Embed Size (px)
Citation preview
Malaysia
RMTAC
Protocol & Tools
involved
Pharmacist
Outline of presentation Protocol of RMTAC
What you should know?
Workflow of RMTAC
Documentation
Statistics
Tools need to prepare Questionnaires- ACT, CAT
Inhalers-placebo
Test- spirometry, peak flow meter
Flipchart of Inhaler/Handbook
Flipchart of the Disease
Respiratory diary (asthma diary)
PROTOCOL BOOK
http://www.pharmacy.gov.my/v2/sites/default/files/document-
upload/book.-protocol-respiratory-2.6-fa.pdf
2010 2015
What you should know? Malaysia RMTAC- introduced in 2004.
started by Hospital Melaka by former KPF, Tn Hj Malek.
RMTAC- work in a team
◦ Chest physician/Family Med specialist
◦ Nurse
◦ Lab technician
◦ Pharmacist : 1-4 person/team
Working hours- usually on respi clinic day
Place to counsel patient- room at the clinic
Before start the MTAC program, inform JKNS
What you should know? Main Objectives of RMTAC
◦ To help patients in managing their Asthma &COPD.
• Other objectives:
◦ To maximize the benefits of medication therapy in Asthma/COPD
patients.
◦ To increase patient’s adherence towards Asthma/COPD medications.
◦ To educate and encourage patients/caregivers on the appropriate use
of Asthma/COPD medications and self-care inhalers/devices.
◦ To minimize adverse effects or complications resulting from the
Asthma/COPD medications and/or multiple drug regimens.
◦ To reduce the frequency of emergency room visits and thus, reduce
the total health care costs in treating Asthma/COPD.
◦ To collaborate with consultative services physicians and other health
care professionals on Asthma/COPD medication related issues.
Scope of service
Operate in the clinic area, during clinic days
Pharmacist role :-
◦ Assessing patients for pharmaceutical care
issues,
◦ providing appropriate education to patients and
caregivers,
◦ completing follow-up sessions and
◦ documenting actions and plans in relevant
RMTAC forms
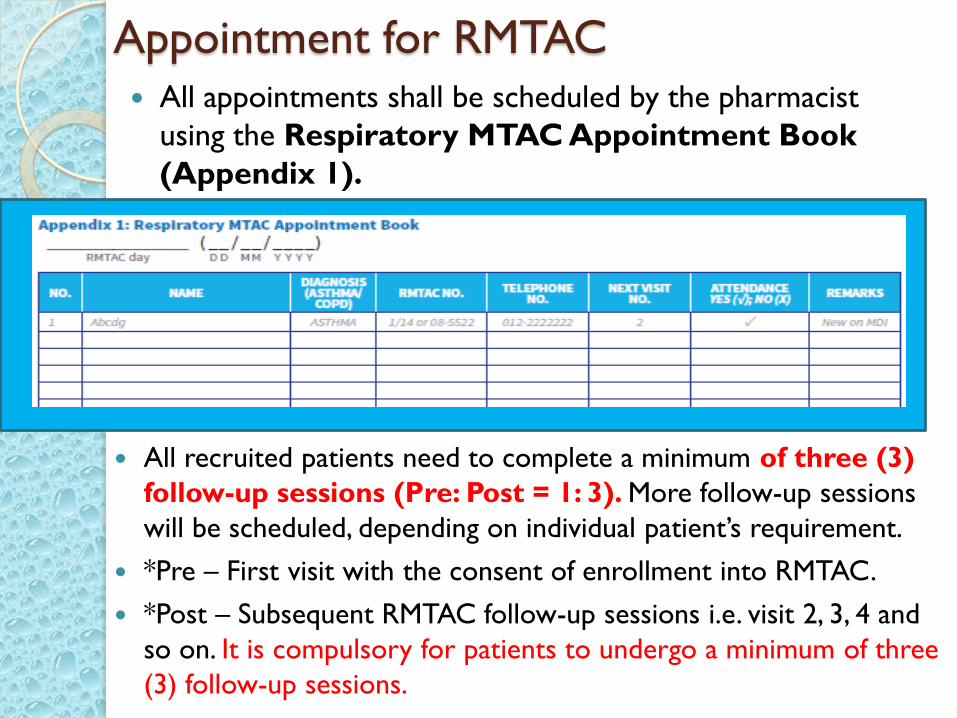
Appointment for RMTAC All appointments shall be scheduled by the pharmacist
using the Respiratory MTAC Appointment Book
(Appendix 1).
All recruited patients need to complete a minimum of three (3)
follow-up sessions (Pre: Post = 1: 3). More follow-up sessions
will be scheduled, depending on individual patient’s requirement.
*Pre – First visit with the consent of enrollment into RMTAC.
*Post – Subsequent RMTAC follow-up sessions i.e. visit 2, 3, 4 and
so on. It is compulsory for patients to undergo a minimum of three
(3) follow-up sessions.
Patients diagnosed with Asthma/COPD, who fulfill at least ONE of the following criteria, should be offered to be recruited into the RMTAC:
Patients with Childhood Asthma Control Test (C-ACT)
or Asthma Control Test (ACT) score of ≤ 19.
Patients with uncontrolled Asthma according to latest
GINA Guidelines.
Patients with frequent Asthma/COPD exacerbation
according to latest GINA/GOLD Guidelines.
Patients with poor inhaler technique.
Patients with low adherence to medications (Morisky
Medication Adherence Scale score < 6).
Who shall be recruited?
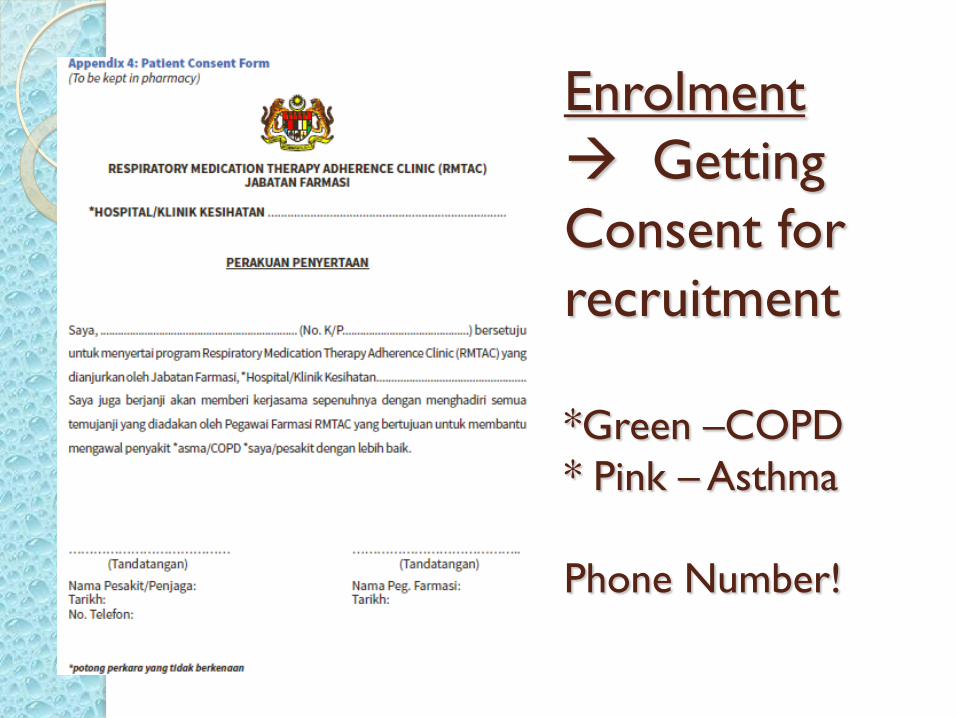
Enrolment
Getting
Consent for
recruitment
*Green –COPD
* Pink – Asthma
Phone Number!
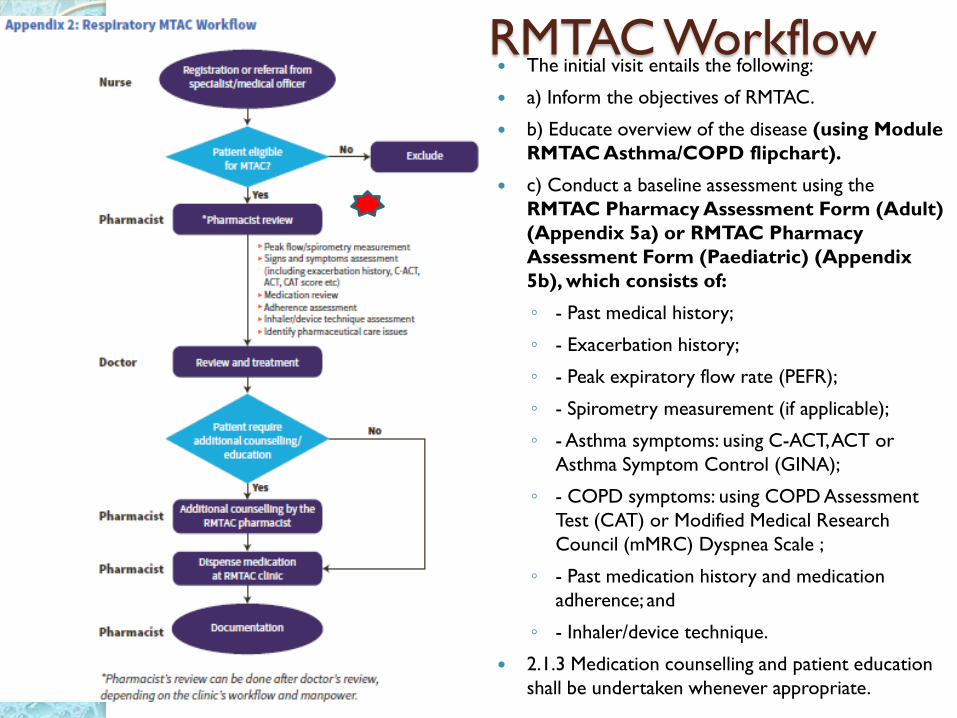
RMTAC Workflow The initial visit entails the following:
a) Inform the objectives of RMTAC.
b) Educate overview of the disease (using Module
RMTAC Asthma/COPD flipchart).
c) Conduct a baseline assessment using the
RMTAC Pharmacy Assessment Form (Adult)
(Appendix 5a) or RMTAC Pharmacy
Assessment Form (Paediatric) (Appendix
5b), which consists of:
◦ - Past medical history;
◦ - Exacerbation history;
◦ - Peak expiratory flow rate (PEFR);
◦ - Spirometry measurement (if applicable);
◦ - Asthma symptoms: using C-ACT, ACT or
Asthma Symptom Control (GINA);
◦ - COPD symptoms: using COPD Assessment
Test (CAT) or Modified Medical Research
Council (mMRC) Dyspnea Scale ;
◦ - Past medication history and medication
adherence; and
◦ - Inhaler/device technique.
2.1.3 Medication counselling and patient education
shall be undertaken whenever appropriate.
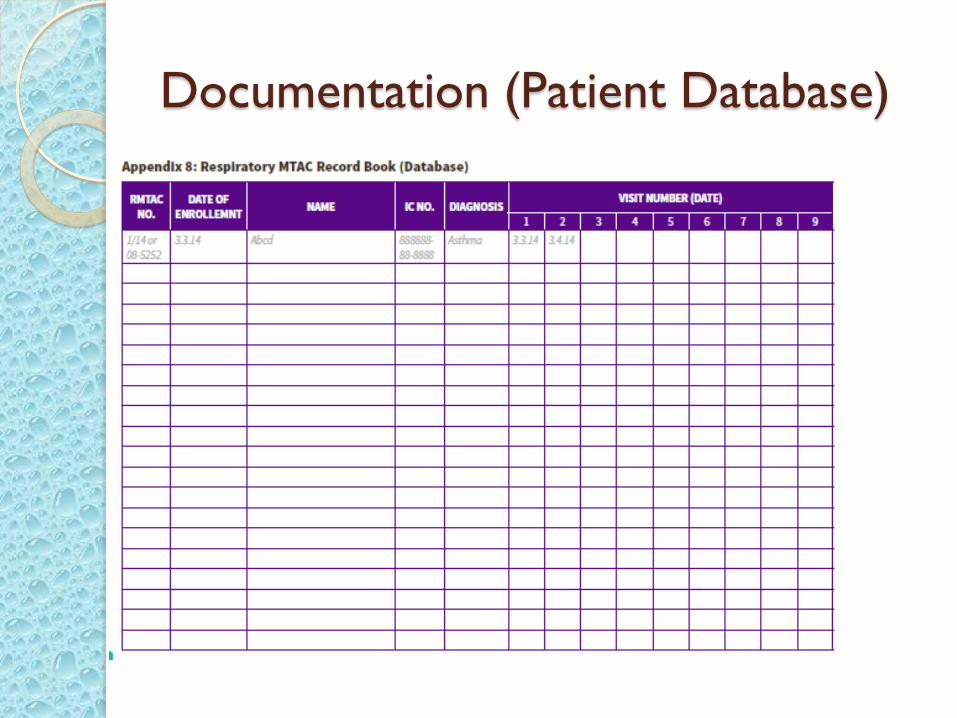
Documentation (Patient Database)
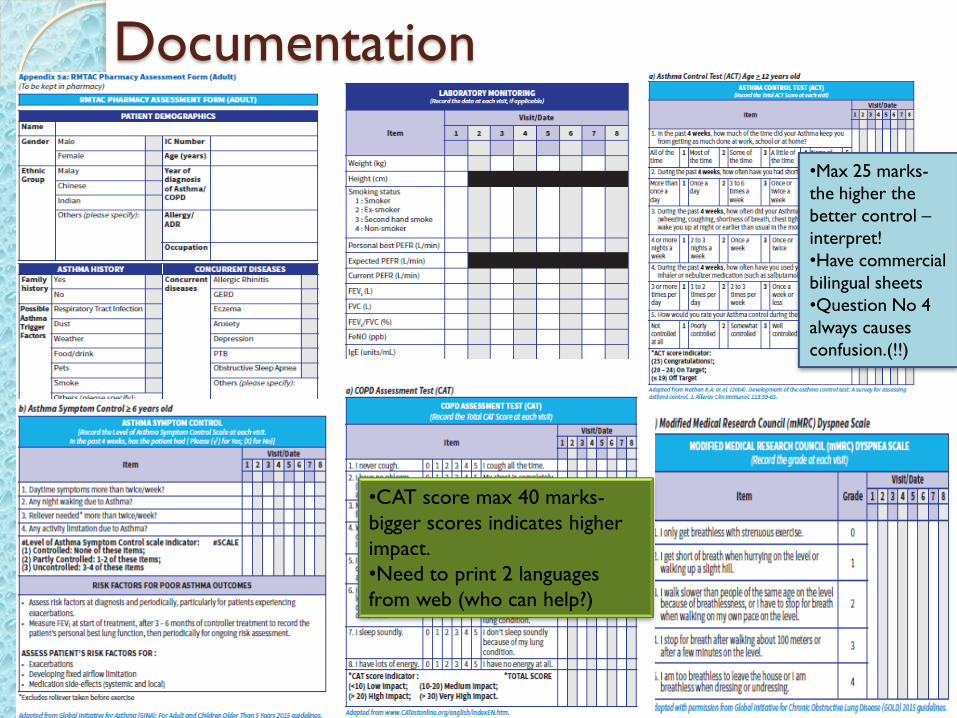
Documentation
•Max 25 marks-
the higher the
better control –
interpret!
•Have commercial
bilingual sheets
•Question No 4
always causes
confusion.(!!)
•CAT score max 40 marks-
bigger scores indicates higher
impact.
•Need to print 2 languages
from web (who can help?)
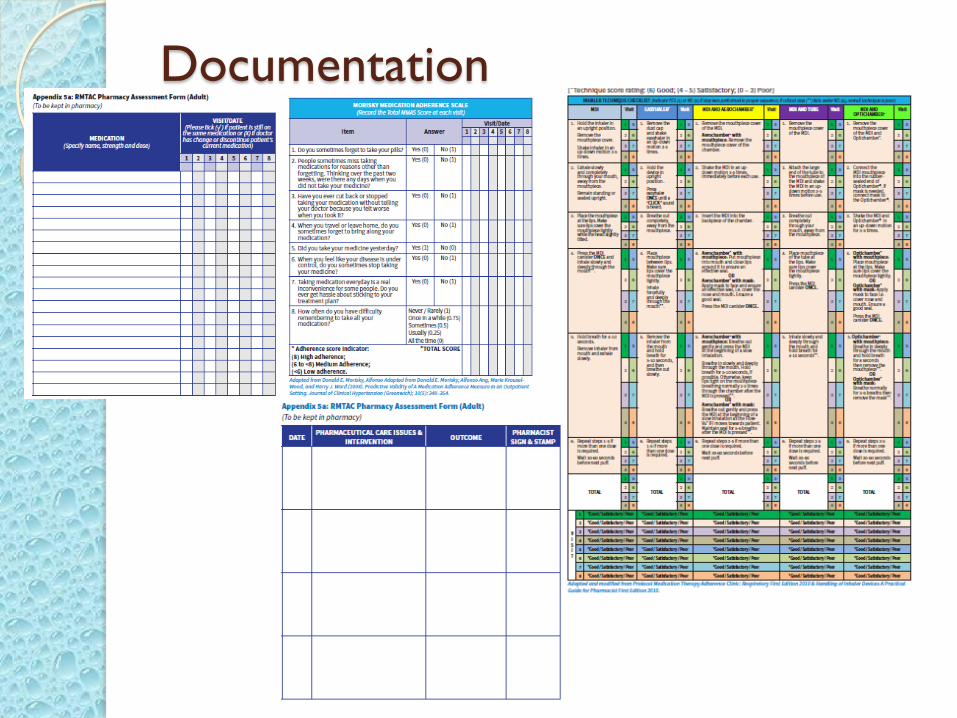
Documentation
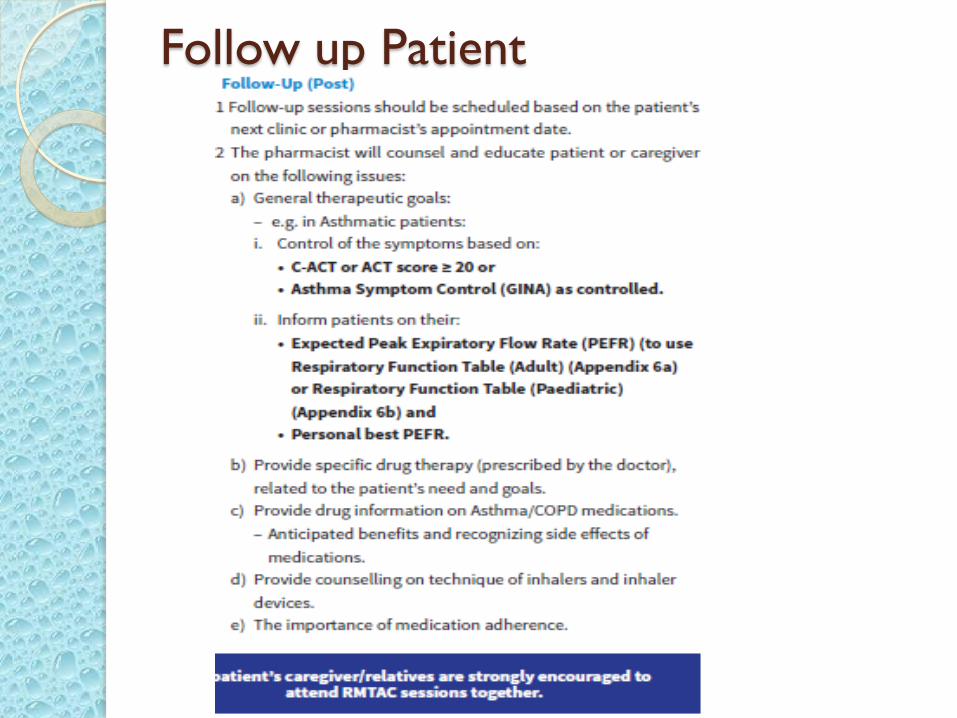
Follow up Patient
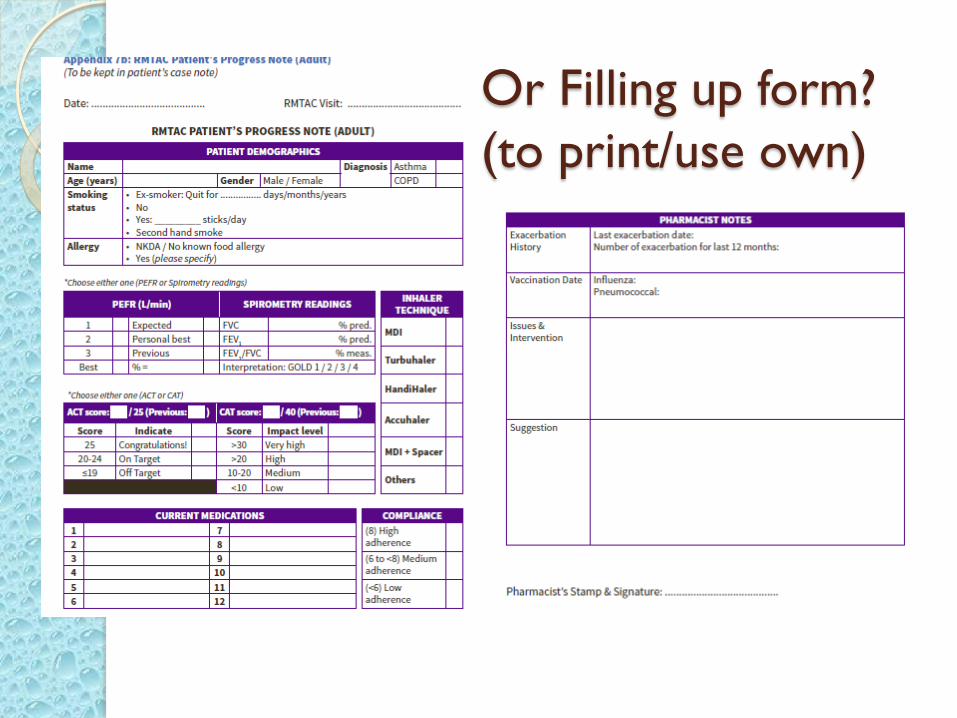
Or Filling up form?
(to print/use own)
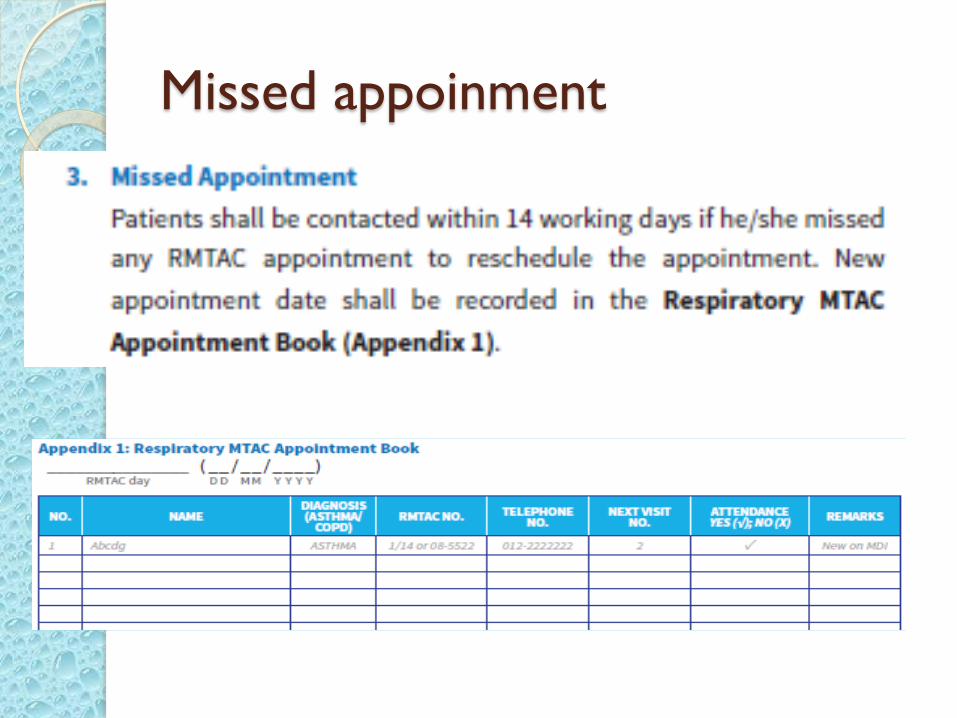
Missed appoinment
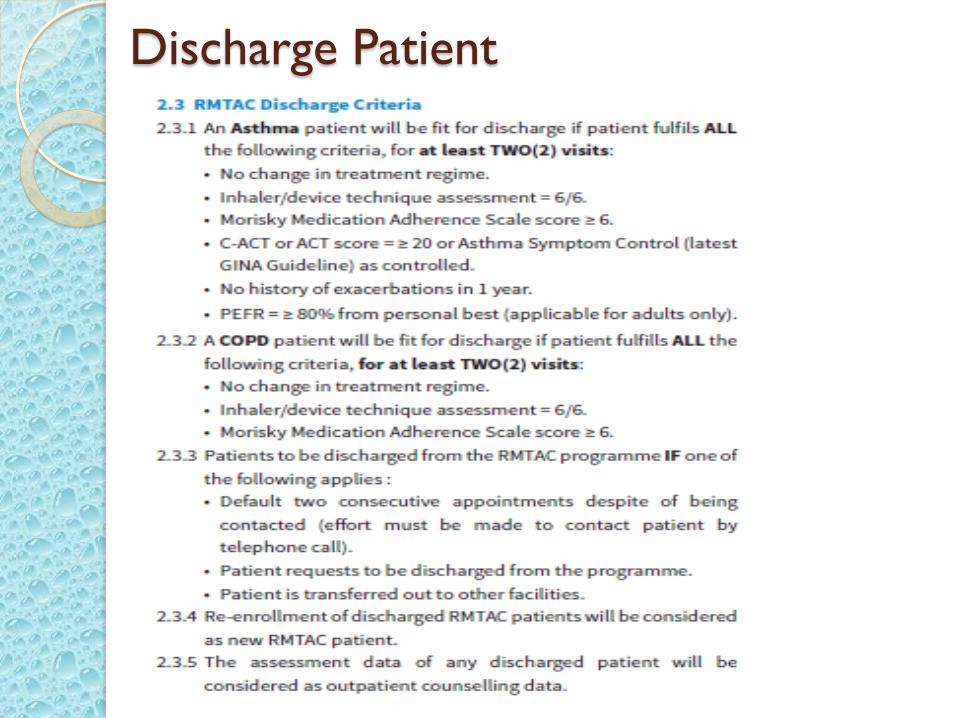
Discharge Patient
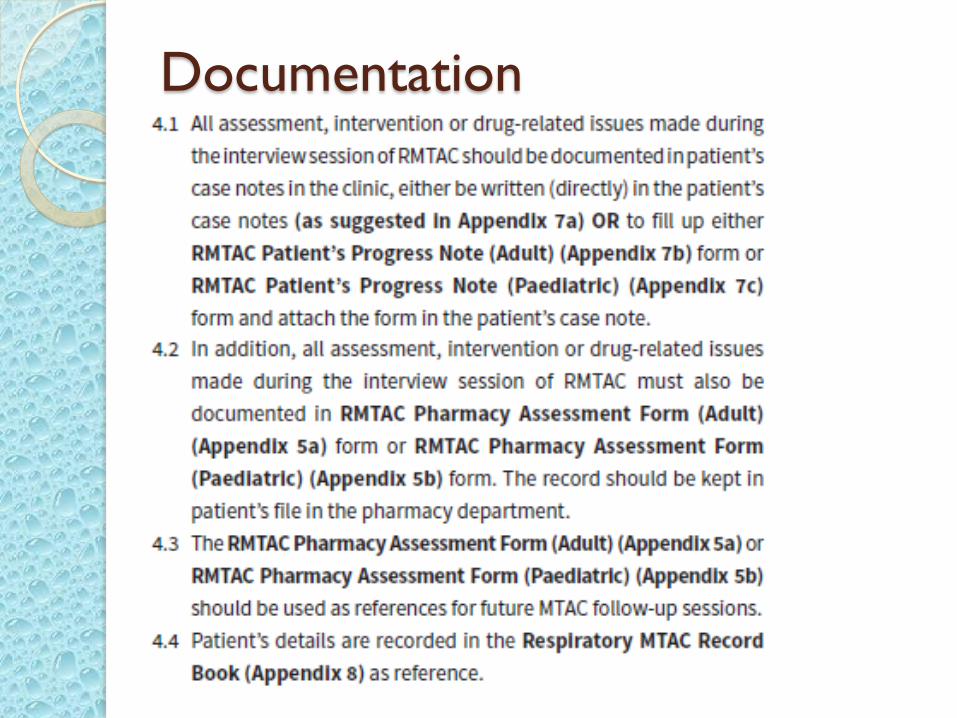
Documentation
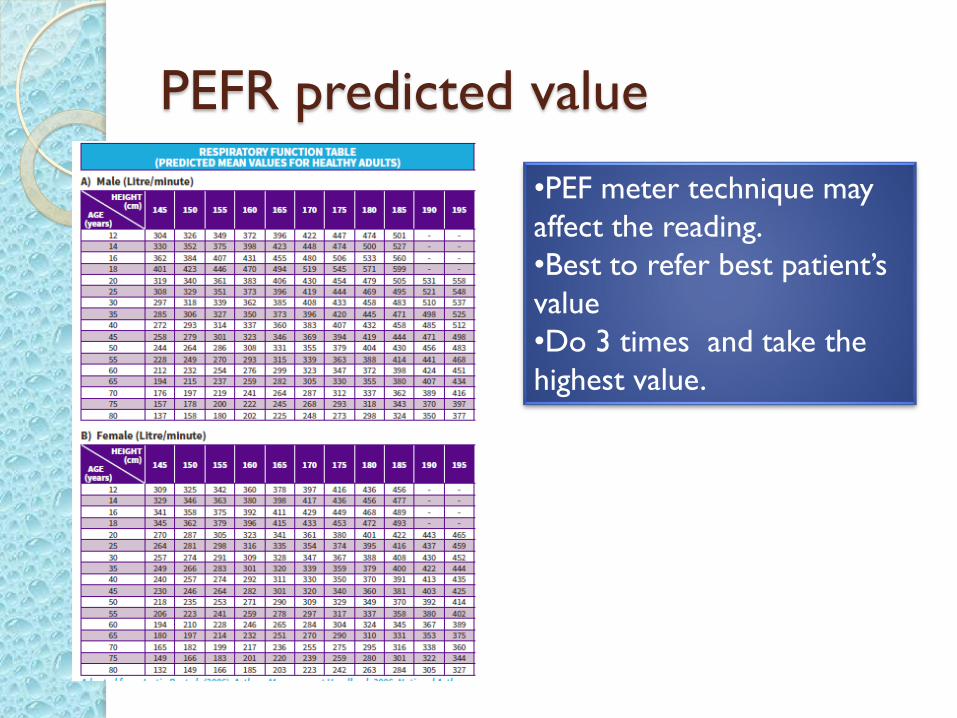
PEFR predicted value
•PEF meter technique may
affect the reading.
•Best to refer best patient’s
value
•Do 3 times and take the
highest value.
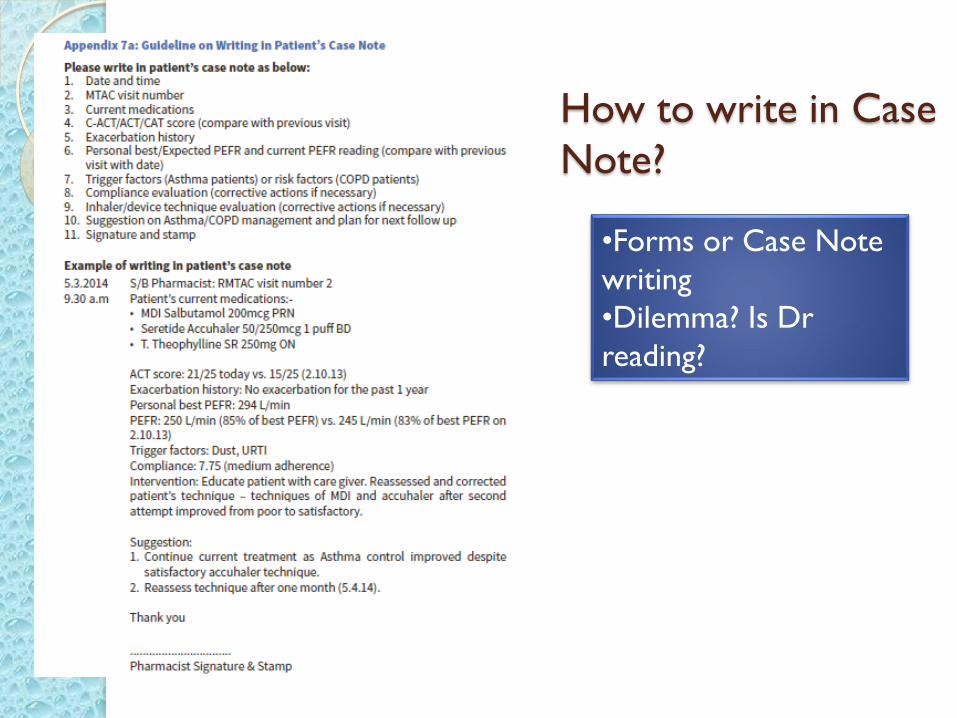
How to write in Case
Note?
•Forms or Case Note
writing
•Dilemma? Is Dr
reading?
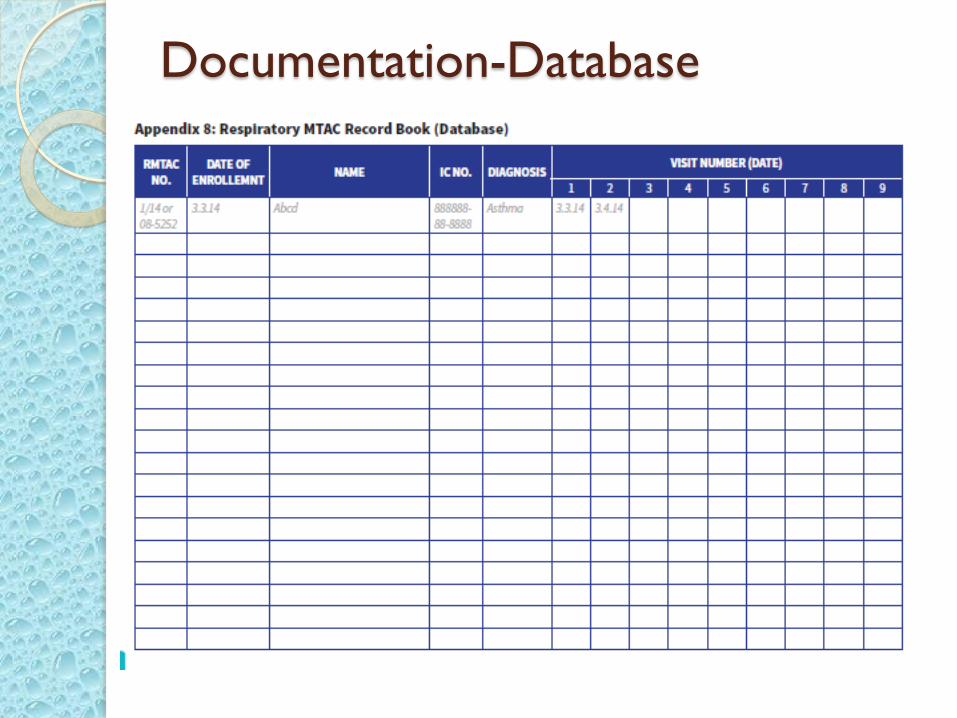
Documentation-Database
TOOLS
Questionnaires- ACT, C-CAT & COPD test
Inhalers-placebo
Test device- spirometry, peak flow meter
Inhaler flipchart
Disease flipchart
Inhaler handbook
Respiratory diary (asthma diary)
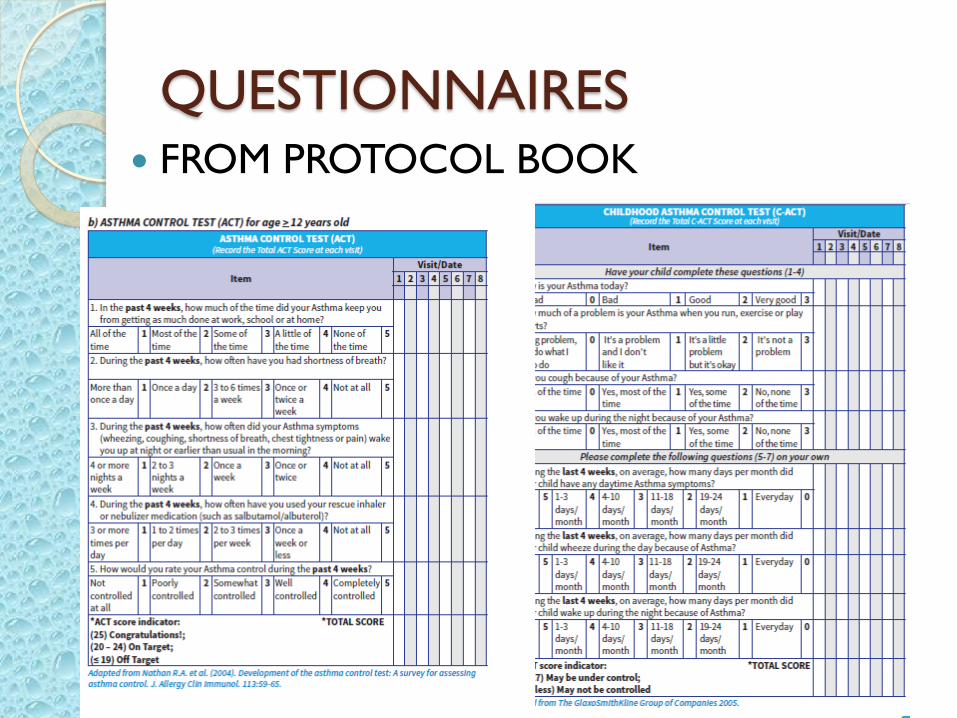
QUESTIONNAIRES FROM PROTOCOL BOOK
PLACEB0
FLIP CHART
25

FLIP CHART TEKNIK PENGGUNAAN
UBAT SEDUT
26
BUKU TEKNIK INHALER
27
ACTIVITIES Baseline Knowledge
◦ Pre Test –MCQ (1 hour)
◦ Assessment on Inhalers technique
Introductory Lectures
A) General
◦ Activities in the clinic and ward
◦ Objectives of Respiratory MTAC(RMTAC)
◦ Protocol and documentation (refer to Respiratory MTAC Protocol: Asthma/COPD (Adult & Paediatric) 2nd Edition 2015 & use of CP1, CP2, CP3, CP4 & counselling form)
◦ Inhaler technique (refer to Respiratory MTAC Protocol: Asthma/COPD (Adult & Paediatric) 2nd Edition 2015 or any other updated relevant references)
◦ **Science behind inhalation (additional)
◦ ** Study discussion
B) Asthma
◦ Pathophysiology (disease, risk & trigger factors)
◦ Management and pharmacotherapy (GINA etc)
◦ Assessment tools (ACT, Level of Asthma Symptom Control, PEFR, laboratory investigation)
C) COPD
◦ Pathophysiology (disease, risk factors)
◦ Management and pharmacotherapy (GOLD etc)
◦ Assessment tools (CAT, mMRC, FEV1, laboratory investigation)
Ward Attachment : ◦ Rounds with physicians (at least 6 rounds)
◦ Clerk case (6 cases)
MTAC Attachment : ◦ Observation 2 cases (1 Asthma & 1 COPD)
◦ Hands-on and case clerking - 4 cases (2 enrolment / new case) -1 Asthma & 1 COPD; 2 follow-up (1 Asthma & 1 COPD)] Entry in case note/ form
ACT/CAT
◦ Medication history taking, patient interview and education
◦ Medication compliance assessment
◦ Medication counselling – technique
◦ Peakflow
◦ Adverse Drug Reaction (ADR) or Allergic Reaction reporting (if any)
◦ Prepare , dispense Medication, and set next TCA
Case Presentation:
◦ 2 cases (1 from RMTAC and 1 from Ward clerking)
Bedside Presentation:
◦ 6 cases (3 COPD; 3 Asthma)
◦ With CP2 and counseling forms
Post Test and Discussion
Case simulations (as needed)























![[Slideshare] Slideshare para tu negocio online](https://img.pdfslide.net/doc/110x75/54ba05494a7959fe4f8b45d7/slideshare-slideshare-para-tu-negocio-online.jpg)





