Embed Size (px)
Citation preview

Anatomical and Physiological Peculiarities of Respiratory System in Children. Peculiarities of Embryogenesis of
Respiratory Organs and Anomalies in Their Development.

Plan of the lecture
Making up and intrauterine development of respiratory organs.
Peculiarities of the structure of upper respiratory passages.
Middle and lower respiratory passages, peculiarities of their structure in children in different age periods.
Examination of children with diseases of the respiratory system.
Embryogenesis of respiratory organs
From the 3rd week of embryonic development begins the formation of respiratory organs and lasts a long time after the birth of a child.
In the 3rd week of embryogenesis in cervical portion of entodermal tube appears a bulge, which grows rapidly. In the 4th week it divides into two parts- right and left - the future right and left lungs. Each of them in its turn branches up like a tree. Plain muscular fibers and cartilages of bronchi are formed of a mesodermal mesenchima.

Embryogenesis of respiratory organs
Canalicular phase (recanalization) lasts 16-26 weeks. This time takes place formation of holes in bronchi, continues development and vascularization of the future respiratory sections of the lungs.
Completing phase (alveolar)- period of the formation of alveoli - begins in the 24th week. To the moment of the child’s birth it does not finish and formation of alveoli continues also in postnatal period.

Sponsored Sponsored
Medical Lecture Notes – Medical Lecture Notes – All SubjectsAll Subjects
USMLE Exam (America) – USMLE Exam (America) – PracticePractice

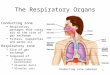
In anatomical structure respiratory organs are divided into:
upper respiratory passages (nasal cavity, pharynx, larynx);
middle respiratory passages (trachea, bronchi);
lower respiratory passages (bronchioli, alveoli).
In children in different age periods are noticed peculiarities of respiratory organs structure.

Peculiarities of the structure of upper respiratory passages:
Nose: small sizes; nasal passages are narrow; in children of the first years of life is absent the lower nasal
passage (its development finishes by 4 years of age); mucous membrane is gentle, well vascularized, inclined to
quick edemas; lymph system of the nose is connected with subdural and
subarachnoidal areas, promoting generalizing infection.

Peculiarities of the structure of upper respiratory passages:
Additional sinuses: underdeveloped (in newborns only sinusoidal
and cribrate are in germinal state, which Rtg are detected from 3 months);
from 2 years of life is developing frontal and from 6 years - the main sinuses, due to which in children of early age never are sinusitis.

Peculiarities of the structure of upper respiratory passages:
Pharynx:is relatively short and narrow;internal hearing passage, which opens in rhinopharynx, is rather wide and straight and this promotes development of medial otitis;lymphatic ring of Pirogov-Valdeiern in newborns is underdeveloped, cripts are absent. Due to this in the first years of life anginas arise very seldom. By 2-3 years of life there is intensive development of tonsils, especially rhino-pharyngeal ones. Clinically this is demonstrated by adenoids.

Peculiarities of the structure of upper respiratory passages:
Larynx: short, wide, funnel like, with gentle mild cartilages, thin
muscles; localized high; rima glottis is narrow, vocal cords are short, due to this the
children have loud voice; mucous membrane is thin, gentle, rich of vessels, submucous
layer is hydrophilic. This promotes quick development of swelling and development of “wrong croup";
in submucous membrane there is much lymphoid tissue. Sex differences in the structure arise beginning with 10 years
of age (in boys the angle of the cartilage becomes acute, the entrance widens, vocal cords become longer; in girls – lengthening is not considerable, larynx is shorter and wide).

Peculiarities of the structure of upper respiratory passages:
Trachea: narrow, ellipsoid shape (in newborns) and ring like
(in older children); cartilage is narrow, mild; mucous membrane is gentle, well vascularized; bifurcation of trachea is located higher (at the level of
3rd dorsal vertebra); weakly fixed, lightly displaces; the number of mucous glands is not large (dryness as
a result).

Peculiarities of the structure of upper respiratory passages:
Bronchi: the right bronchus is wider. Goes almost vertically, the left
bronchus is narrow and goes out under angle (in newborns equal angles of going out). Due to this –most of the foreign bodies enter the right bronchus.
the system of branching out of bronchi is rough, less muscular fibers. With age branching out of bronchi becomes finer and to 7th year the process is completely finished.
histological structure of bronchial walls is characterized by the presence of hyaline cartilage plates, weak muscular layer, poor elastic fibers (there is no adequate cough);
mucous membrane is thin, well vascularized, but dry.

Peculiarities of the structure of lower respiratory passages
The lungs: by the 4th month the number of alveoli becomes more; after 4 months continues the process of increasing the sizes at the
account of differentiation of the existing apparatus; characteristic rough branching out of the bronchial tree; histological structure of a lung is characterized by the presence of
loose connective tissue in interlobular membranes and poor elastic tissue;
forming of Kohn pores (interalveolar complexes); well developed net of blood vessels and accompanying lymphatic
nodes; respiratory function depends on the maturity of corresponding
apparatus.

Peculiarities of the chest
The chest: convex, short; in newborns has round cross (barrel shaped); horizontal going out of ribs from the spine; in the first months of life the lungs are larger than the
chest and are pressed into the ribs; the chest is in the stage of breathing in; breathing musculature is poorly developed.

Peculiarities of respiration in children
superficial, depth – 8-10p. less than in adults; large rate of breathing: in newborns – 50-60 - 1 min; 2 weeks-3 months – 40-45 – 1min; 3-6 months – 35-40 - 1 min; 7-12 months- 30-35 – 1 min; 2-3 years – 25-30 – 1 min; 4-6 years – 20-25 – 1 min; 7-12 years – 2—22 – 1 min; 14-15 years – 18-20 –1 min; adults – 16 – 1 min.

Peculiarities of respiration in children
arrhythmia in children – breathing in is shorter than breathing out, pauses are different. During sleep – they are rhythmical ;
the type of breathing depends on age and sex; newborns and 1 year –abdominal type of breathing; 2 years – 8-9 years – mixed type; from 10 years –in boys – abdominal; girls – breast.

So, taking into account the above said, it can be concluded that in children of younger age there are more “favourable” conditions for the development of respiratory organs pathology.

Methods of examination of children with respiratory organs pathology
1.Clinical: A). questioning (complaints, anamnesis of the disease,
anamnesis of life); B). survey; C). palpation; D). percussion; E). auscultation. 2. Paraclinical: A). Laboratory general blood analysis, biochemical blood analysis, analysis of
sputum.

Methods of examination of children with respiratory organs pathology
B). Instrumental rentgenological- rentgenography of the lungs, tomography,
rentgenography of nasal cavity, bronchography, radiological scanning of the lungs;
endoscopic (bronchoscopy, laryngoscopy). C).Functional of the function of external breathing – spirography with
determination of vital capacity of the lungs (VCL), forced VCL, maximal ventilation of the lungs (MVL), rate of air flow on breath in and breath out;
functional methods of examination with the use of pharmacological probes.

Methods of examination of children with respiratory organs pathology
D). Microbiological methods: samples from fauces and nose, examination of bronchial secret, pleural sweat.
E). Allergological diagnostics: skin (applications, scarification) probes with allergens. Determination of general IgE and specific IgE to different allergens.
F). Oxygenometria: direct (determination of oxygen saturation of blood) and indirect (dynamics of saturation).

Cough
– – defense act of the organism - discharging from the respiratory passages nasal mucus, exudates, foreign bodies.
Relatively narrow lumen of respiratory passages in children of an early age, poor development of muscular membrane of bronchi promote incompleteness of cough pushes.
According to rhythm cough can be divided into: cough as separate coughing pushes (weak cough): in
neuroses, sinusitis, in the early stages of tuberculosis); periodical cough – in patients with pneumonia, chronic
bronchitis. A variation is cough attack, which is the main symptom of whooping cough.
Permanent cough – characteristic of patients with pharyngitis, acute bronchitis.

Cough
If cough is not accompanied with discharge of sputum, it is called dry, and with sputum discharge – moist cough.
according to timbre there are such kinds of cough:
barking – in laryngitis; loud (as in the tube) – in tracheitis.

Sputum
pathological discharges from respiratory passages. The amount of sputum always is different:
little – in bronchial asthma, acute bronchitis, interstitial pneumonia;
much – in bronchoectasis, abscessing pneumonia. According to character of pathological process sputum can be: mucous (colorless, transparent, thick), mico-purulent (thick, turbid, contains mucus and pus), purulent (in severe purulent bronchitis, abscesses), bloody (bleeding in upper respiratory passages, tuberculosis,
high blood pressure in lesser blood circulation circuit).

In microscopy in sputum can be:
neutrophils – fresh purulent process; eosinophils – bronchial asthma, bronchitis; alveolar cells – fresh inflammatory process; in bronchial asthma – spirals of Kurshman,
crystals of Sharko-Leiden.

Pains in the chest
arise in diseases of respiratory system as well as during the diseases of all other organs in the chest cavity. Pains in the chest may cause forced position (in pleuropneumonia, pleuritis).
Generally the pains are acute, intensive, increase in deep breathing, during cough, moving the arms.

Change of the voice in a child
indicates on the disease of mucous membrane of larynx with lesion of the vocal cords. Under acute respiratory infections (more often in paragrippe) develops edema of mucous membrane beneath the vocal cords- laryngitis, clinically demonstrated by rough barking cough and harsh voice. In diphtheria of larynx, when croupous inflammation of vocal cords develops with formation of a film, the voice is lost (aphonia). Nasal shade of the voice takes place in chronic rhinitis and adenoids, retropharyngeal abscesses, tumors of tonsils. Harsh low voice is characteristic of mixedema.

Change of respiration rate
Slowing of respiration rate (bradypnea)- is met rarely. The main reason – hindered function of respiratory center (severe intoxication, renal insufficiency, hepatic insufficiency).
Increase of respiration rate (tachypnea) is observed under diseases of respiratory and cardiovascular systems, anemias, inflammations, pains.

Dyspnea Dyspnea is acceleration and hardening of respiration.
Objective symptoms of dyspnea are change of rhythm, respiration rate and participation of additional respiratory muscles.
Differentiation: - inspiratory dyspnea – hardened loud breathing in (in
stenosis of the larynx, foreign bodies in trachea, true croup); - expiratory dyspnea – hardened prolonged breathing out
with participation of abdominal muscles. It can take place in narrowing the lumen of bronchi, bronchioles at the account of edema or their spasm. Is characteristic of obstructive bronchitis, bronchial asthma;
mixed – hardened breathing in and breathing out. It can take place in disturbed pulmonary tissue, pleura, diseases of the heart, ascites, meteorism.

Change in the type of respiration
Change of thoracic type of breathing for abdominal one in girls appears in traumas of the ribs, myositis, fibrinous pleuritis.
Change of abdominal type of breathing for thoracic one in boys is a witness of peritonitis, lesion of diaphragm, ascites, meteorism.

The shape of the chest In healthy children of an older age the chest is cylinder-shaped. In emphysema of the lungs, bronchial asthma, obstructive
bronchitis- the chest is short and wide - barrel-shaped. Such shape of the chest is physiological in newborns: anterior-posterior size is actually equal to transversal, horizontal branching of the ribs.
Intercostal spaces in healthy children are the same. Widening, falling out are characteristic of exudative pleuritis, hydro- and pneumothorax.
Narrowing and extension – for chronic broncho-pulmonary processes.
In healthy children the chest is symmetrical. In pathology the symmetry is violated with signs of retraction (chronic fibrinous process in the lungs- exudative pleuritis, pneunothorax).

Pathological symptoms in palpation
Increasing of vocal fremitus- during pathological processes in pulmonary tissue, accompanied by its consolidation (in pneumonias).
Weakening of vocal fremitus - in pleuritis, pneumothorax, atelectasis, pleural tumors.
Can also depend on factors not connected with pathological processes (obesity, edemas, sharp physical weakness).

Changes in percussion sound
Loss of resonance or dull sound instead of clear one is observed in:
decrease of the amount of air in pulmonary tissue (inflammation, tuberculosis, atelectasis);
formation in the lungs another airless tissue (tumor, abscess);
filling up the pleural cavity with fluid (pleuritis). This symptom can also be present in pathology of
trachea-bronchial lymph nodes, cardiovascular system pathology, thymomegaly, tumors of mediastinum.

Changes in percussion sound
Thympanic sound appears in: formation in the lungs a cavity, full of air
(cavern, cyst, pneumothorax); decreasing of elasticity of pulmonary tissue
(emphysema). Besides, in high location of diaphragm (meteorism).
Boxing sound - arises when pulmonary tissue elasticity is sharply decreased (BA, emphysema).

Physical changes (auscultation symptoms)
Normally above the pulmonary areas is heard vesicular respiration (we hear breathing in and 1/3 of breathing out) - sound “f”.
Above the trachea, larynx, area of location of large bronchi in healthy children we hear bronchial respiration - sound “h”.

Physical changes (auscultation symptoms)
Vesicular breathing, in which breathing in is shortened, and breathing out is almost unnoticed, is called weakened breathing. Can be observed physiologically:
in newborns and 6 months; in obesity; well developed muscular tissue: pathologically: in tracheal or bronchial occlusion; initial stages of pneumonia; under limited respiratory movements; in exudative pleuritis, hydrothorax;

Physical changes (auscultation symptoms)
harsh breathing - such breathing in which respiratory murmurs are sharply expressed and equally well is heard breathing in and breathing out.
most frequently is present in bronchitis.
Physical changes (auscultation symptoms)
If bronchial breathing is determined above the pulmonary areas, it is considered to be pathology (in considerable, wide spread consolidation of pulmonary tissue - polysegmentary, croupous pneumonia, tuberculosis, atelectasis).

Rales
are additional respiratory murmurs, which arise in trachea, bronchi, pulmonary cavities due to motion and vibration of exudate. Differentiation:
dry and moist rales. Dry rales: whistling - obstructive bronchitis;
buzzing - acute simple bronchitis;
in bronchial asthma - different rales. Moist rales: fine-, medium-, large-, bubbling rales.

Auscultation changes in bronchitis and pneumonias:
in bronchitis rales are heard - along the whole length of the lungs;
in pneumonia - localized; in bronchitis- changing in localization; in pneumonia- persistent; in bronchitis-not loud; in pneumonia - loud (due to infiltration and
consolidation of the lungs tissue).

Peculiarities of crepitation :
is heard at the end of breathing in; does not change during cough; is scattered in type of localization; has a uniform caliber of murmurs.
Crepitation - characteristic sign of pneumopathias,croupous pneumonia.

Pleural murmur
Additional respiratory murmur, which arises under pleural pathology (friction of visceral and parietal layers of pleura). Differentiation of pleural murmur and crepitation is done according to the following criteria:
heard both stages of respiration; in pressing with phonendoscope the phenomenon
increases; heard more superficially; while imitating respiration, crepitation is not heard,
but pleural murmur is preserved.