Embed Size (px)
Citation preview

D R . V . D I N E S A P R A B H U ,
P R O F A N D H O D O F P U L M O N A R Y M E D I C I N E ,
G O V T . M E D I C A L C O L L E G E , T H R I S S U R
RNTCP, Current Guidelines
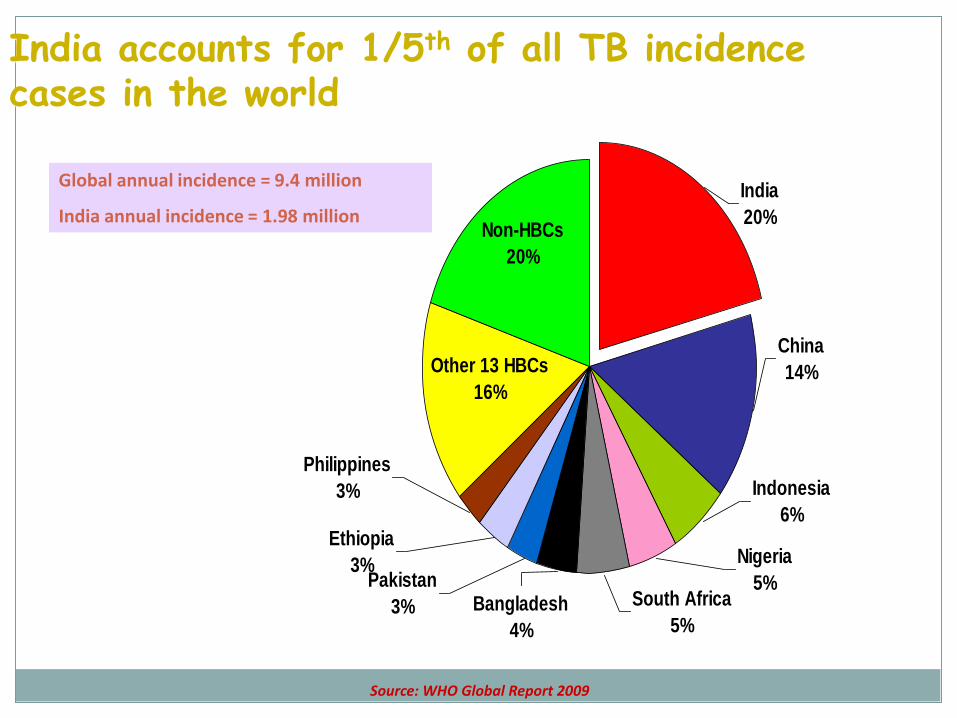
India accounts for 1/5th of all TB incidence cases in the world
Non-HBCs
20%
Pakistan
3%
Ethiopia
3%
Philippines
3%
South Africa
5%Bangladesh
4%
Nigeria
5%
Indonesia
6%
China
14%
India
20%
Other 13 HBCs
16%
Source: WHO Global Report 2009
Global annual incidence = 9.4 million
India annual incidence = 1.98 million

Evolution of TB Control in India
1950s-60s Important TB research at TRC and NTI
1962 National TB Programme (NTP)
1992 Programme Review
only 30% of patients diagnosed;
of these, only 30% treated successfully
1993 RNTCP pilot began
1998 RNTCP scale-up
2001 450 million population covered
2004 >80% of country covered
2006 Entire country covered by RNTCP

Objectives of the RNTCP
To achieve and maintain a Cure Rate of at
least 85% among new sputum smear-
positive patients detected
To achieve and maintain a Case Detection
Rate of at least 70% of all such patients

Revised NTCP Pilot tested in 1993
Uses the DOTS strategy
RNTCP now covers the entire country (all 632
districts; over 1.17 Billion people) – as of 24th
March 2006
Over12.3Million patients put on DOTS in India,
& 2.2million Lives saved

The 5 components of DOTS
Political & administrative commitment
Diagnosis by good quality sputum microscopy
Adequate supply of good quality drugs
Directly observed treatment
Systematic monitoring & Accountability

What is the Scientific
Basis for DOTS?

Scientific Basis of DOTS
Sputum microscopy
Domiciliary treatment
Short course chemotherapy
Intermittent chemotherapy
Directly observed treatment

Sputum microscopy
• Provides definitive diagnosis
• Easy to perform
• Replicable
• Cost effective
• 50% of the new pTB pts. expected to be SS+

Microscopy is More Objective and Reliable than X-ray
Inter-observer variability is much
less with microscopy than with x-
ray
AFB microscopy provides
information on infectiousness of
the patient, which x-ray does not
AFB microscopy allows
prioritization of cases, which x-
ray does not
AFB microscopy is also an
objective method to follow the
progress of patients on treatment

X-ray is an Important Complementary Tool
• Highly sensitive; with low specificity
• Plays a useful supportive role:
• May lead to over-diagnosis
–May miss the diagnosis of other
diseases (e.g. malignancies)
• NOT a good tool for follow-up of
patients on ATT

Other Diagnostic Tests
Mantoux gives evidence of infection, not disease
ESR is not specific
Culture is specific, sensitive But time consuming, costly, requires specialized labs
Other tests like PCR, Ig Assays etc. No value over conventional techniques
Highly sensitive, but poor specificity

Scientific Basis of DOTS
Sputum microscopy
Domiciliary treatment
Short course chemotherapy
Intermittent chemotherapy
Directly observed treatment

The Madras Study
TRC, 1959
Domiciliary treatment as effective as
sanatorium treatment
No additional benefit by bed rest or
special diet
Risk of infection among contacts similar
Most patients do not need hospitalization
Lowered economic burden on society

Scientific Basis of DOTS
Sputum microscopy
Domiciliary treatment
Short course chemotherapy
Intermittent chemotherapy
Directly observed treatment

Short course chemotherapy
TRC studies, 1968 - 87
Favourable results with short courses of ATT
6 months adequate for NSP patients
8 months adequate for retreatment cases
Durations adequate to prevent MDR TB
More convenient and economical
Direct observation more feasible
Improved patient compliance to treatment

Scientific Basis of DOTS
Sputum microscopy
Domiciliary treatment
Short course chemotherapy
Intermittent chemotherapy
Directly observed treatment

Lag period
When tubercle bacilli are exposed to a drug for a short time (6–24 hours) and, after careful removal of the drug, are transferred to a drug free medium, the surviving bacilli start to grow again after an interval of several days.
All tuberculosis drugs have been tested for their ability to produce a lag period, in order to determine whether they are suitable for intermittent regimens

Scientific Basis of DOTS
Sputum microscopy
Domiciliary treatment
Short course chemotherapy
Intermittent chemotherapy
Directly observed treatment

What is the need for DOT?
At least 1/3 of patients on self-administered Rx
fail to adhere to Rx
Impossible to predict which patients will take
medicines
DOT necessary at least in the IP of Rx to
ensure adherence and smear conversion
TB patient missing 1 attendance can be traced
immediately and counseled.

The famous pathanamthitta study

Directly observed treatment
Ensures the best possible results in TB treatment
Observer watches & assists patient swallow the tablets
Ensuring that the patient receives the medication
Many patients who do not receive DOT stop ATT
Poor results and high death rates in the absence of DOT
Observing the patients during the entire course
Ensures that the patient receives the right drugs
Ensures the right doses
Ensures the right intervals

Diagnosis of TB
Cough for ≥2 weeks (TB suspects) screened from OPD/clinics and referred for sputum microscopy
Sputum microscopy performed at quality assured Designated Microscopy Centres (DMCs)
If sputum is initially negative and remains so after a course of antibiotic, despite persisting symptoms, then X-ray chest is done
Standard diagnostic algorithm for pulmonary TB
Patients diagnosed as Sputum +ve and Sputum –ve PTB
Extra-Pulmonary TB is diagnosed based on clinical evaluation and histopathological evidence


Intensive Phase
Aims for a rapid killing of bacilli
A state of non-infectiousness achieved within a short period 2/52
Quick relief of symptoms
Smear negativity by 2/12
Prevent development of drug resistance

Continuation Phase
Aims to eliminate remaining bacilli
Killing of “persisters” prevents relapses
Multi-drug regimens and DOT necessary (unless R not used) even though risk of emergence of drug resistance is less as fewer bacilli remain


Categorization of Patients
Classified into two groups based on H/o previous treatment
New cases: All new pulmonary (sputum positive and negative) and extra pulmonary TB patients
Previously treated cases: Patients who have more than one month Anti TB Rx previously (default, failure and relapse)

Regimen for new cases
Regimen: 2H3R3E3Z3 / 4 R3H3
IP: 8 weeks (24 doses)
CP:18weeks (54 doses)
If sputum is + ive at the end of two months, IP is continued for another one month (12 doses)
CP is for 4 months

New cases cont….
For TBM in new cases, Inj SM is used in place of EMB in IP (H3R3Z3S3 instead of H3R3Z3E3)
CP for patients with TBM and spinal TB is 7 months
Hence total duration of Rx is 9 months
Steroids recommended for TBM and TB Pericarditis

Regimen for Previously treated cases
Regimen: 2S3H3R3Z3E3/1H3R3Z3E3/5H3R3E3
If sputum is + ive at the end of three months, IP is extended for another one month (12 doses, four weeks)
If sputum remains +ive at the end of extended IP, sputum is send to an accredited RNTCP C&DST lab for C&S testing
CP is for 5 months (22weeks, 66 doses) H3R3E3
At least first dose of every week being directly observed
Relapse case have better outcome than Failure and Treatment after default cases

Follow-up Sputum Tests
At the end of Intensive Phase
Two months into Continuation Phase
At the end of Continuation Phase

Drug Resistant case: A patient whose TB is due to tubercle bacilli that are resistant in vitro to at least to one Anti TB drug according to accredited laboratory methods in an RNTCP accredited laboratory
MONO RESISTANCE: A patient whose TB is due to tubercle bacilli that are resistant in vitro to exactly to one anti TB drug in an RNTCP accredited laboratory

POLY RESISTANCE: A patient whose TB is due to tubercle bacilli that are resistant in vitro to more than one anti TB drug, except not due to INH and Rifampicin in an RNTCP accredited laboratory

Multi Drug Resistant Tuberculosis
DEFINITION: An isolate of M. Tuberculosis resistant to at least INH and Rifampicin with or without other antitubercular drugs based on DST result from an RNTCP accredited culture and DST laboratory.
How does drug resistance happen?
When these drugs are misused or mismanaged. When patients do not complete their full course of
treatment;
When health-care providers prescribe the wrong treatment, the wrong dose, or length of time for taking the drugs;
When the supply of drugs is not always available;
When the drugs are of poor quality.

Who is at risk for getting MDR TB?
People who Are irregular in taking medicines
Do not take all of their TB medicine as told by their doctor or nurse
Relapse
Come from areas of the world where drug-resistant TB is common
Have been exposed to DR TB

Extensively drug resistant TB-XDRTB
DEFINITION: TB showing resistance to INH, Rifampicin, and any fluroquinoline, and at least one of the three injectable drugs used in Anti TB treatment: Capriomycin, Kanamycin and Amikacin

Link between TB and HIV HIV co-infection strongest known risk factor for
the progression of latent TB infection
Conversely, TB is amongst the most common causes of morbidity and mortality in people living with HIV/AIDS
Immune response to TB bacilli increases HIV replication leading to a rapid progression of HIV disease
Optimal access to DOTS will significantly reduce morbidity and mortality in PLWHA

Treatment of TB in HIV TB can be successfully treated even in HIV-infected patients
But, cannot alone prevent people from dying of AIDS In addition to TB treatment, ART and CPT needed for those eligible
DOTS is the treatment of choice
Intermittent SCC is effective National policy is to provide RNTCP Cat-I to new cases and Cat-II to
re-treatment cases
Higher relapse rates have been observed especially in those treated with non-Rifampicin containing regimen Whether true relapse or re-infection?
Drug interactions between Rifampicin and ARVs National policy is to start ART after completing anti-TB treatment, or
modify ART by replacing Nevirapine with Efavirenz for the duration of TB treatment

What is New in RNTCP, effective April 2009
EARLIER NOW
3 weeks cough 2 weeks cough
3 sputum specimens required
2 sputum specimens
At least 2specimens should be positive
1 positive is enough

Category 3 is phased out
Ethambutol is reintroduced and dose is @ 20mg/KG
PPM – Public Private Mix

Public-Private share in national health programs

Scheme for treatment adherence
All private practitioners involved as DOTS
Centres
Private practitioner provides DOT services to TB
Patients
PP has to undergo 4 hours of intensive training
in Training Module for Medical Practitioners

DMC in Thrissur District
Doctors’ Laboratory, Chelakara
St. James Hospital, Chalakudy
Modern Laboratory, Kodungallur
Co Operative Hospital, Irinjalakuda

New in RNTCP Cont…
Reference Laboratory is set up for high quality culture and sensitivity tests
Vigilance for MDRTB
For TBM, Inj SM is substituted for Ethambutol in IP
NTP should record and report two age groups for children (0-4 yrs and 5-14yrs)