Embed Size (px)
Citation preview

Risk Stratification of “Mild” Traumatic Brain Injury
Frederick Korley, M.D., Ph.D.

Statement of Problem
Korley FK, Pham JC, Kirsch TD: Use of advanced radiology during visits to US emergency departments
for injury-related conditions, 1998-2007. JAMA 304(13): 1465-71, 2010.
4.8 million persons evaluated in the ED for TBI
each year
2.5 million diagnosed with TBI
Korley FK, Kelen GD, Jones CM, Diaz-Arrastia R: Emergency Department Evaluation of Traumatic Brain Injury in the United States, 2009-2010. J Head Trauma Rehabil. 2015 Sep 10
Korley FK, Pham JC, Kirsch TD: Use of advanced radiology during visits to US emergency departments for injury-related conditions, 1998-2007. JAMA 304(13): 1465-71, 2010.

Hypothesis
A data-driven, multi-disciplinary approach utilizing novel methods (proteomics, genomics, metabolomics, advanced imaging) for characterizing patient and injury characteristics, and coupled with existing clinical data will improve TBI risk-stratification.

Head Injury Serum Markers for Assessing Response to Trauma (HeadSMART) Cohort
• Prospective observational cohort• Two demographically distinct academic EDs• Data: NINDS common data elements • Serum, plasma and mRNA sampling at 0, 4, 24 hours; 3
and 7 days; 1, 3 and 6 months. DNA at baseline• Outcome assessment
• Phone• Battery of cognitive and psychiatric assessments in
person

What is TBI? Who should be included in studies?
• American congress of Rehabilitation Medicine’s Definition• Traumatically induced physiological disruption of brain
function, as manifested by:• LOC• Memory loss• Altered mental status• Focal neurologic deficit
• What about head injury not meeting “TBI” criteria?• Head Injury BRain Injury Disputed (HIBRID)

Risk of prolonged recovery in HIBRID patients
• To determine the risk of prolonged recovery in HIBRID patients
• Method: • Population:
• HeadSMART TBI patients categorized as: HIBRID, ACRM+ CT-; ACRM+ CT+
• Control groups: Non-head injury trauma controls, healthy controls
• Outcomes:• Disability (Glasgow Outcome Scale Extended)• Post-concussive symptoms (Rivermead Post-
Concussive Questionnaire)• Depression (Patient Health Questionnaire 9)

Recovery at 1 month Post-Injury

Patients’ expectations
You were evaluated for a head injury during your visit. What is your understanding regarding how well you will heal from this head injury?
Accuracy based on functional disability
Accuracy based on post-concussive symptoms
Discussed with physicians, high risk (n=7) 57.1% 42.9%Discussed with physicians, low risk (n=38) 55.3% 60.5%Did not discuss, high risk (n=9) 100% 75.0%Did not discuss, low risk (n=38) 60.5% 57.9%Did not discuss, no idea (n=12) 58.3% (poor),
41.7% (good)50.0% (poor), 50% (good)

How good is clinician gestalt for identifying high risk?
Based on what you know now about this patient's presentation, do you think this patient will have a complete functional recovery i.e. they will be back to their pre-TBI functional state at 3 months after injury?
Accuracy based on functional disability
Accuracy based on having post-concussive symptoms
Yes 53.9% 59.4%No 40.0% 61.6%
Based on what you know now about this patient's presentation, do you think this patient will have 3 or more post-concussive symptoms (for example: headaches, fatigue, insomnia, loss of concentration, noise and light sensitivity, memory loss, dizziness) at 3 months after injury?
Accuracy based on functional disability
Accuracy based on having post-concussive symptoms
91 – 100% certain
37.3% 68.9%
71 – 90% certain
55.6% 52.2%
<70% certain 60.0% 59.5%

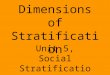
Day-of-injury serum BDNF can predict risk

Day-of-injury serum BDNF can predict risk
p = 0.005

Ongoing Work
• Examine the diagnostic and prognostic utility of the following biomarkers in TBI: GFAP, S100B, BDNF, Troponin, Total tau, phosphorylated Tau, ICAM 5, Neurogranin, beta synuclein, among others
• Evaluate the effect of catecholamine surge in TBI and its effect on cerebrovascular reactivity
• Examine the metabolomic profile of recovery from TBI• Develop prognostic models using machine learning tools

Acknowledgements
• Patients and Family Members• Subject Enrollment
– Hayley Falk M.Sc– AJ Hall– Freshta Akabari– Uju Ofoche – Olivia Lardo– Braden Anderson
• Neuropsychiatry– Alex Vassila B.S.– Vani Rao M.D.– Durga Roy M.D.– Matthew Peters M.D.– Kostas Lyketsos M.D., M.P.H.
• Neurocognitive/Rehab– Kathleen Bechtold Ph.D.
• Neurology– Ramon Diaz-Arrastia M.D., Ph.D
• Proteomics– Allen Everett, M.D.– Jenny Van Eyk, Ph.D.– David Lubman, Ph.D.
• Metabolomics– Charles Burant, Ph.D.
• Neuroradiology– Haris Sair M.D.
• Machine learning– Scott Levin Ph.D.– Kayvan Najarian, Ph.D.
• Funding– ImmunArray– Biodirection– Robert Wood Johnson Medical
Faculty Development Award– University of Michigan Injury
Center