Embed Size (px)
Citation preview
Lê Bá Hứa
1. Hiểu được cơ chế điều hòa CH muối nước và cơ chế RLCH muối nước trong các dạng mất nước hoặc ứ nước thường gặp.
2. Phân tích được các cơ chế gây phù thủng.
3. Biết được nguyên nhân và hậu quả của RL nước và điện giải.
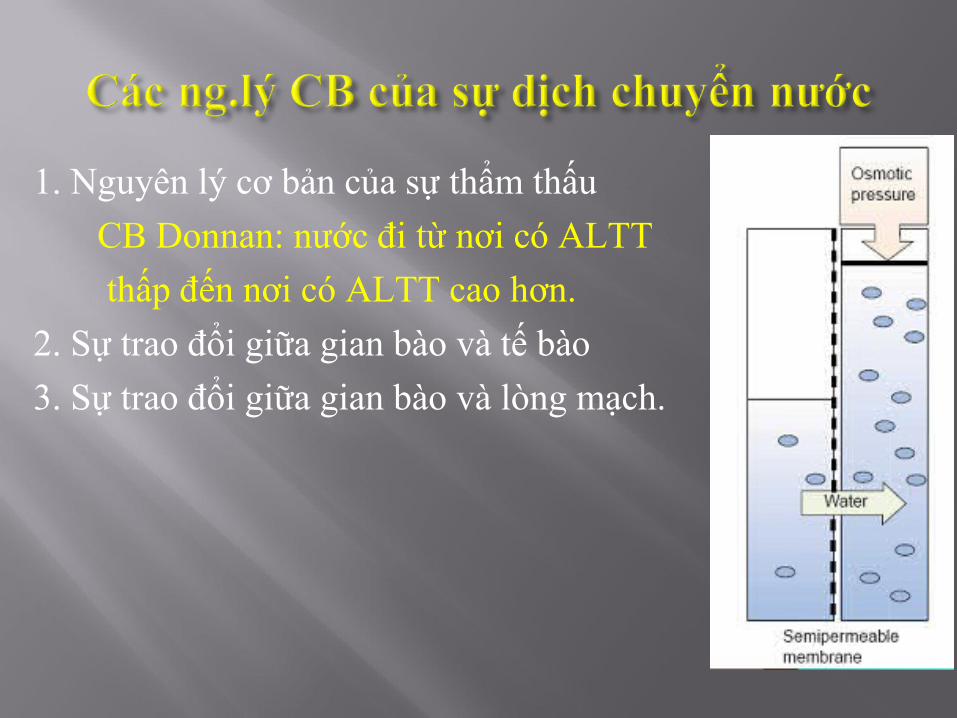
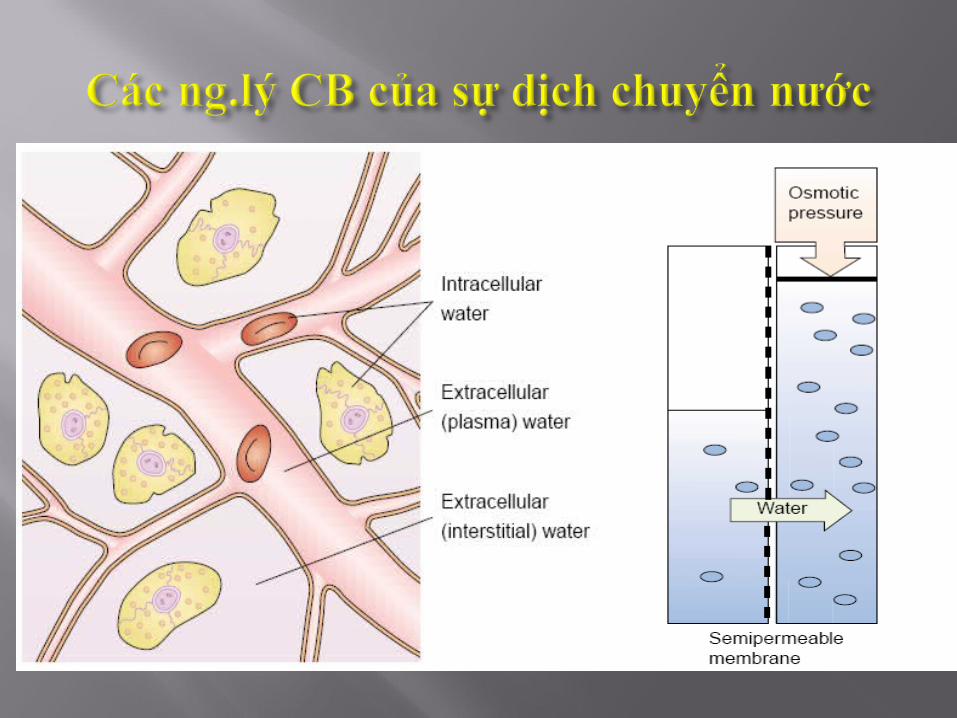
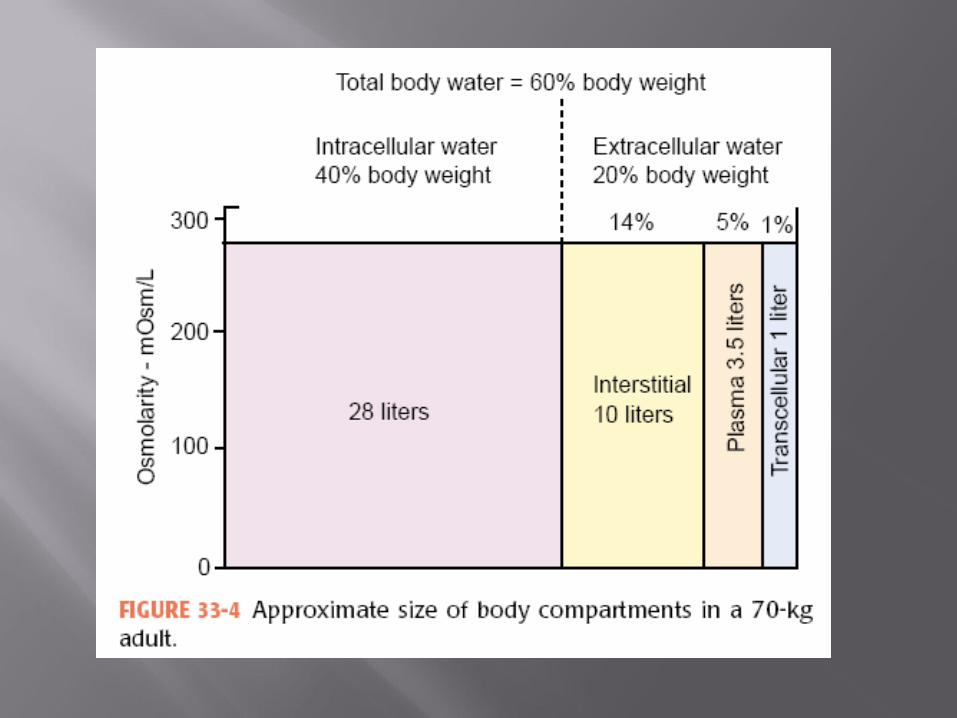
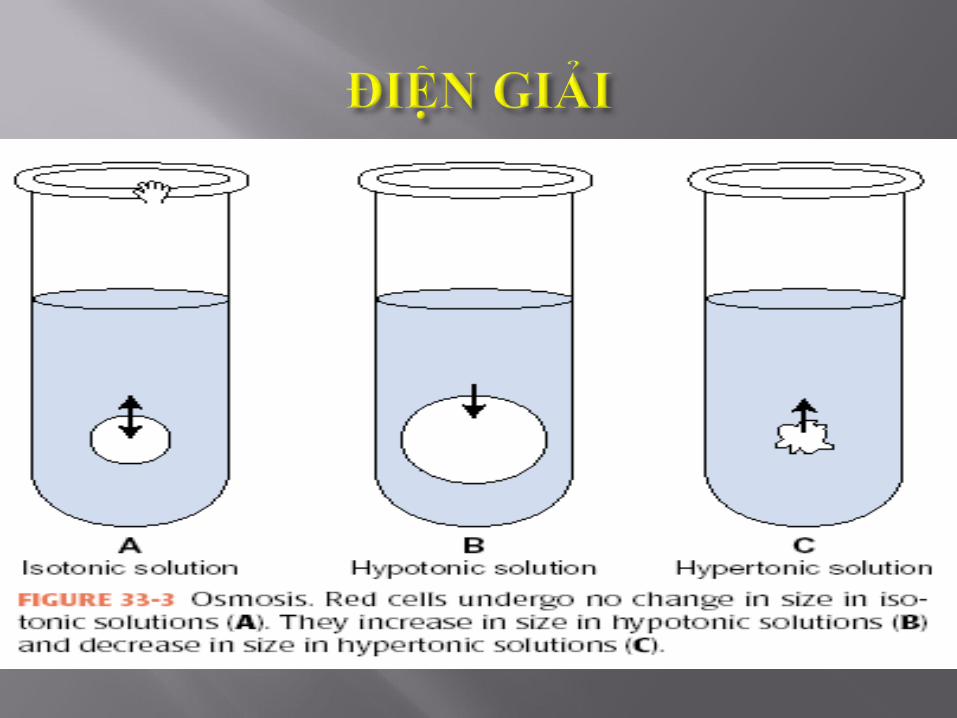
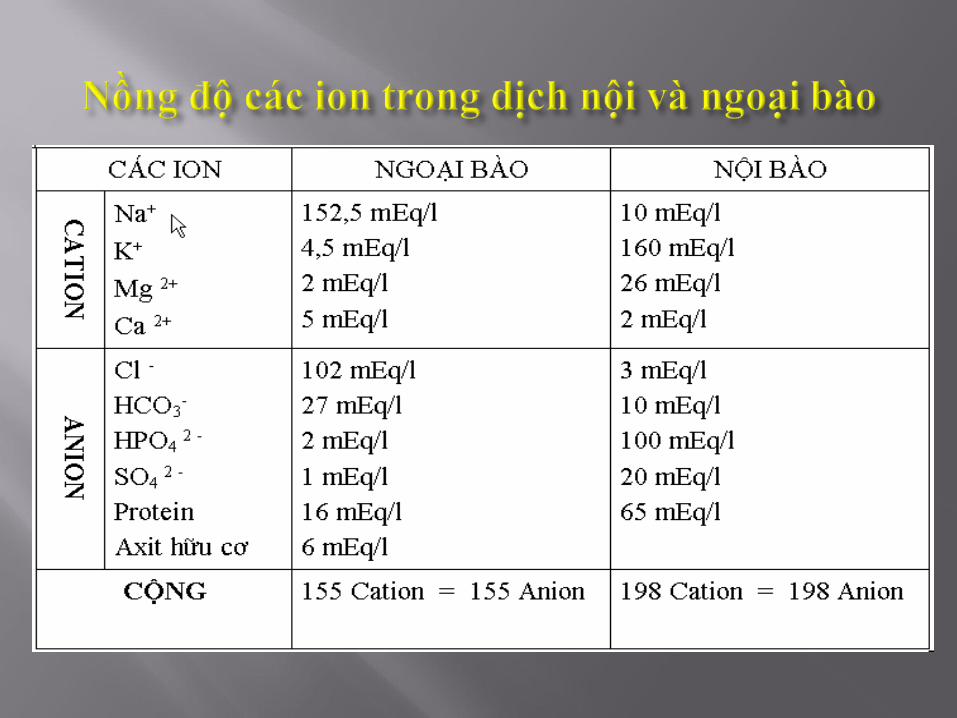
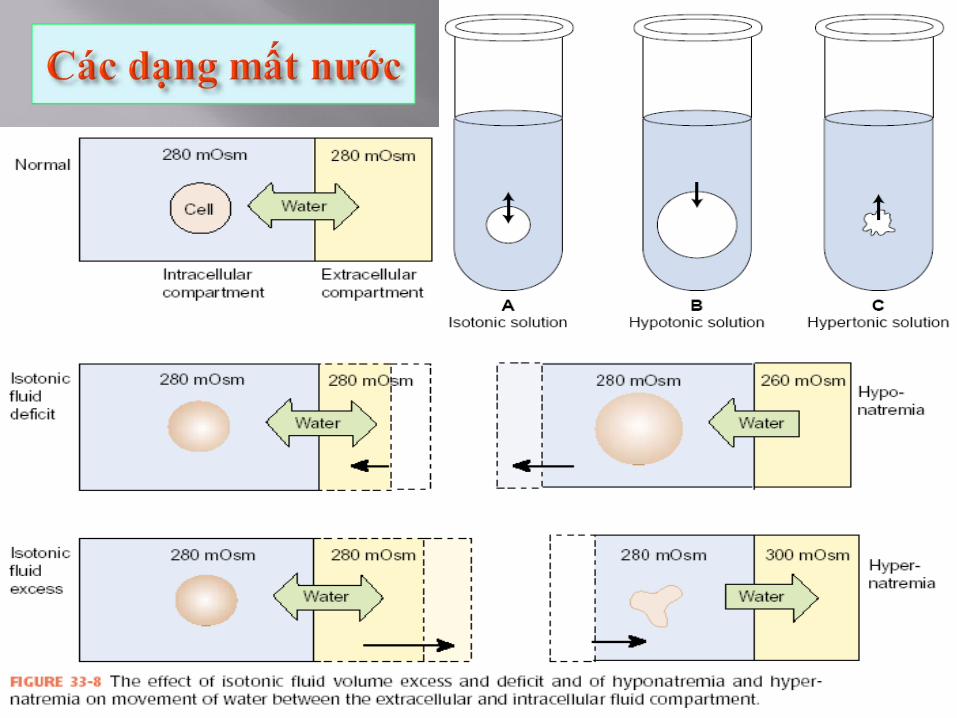
1. Nguyên lý cơ bản của sự thẩm thấu
CB Donnan: nước đi từ nơi có ALTT
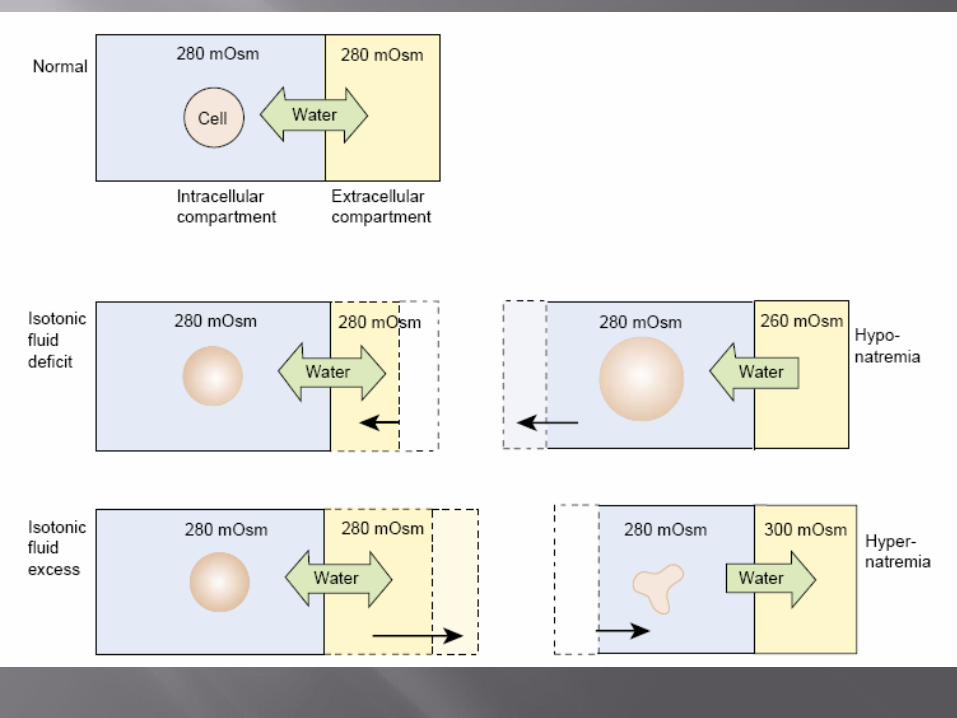
thấp đến nơi có ALTT cao hơn. 2. Sự trao đổi giữa gian bào và tế bào
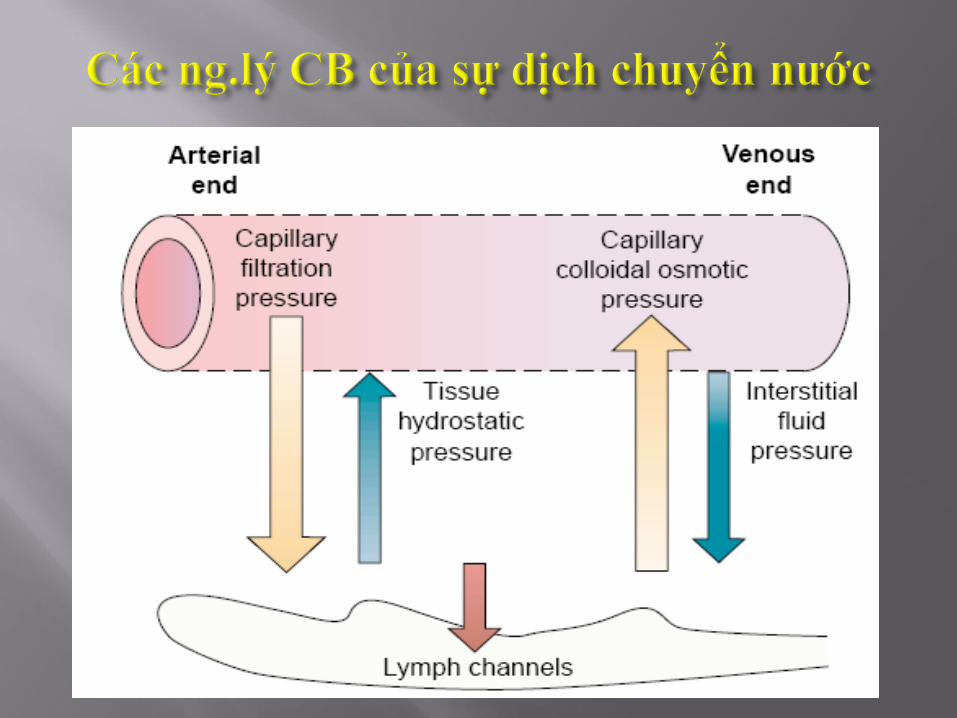
3. Sự trao đổi giữa gian bào và lòng mạch.
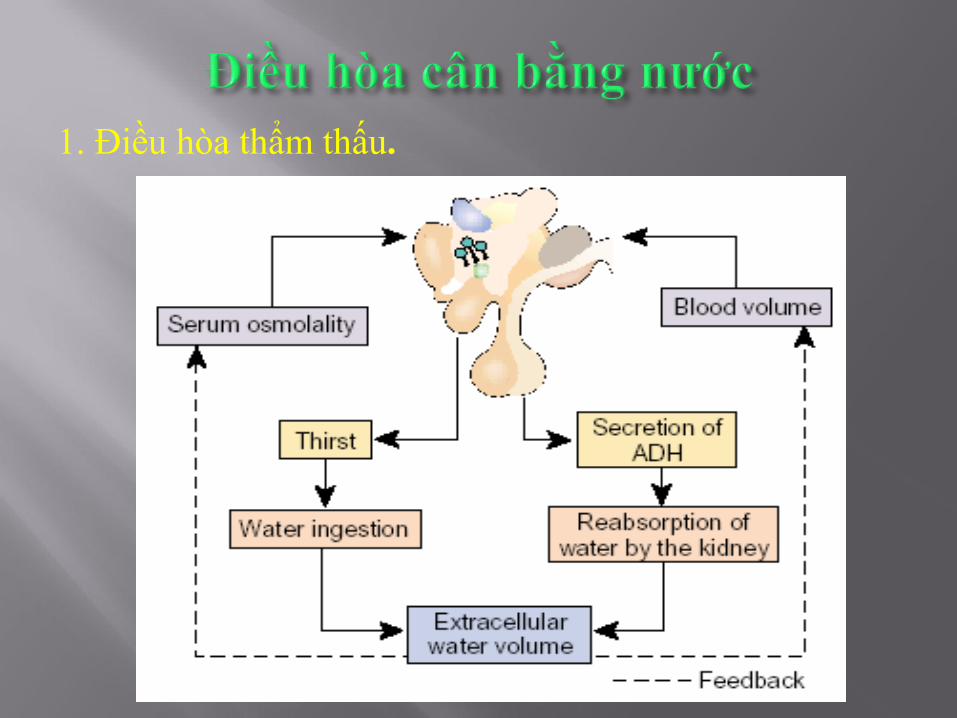
1. Điều hòa thẩm thấu.
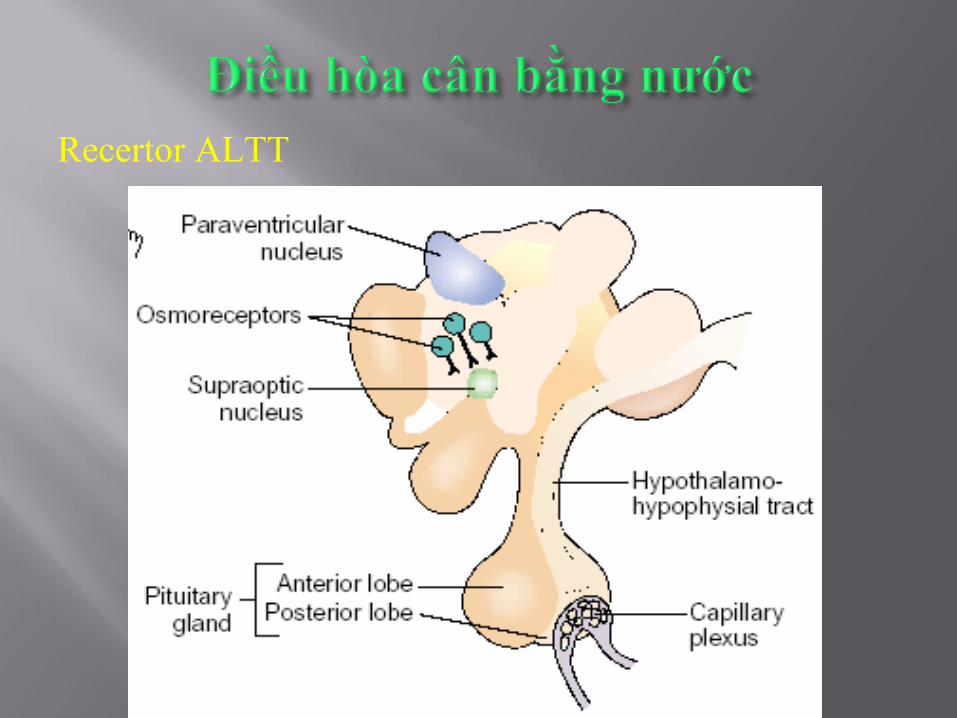
Recertor ALTT
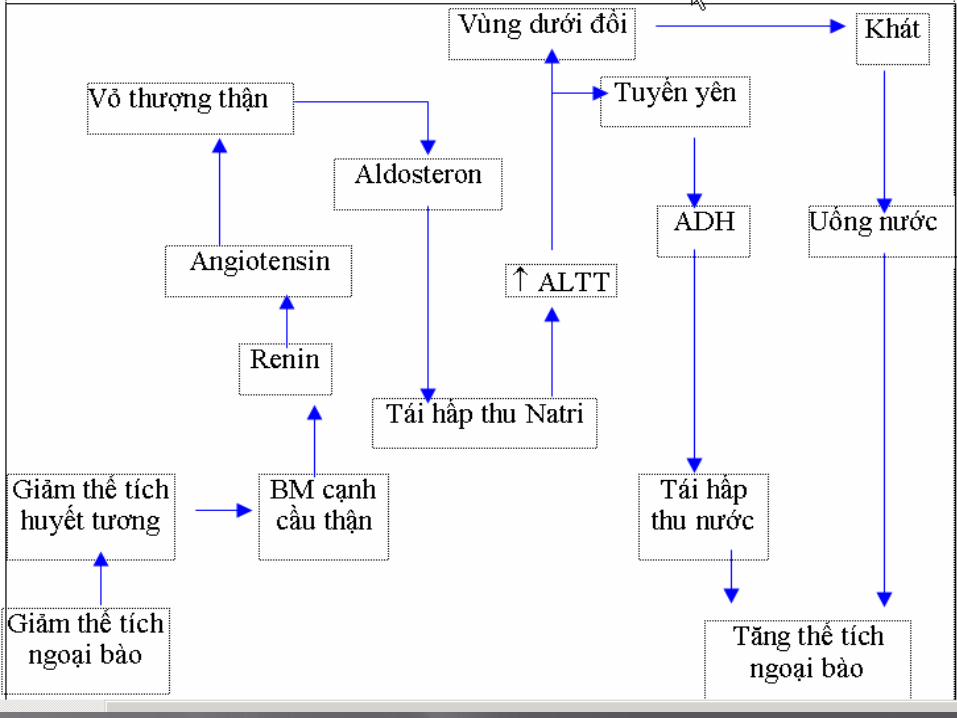
2. Điều hòa thể tích:- Receptor nhận cảm áp lực tại thận
hthống RAA - Receptor nhận cảm áp lực tại tiểu nhĩ
ANP (atrial natriuretic peptide):
Tăng thải Natri qua OT, lợi tiểu do ức chế sự bài tiết ADH và Ald (Ackermann, 1986).
- Receptor áp lực ở khu vực TM ngực và xoang cảnh
Từ R qua đường TK gây tiết ADH.
3. Cơ chế điều khiển ngược Macula- Densa của thận
1. Hẹp ĐM thận và tăng trương lực mm thận
2. Hội chứng tăng Aldosteron
- nguyên phát (hội chứng Conn)
- thứ phát: Xơ gan( giảm giáng hóa Aldosteron), thận hư, suy tim..., tăng renin trong u thượng thận hoặc hội chứng Bartter
3. Thiếu hụt aldosteron
- nguyên phát ( Bệnh Addison)
- thứ phát (thiếu hụt ACTH từ tuyến yên)
4. Đái tháo nhạt (DI: diabetes insipidus).
+ trung ương (CDI : central DI). giảm tiết ADH.
+ do thận (RDI : renal DI). Do R của TBOT kém nhạy cảm với ADH
+ Phân biệt: uống 10 µg Desmopressine
1. Định nghĩa - Phù.- Thủng.
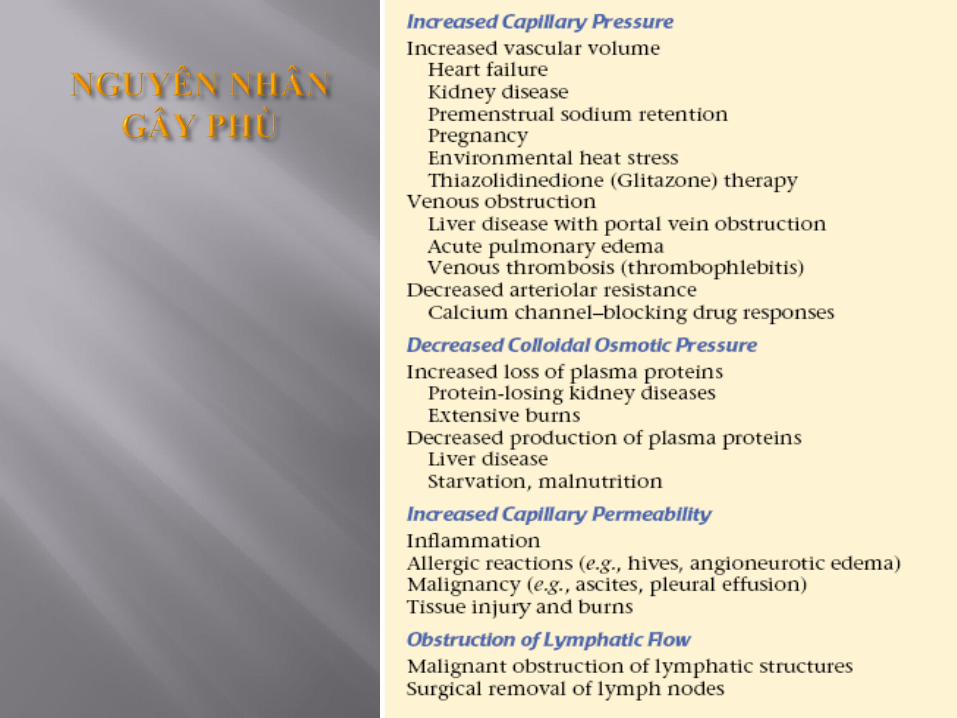
2. Các cơ chế chính gây phù - Tăng áp lực thẩm thấu ngoại bào - Tăng áp lực thủy tĩnh- Giảm áp lực thẩm thấu keo- Tăng tính thấm thành mạch- Cản trở tuần hoàn bạch huyết
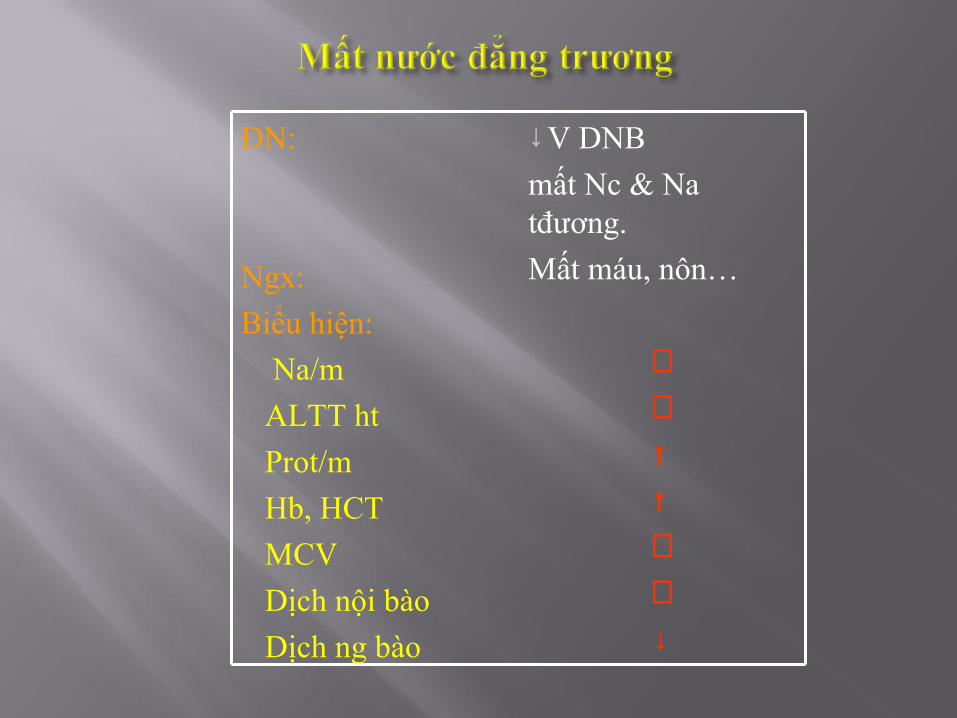
ĐN:
Ngx:
Biểu hiện:
Na/m
ALTT ht
Prot/m
Hb, HCT
MCV
Dịch nội bào
Dịch ng bào
↓V DNB
mất Nc & Na tđương.
Mất máu, nôn…
⊥⊥↑↑⊥⊥↓
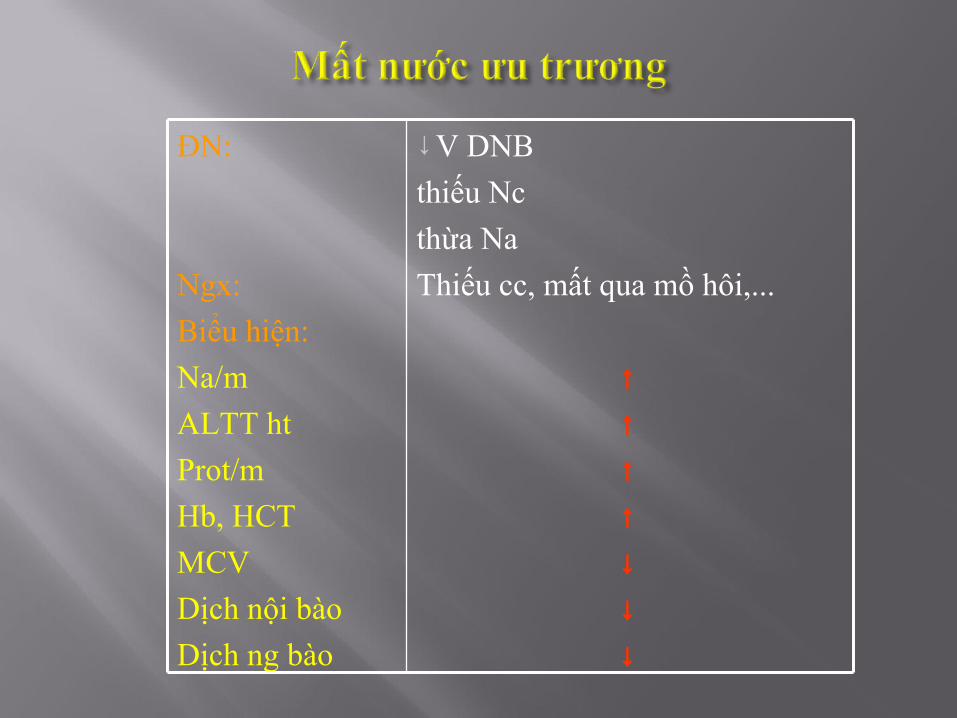
ĐN:
Ngx:
Biểu hiện:
Na/m
ALTT ht
Prot/m
Hb, HCT
MCV
Dịch nội bào
Dịch ng bào
↓V DNB
thiếu Nc
thừa Na
Thiếu cc, mất qua mồ hôi,...
↑↑↑↑↓↓↓
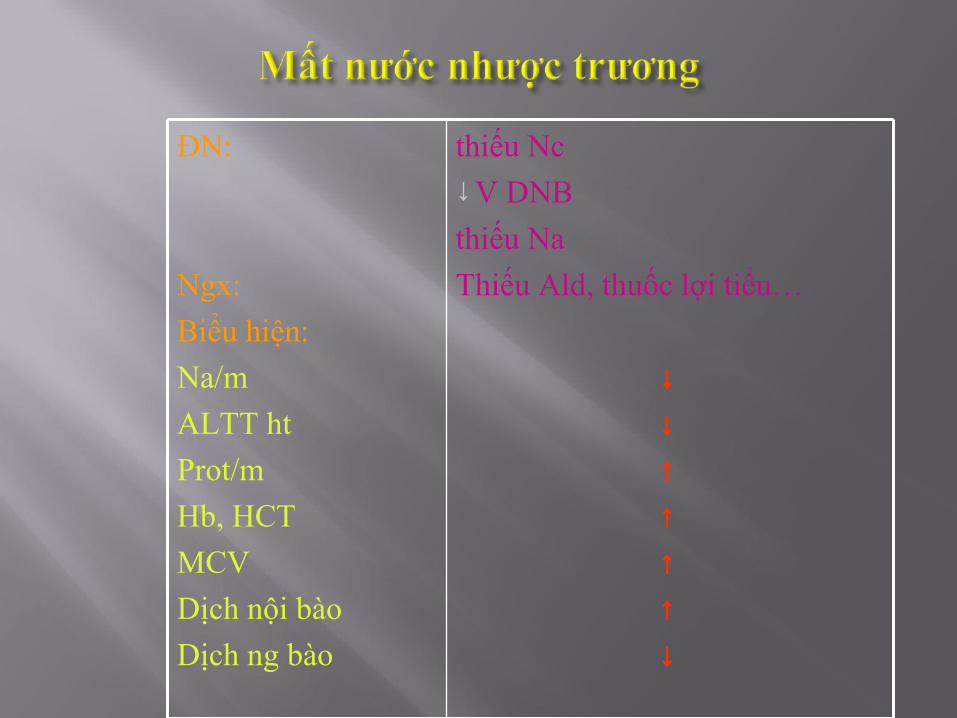
ĐN:
Ngx:
Biểu hiện:
Na/m
ALTT ht
Prot/m
Hb, HCT
MCV
Dịch nội bào
Dịch ng bào
thiếu Nc ↓V DNB
thiếu Na
Thiếu Ald, thuốc lợi tiểu…
↓↓↑↑↑↑↓

MẤT NƯỚC Đẳng trương Ưu trương Nhược trương
ĐN:
Ngx:
Biểu hiện:
Na/m
ALTT ht
Prot/m
Hb, HCT
MCV
Dịch nội bào
Dịch ng bào
↓V DNB
mất Nc & Na tđương.
Mất máu, nôn…
⊥⊥↑↑⊥⊥↓
↓V DNB
thiếu Nc
thừa Na
Thiếu cc, mất qua mồ hôi,...
↑↑↑↑↓↓↓
↓V DNB
thiếu Nc
thiếu Na
Thiếu Ald, thuốc lợi tiểu…
↓↓↑↑↑↑↓
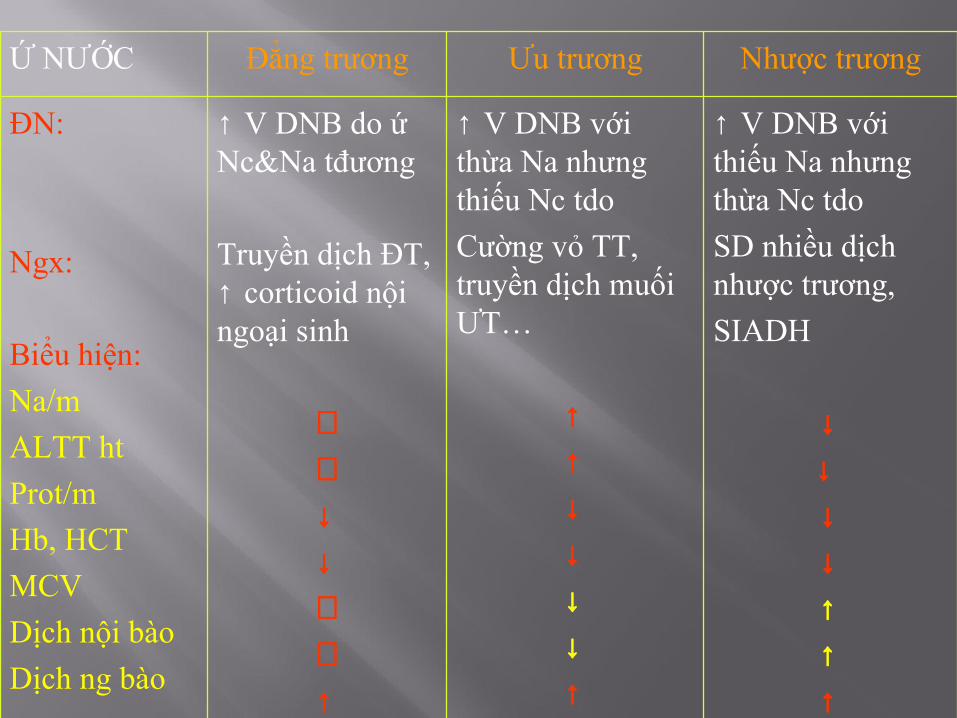
Ứ NƯỚC Đẳng trương Ưu trương Nhược trương
ĐN:
Ngx:
Biểu hiện:
Na/m
ALTT ht
Prot/m
Hb, HCT
MCV
Dịch nội bào
Dịch ng bào
↑ V DNB do ứ Nc&Na tđương
Truyền dịch ĐT, ↑ corticoid nội ngoại sinh
⊥⊥↓↓⊥⊥↑
↑ V DNB với thừa Na nhưng thiếu Nc tdo
Cường vỏ TT, truyền dịch muối ƯT…
↑↑↓↓↓↓↑
↑ V DNB với thiếu Na nhưng thừa Nc tdo
SD nhiều dịch nhược trương,
SIADH
↓↓
↓↓↑↑↑
SIADH results from a failure of the negative feedback system that regulates the release and inhibition of ADH.
In persons with this syndrome, ADH secretion continues even when serum osmolality is decreased; this causes marked retention of water in excess of sodium and dilutional hyponatremia. An increase in the glomerular
filtration rate resulting from an increased plasma volumecauses further increases in sodium loss by suppressing therenin-angiotensin mechanism. Urine osmolality is high,and serum osmolality is low.
(1) hypotonic hyponatremia,
(2) natriuresis,
(3) urine osmolality in excess of plasma osmolality,
(4) absence of edema and volume depletion, and
(5) normal renal and adrenal function.20
SIADH can be caused by a number of conditions; however, the major causes are neoplasia, neurologic diseases, lung diseases, and a variety of pharmacologic agents. Tumors, particularly bronchogenic carcinomas and cancers of the lymphoid tissue, prostate, and pancreas, are known to produce and release ADH independent of normal hypothalamic control mechanisms. Other intrathoracic conditions, such as advanced tuberculosis, severe pneumonia, and positive-pressure breathing, also cause SIADH. The suggested mechanism for SIADH in positive-pressure ventilation is
activation of baroreceptors (e.g., aortic baroreceptors, cardiopulmonary receptors) that respond to marked changes in intrathoracic pressure.
the major causes are neoplasia, neurologic diseases, lung diseases, and a variety of pharmacologic agents.
Tumors, particularly bronchogenic carcinomas and cancers of the lymphoid tissue, prostate, and pancreas, are known to produce and release ADH independent of normal hypothalamic control mechanisms. Other intrathoracic conditions, such as advanced tuberculosis, severe pneumonia, and positive-pressure breathing, also cause SIADH. The suggested mechanism for SIADH in positive-pressure ventilation
is activation of baroreceptors (e.g., aortic baroreceptors, cardiopulmonary receptors) that respond to marked changes in
intrathoracic pressure.
Disease and injury to the central nervous system (CNS) can cause direct pressure on or direct involvement of the hypothalamic–posterior pituitary structures.
Examples include brain tumors, hydrocephalus, headinjury, meningitis, and encephalitis. Other stimuli, suchas surgery, pain, stress, and temperature changes, are
capable of stimulating ADH release through the limbic system.
Human immunode.ciency virus infection is frequently associated with SIADH. It has been reported that up to 35% of persons with acquired immunode.ciencsyndrome
who are admitted to the acute care setting have SIADH related to Pneumocystis carinii pneumonia, CNS infections, or malignancies.
The manifestations of SIADH are those of dilutional hyponatremia. The
severity of symptoms usually is proportional to the extent
of sodium depletion and water intoxication.
The treatment of SIADH depends on its severity. In mild cases, treatment consists of .uid restriction. If .uid restriction is not suf.cient, diuretics such as mannitol and furosemide (Lasix) may be given to promote diuresis and free-water clearance. Lithium and the antibiotic demeclocycline inhibit the action of ADH on the renal collecting ducts and sometimes are used in treating the disorder. In cases of severe water intoxication, a hypertonic (e.g., 3%) sodium chloride solution may be administered intravenously. New antagonists to the antidiuretic action of ADH (aquaretics) offer a new therapeutic approach.20
Drugs induce SIADH in different ways; some drugs are thought to increase hypothalamic production and release,and others are believed to act directly on the renal tubules to enhance the action of ADH.
SIADH may occur as a transient condition, as in a stress situation, or as a chronic condition, resulting from disorders such as lung tumors.





























