlomerular Lesions
Thin basement membrane nephropathyIgA glomerulonephritis
FSGSLupus glomerulonephritis
Crescentic glomerulonephritis Membranous glomerulonephritis
Mesangiocapillary glomerulonephritisDense deposit disease
PSGN
Nonglomerular HematuriaUrinary tract infectionUrinary tract calculi
Hypercalciuria and hyperuricosuriaAutosomal dominant polycystic kidney
diseaseBenign prostatic hypertrophyTransitional cell carcinoma
Nonglomerular HematuriaRenal cell carcinomaProstatic carcinomaExercise hematuria
TraumaBleeding diathesis and anticoagulants
Renal papillary necrosisSickle cell diseas

PROTEINURIA
• The dipstick is based on color change induced by the
presence of proteins at a given pH.
• Albumin> other proteins (light chains of Bence Jones
protein)
• 1+ protein ~ 30 mg/dL of proteinuria
• 3+ protein ~ 500 mg/dL of proteinuria.

Types of proteinuria
tubular
overflow
glomerular
Loss of charge and size selectivity>1gm/day
Mostly LMW proteins
Small or +vely charged proteins(Myeloma)

PROTEINURIA
• Microalbuminuria : excretion of abnormal quantities of
albumin below the level detectable by the urine dipstick.
• Radioimmunoassay or enzyme immunoassay.
• Earliest clinically detectable stage of diabetic
nephropathy
• Normal albumin excretion <30 mg/day



NEPHROTIC SYNDROME
1) High-grade, albumin-dominant proteinuria (generally
>3000 mg/day or spot urine protein/creatinine ratio of
>3000 mg of protein/gm of creatinine)
2) Hypoalbuminemia
3) Edema
4) Hyperlipidemia
5) Lipiduria

Diagnostic Evaluation in Adults with Nephrotic Syndrome• Patient history : medication or toxin exposure; risk factors for HIV or viral
hepatitis
• H/O diabetes, systemic lupus erythematosus, or other systemic illness
• Urine dipstick : Confirm proteinuria
• Random urine protein/creatinine ratio
• Quantify degree of proteinuria (ratio greater than 3 to 3.5)
• Serum creatinine
• Rule out acute renal failure, assess glomerular filtration rate
• Serum albumin : hypoalbuminemia
• Lipid panel : hyperlipidemia
• Serum or urine protein electrophoresis : amyloidosis or multiple myelomaNephrotic Syndrome in Adults: Diagnosis and ManagementAm Fam Physician. 2009 Nov 15;80(10):1129-1134

Approach to nephrotic syndrome in children

Diagnostic studies for nephrotic syndrome in children
• Establish whether nephrotic syndrome is present, because hypoalbuminemia
can occur in the absence of proteinuria and edema can occur in the absence
of hypoalbuminemia
• Laboratory tests should confirm (1) nephrotic-range proteinuria (2)
hypoalbuminemia, and (3) hyperlipidemia.
• Urinalysis
• Urine protein quantification (by first-morning urine protein/creatinine or 24-
hour urine protein)
• Serum albumin
• Lipid panel

Diagnostic studies for nephrotic syndrome in children
• First morning urine protein/creatinine is more easily
obtained than 24-hour urine studies (more reliable) and
excludes orthostatic proteinuria.
• Nephrotic-range proteinuria :
Urine protein/creatinine ratio > 2-3 mg/mg
24-hour urine protein level > 40 mg/m2/h
>1000 mg/m2/d

Diagnostic studies for nephrotic syndrome
• Lipid panel findings are typically as follows:
• Elevated total cholesterol, LDL cholesterol
• Elevated triglycerides with severe hypoalbuminemia
• HDL cholesterol (normal or low)

Diagnostic studies for nephrotic syndrome in children• Other tests and procedures in selected patients may include the following:
• < 1 year of age should be evaluated for congenital/infantile nephrotic
syndrome.
• Congenital infection (syphilis, rubella, toxoplasmosis, CMV, HIV)
• NPHS1, NPHS2, WT1, and PLCE1 as guided by biopsy findings and clinical
presentation
• Kidney ultrasonography
• Chest radiography
• Mantoux test
• Kidney biopsy

Diagnostic studies for nephrotic syndrome in children• The patient with INS can present with acute kidney failure due to
intravascular volume depletion and/or bilateral renal vein thrombosis.
• In the absence of the above, elevated BUN and creatinine levels and
signs of chronic kidney failure suggest a chronic glomerular disease
other than MCNS, such as:
• Focal segmental glomerulosclerosis (FSGS)
• Membranous nephropathy (MN)
• MPGN
• IgA nephropathy

Indications of kidney biopsy
1) Age younger than 1 year or older than 8 years
2) Presence of recurrent gross hematuria
3) Relevant family history of kidney disease
4) Symptoms of systemic disease
5) Positive viral screens

NEPHRITIC SYNDROME
• Glomerular hematuria; active urine sediment
• Dysmorphic RBCs (especially acanthocytes) and RBC
casts; often WBCs and WBC casts
• Result of an inflammatory process in the glomerulus
• GFR reduced
• Variable degrees of hypertension, oliguria, and edema

NEPHRITIC SYNDROME
• Proteinuria -low magnitude
• In many cases, the degree of proteinuria is limited by the
accompanying reduction in GFR.
• High-grade proteinuria and even full-blown nephrotic
syndrome can coexist with nephritic syndrome in some
patients.
• Hematuria can be sporadic, intermittent, or persistent.
• It can be microscopic or gross

NEPHRITIC SYNDROME
• The character of the glomerular hematuria does not
always predict the underlying cause of the disorder, nor
does it predict the long-term renal outcome of the
process.
• Glomerular hematuria due to nephritic syndrome must
be distinguished from bleeding caused by other kidney,
interstitial, or lower GU tract pathology.

NEPHRITIC SYNDROMES
Synpharyngitic hematuria IgA nephropathy
Fever, skin rash, joint symptoms Systemic disease causing glomerular hematuria
Hearing loss and visual symptoms related to lens
Alport’s disease
Hemoptysis Vasculitis or anti–glomerular basement membrane disease


Serologies
Antinuclear antibody (ANA) lupus nephritis Lower titres (1:80 or 1:40 are non-specific)
Rheumatoid factor titer rheumatoid arthritis, cryoglobulinemia (type II, III)
Complement components C3 and C4Serum immunoelectrophoresis IgA nephropathy, HSP
Myeloma kidney, lymphomas, amyloidosis, LCDD, HCDD, immunotactoid glomerulonephritis, cryoglobulinemia
Urine electrophoresis, serum free light chains, kappa-lambda ratio
Complement serum electrophoresis
ANCA Rapidly progressive GN

Serologies
Anti-GBM antibodies (IF, western blot)
Anti-GBM disease
Cryoglobulins I: waldenstrom macroglobulinemia, myelomaII: Hepatitis C, SLE, Sjogren syndrome, lymphoma
Hepatitis B Membranous nephropathy
Hepatitis C MPGN, Membranous nephropathy, cryoglobulinemia
HIV Nephrotic syndrome, acute kidney injury
Anti-DNAse/Antistreptolysin titre PIGN
ESR Systemic vasculitis, multiple myeloma, malignancy, nephrotic syndrome [DM]

Complement Levels in Acute Nephritic Syndromes
• Low Serum Complement Levels
Systemic Diseases
SLE
Cryoglobulinemia (hepatitis C)
Bacterial endocarditis
Shunt nephritis
Renal Localized Diseases
Acute PSGN (low C3, normal C4)
MPGN
Type I (low C3 and C4)
Type II (dense deposit disease)
(low C3, normal C4)

Complement Levels in Acute Nephritic Syndromes
• Normal Serum Complement Levels
Systemic Diseases
PAN
ANCA–positive granulomatosis
with polyangiitis (Wegener’s)
Hypersensitivity vasculitis
HSP
Renal Localized Diseases
IgA nephropathy
RPGN
Anti–GBM disease
Pauci-immune GN
(kidney-localized)

Acute Renal Failure

MAKING THE DIAGNOSIS
• Characteristic Signs
• Decrease in GFR over a period of hours to days
• Failure to excrete nitrogenous waste products
• Failure to maintain fluid and electrolyte homeostasis

RIFLE Criteria for Acute Kidney Injury (AKI)
Risk Creatinine increase × 1.5 or GFR decrease > 25%
<0.5 mL/kg/hr for >6 hr
Injury Creatinine increase × 2 or GFR decrease > 50%
<0.5 mL/kg/hr for >12 hr
Failure Creatinine increase × 3 or GFR decrease > 75% orCreatinine ≥ 4 mg% (acute increase ≥ 0.5 mg%)
<0.3 mL/kg/hr for >24 hr or Anuria > 12 hr
Loss Persistent AKI = complete loss of renal function >4 wk
End-stage End-stage renal disease > 3 months

Acute Kidney Injury Network (AKIN) Criteria
Stage Creatinine Criteria Urine Output Criteria
1 Increase in serum creatinine ≥ 3 mg/dL (≥26.4 μmol/L) or increase ≥ 150%-200% (1.5-2 fold) above baseline
<0.5 mL/kg/hr for >6 hr
2 Increase in serum creatinine > 200%-300% (>twofold or threefold) above baseline
<0.5 mL/kg/hr for >12 hr
3 Increase in serum creatinine > 300% (>threefold) above baseline or serum
creatinine ≥ 4 mg/dL (≥354 μmol/L) with an acute rise ≥ 0.5mg/dL (≥44 μmol/L)

Prerenal Azotemia
• Intravascular volume depletion: Hemorrhage, renal fluid
loss, gastrointestinal losses, skin loss of sweat, third-
space losses
• Reduced cardiac output: Congestive heart failure,
cardiogenic shock, pericardial effusion with tamponad,
massive pulmonary embolism
• Increased renal vascular resistance: anesthesia,
hepatorenal syndrome, prostaglandin inhibitors, aspirin,
NSAIDs

Prerenal Azotemia
• Vasoconstricting drugs: cyclosporine, tacrolimus,
radiocontrast
• Decreased intraglomerular pressure : angiotensin-
converting enzyme inhibitors, angiotensin II receptor
blockers

Intrarenal or Intrinsic ARF
• Vascular causes :
• Bilateral renal artery:
• Stenosis
• Thrombosis
• Embolism
• Operative arterial cross
clamping
• Bilateral renal vein thrombosis
• Small vessel :
• Atheroembolic disease
• TMA
• Hemolytic uremic
syndrome/thrombotic
thrombocytopenic purpura
• Scleroderma renal crisis
• Malignant hypertension
• HELLP
• Postpartum ARF

Intrarenal or Intrinsic ARF
• Glomerular :E Goodpasture’s syndrome Granular immune complex deposition:E PostinfectiousE Infective endocarditisE Lupus nephritisE Immunoglobulin A (IgA) nephropathyE Henoch-Schönlein purpuraE Membranoproliferative GN No immune deposits:E Wegener’s granulomatosisE Polyarteritis nodosaE Churg Strauss

Postrenal Azotemia
• Bilateral ureteral obstruction or unilateral obstruction in a solitary
kidney:
• Intraureteral: Stones, blood clots, papillary necrosis
• Extraureteral: Bladder, Prostatic cancer, Cervical cancer,
retroperitoneal fibrosis
• Bladder neck obstruction : Prostatic hypertrophy, Prostatic cancer,
Bladder cancer, Autonomic neuropathy, urethral obstruction, Valves,
Strictures

Evaluation of patient
• Thorough history and physical examination
• Urine Sediment
• Rise in blood urea nitrogen, serum creatinine, or both
• Renal hypoperfusion
• Bland urine sediment
• Fractional excretion of sodium 1%
• Return of renal function to normal within 24 to 72 hours of correction
of the hypoperfused state

Urine biochemical parameters in ARF

Evaluation of patient
• Radiology
• Renal ultrasonography
• Computed tomography
• Cystoscopy and retrograde or anterograde pyelography
• Indications of renal Biopsy in ARF :
• 1) ARF of unknown cause
• 2) Suspicion of GN, systemic disease (eg, vasculitis), or AIN
• 3) ATN not recovering after 4 to 6 weeks of dialysis with no more
recurrent insults

Clinical Diagnosis
• Oliguria, 400 mL urine per day
• Serum markers of renal function (future): Cystatin C
• Urine biomarkers of tubular injury (future):
Interleukin 18
Kidney injury molecule 1
• Neutophil gelatinase associated lipocalin

Chronic Renal Failure

Chronic kidney disease
End-stage
renal
disease
Kidney failure
Kidney
damag
e
GFR < 60 mL/min/1.73 m2 for >3 months
abnormalities or markers of kidney damage abnormalities in the composition of blood or urineabnormalities on imaging tests
GFR< 15mL/ min/1.73m2S/S of uremia kidney replacement therapy for t/t of complications of decreased GFR
dialysis or transplantation regardless of the level of GFR


Estimation of Kidney Function
• GFR can be measured directly using parenteral inulin,
iohexol, or iothalamate
• In clinical practice, GFR is estimated by creatinine clearance
(Ccr), which is directly proportional to creatinine generation
from muscle and inversely proportional to serum creatinine
concentration
• GFR is dependent on age, body mass, nutritional status,
and laboratory measurement of creatinine

Estimation of Kidney Function
• Methods for Estimation of GFR:
• 24-hour urine for Ccr
• Patient instructed about collection of urine for 24 hours

Estimation of GFR
v

Estimation of Kidney Function
• Urea clearance: Ccr exceeds the GFR because of tubular secretion
whereas urea clearance is usually lower than GFR because of
tubular absorption
• Cystatin C: LMW protein produced by all human nucleated cells
• A serum marker of kidney insufficiency, may improve detection of
early CKD
Superior estimation of GFR by cystatin C in children, transplant
patients and cirrhotics
> sensitive for detection of early CKD than serum creatinine

Complications of CKD: bone/mineral,heart, anemia, acidosis, malnutrition
• Elevations of phosphorus occur with decrease in Ccr
around 50 to 60 mL/min
• Determination of vitamin D (including measurement of
25- and 1,25- vitamin D levels) and PTH status

Complications of CKD: bone/mineral,heart, anemia, acidosis, malnutrition
• Lipid profile in CKD : Hypercholesterolemia
• Lipid profile in nonproteinuric CKD, especially advanced
CKD, is frequently characterized by normal to low total
cholesterol levels, low HDL levels, relatively elevated serum
LDL levels, and elevated TGs
• Elevated levels of lipoprotein a
• Elevated levels of homocysteine, AGEs, and C-reactive
protein

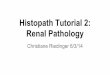
• Q.1) Identify the urinary casts:
Fatty cast
Waxy cast Fatty cast

• Q.2) Idiopathic membranous nephropathy
is a/w which of the following?
Hepatitis B
Hepatitis C
NSAIDs
Antibodies to M-type phospholipase receptor
All of the above

• Q.3)Estimation of GFR in pediatric population is done
by?
Schwartz formula
Cockroft gault formula
MDRD equation
CKD-EPI equation
Any of the above
Cr Cl = k. Height (cms) serum Cr (mg/dl)

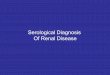
• Q.4) Identify the urinary crystals:
Cystine crystalsTriple phosphate crystals

Thank you