Embed Size (px)
DESCRIPTION
Palmieri, P. A., & Peterson, L. T. (2009). Safety culture as a healthcare construct. Presented at the Annual Meeting of the Academy of Management (August 9): Chicago, Illinois, USA. Nominated for Best Paper Award, Healthcare Management Division.
Citation preview

Safety Culture as a
Healthcare Construct
Patrick A. Palmieri Center for American Education
Lori T. Peterson Nance College of Business Administration
Presented at the 2009 Annual Meeting of the Academy of
Management, Chicago, Illinois (August 9, 2009).
Best Paper Award Nominee, Health Care Division.

• Patrick Albert Palmieri
– Duke Health Technology Solutions
• Information Technology Fellowship
– Duke University
• Doctoral Scholarship
– National Institutes of Health (NIH)
• Roadmap for Medical Research, (Individual T-32 Summer
Research Award). Project: Organizational Safety Culture Survey
Reliability and Validity (Palmieri, PI). Duke University Clinical
and Translational Science Institute (Califf, PI).
• Lori T. Peterson
– Texas Tech University Rawls College of Business
• Center for Health Innovation, Education, and Research
Funding Sources for Our Work

Paper Aims
• Analyze the theoretical underpinnings of safety
culture
• Examine the psychometric performance
properties of the measurement instruments
• Provide an assessment about the state of safety
culture research in healthcare

Presentation Aims
• Summarize the state of healthcare to support the
need for safety culture research
• Identify the disciplinary origination (theoretical
influences) for the safety culture concept
• Describe the contemporary safety culture
framework
• Discuss the findings from our review
• Recommend aims and goals for future safety
culture work

INTRODUCTION

“It may seem a strange principle
to enunciate as the very first
requirement in a hospital that it
should do the sick no harm”
Florence Nightingale, 1863, Notes on Hospitals

Healthcare is Dangerous
• Flawed systems (e.g. Zhan & Miller, 2003)
• Faulty processes (e.g. Reason, Carthey, & de Leval, 2001)
• Poor interactions (e.g. Cook, Render, & Woods, 2000)
• Substandard performance (e.g. Benner et al. 2006)
• Inadequate training (e.g. Bohmer & Edmondson, 2001)
• Poor management practices (e.g. Konteh et al., 2008)
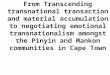
Anatomy and Physiology of Error in Adverse Healthcare Events
Palmieri, DeLucia, Peterson, Ott, & Green (2008)

Safety Culture Focus
• Institute of Medicine recommends that
healthcare organizations:
– Develop safety cultures
– Routinely assess safety culture
– Establish comprehensive patient safety plans to
improve error detection
– Reduce opportunities for error by redesigning
care systems
IOM, 2000, 2004a, 2004b

Definition of Safety Culture
• A global organizational property that can be
defined as:
The organizational inputs of individual
and group attitudes, perceptions, and
values about workplace behaviors and
system processes that collectively
contribute to safe and reliable
organizational outputs. (Cox and Flin 1998 and others)

THEORETICAL INFLUENCES

Theoretical Influences
• Sociology
– Normal Accident Theory
• Psychology
– High Reliability Theory
• Human Factors and Ergonomics (HF/E)
– Aviation Framework

Sociology
• Safety is an emergent property of culture (Smirich 1983)
– Reflect the collective history of individual
contributions to group (Perrow 1970)
• Culture is not easily changed (Perrow & Langton, 1994;
Sagan, 1994)
• Resistant to direct management intervention (Mears & Flin, 1999)
• Safety linked to reduced complexity &
coupling
– Inflexible policies and procedures, and poorly
designed processes and systems (Perrow, 1999)

Psychology
Similar to Sociology except:
• Cultures readily change
– Exist for the purpose of manipulation (Schein, 1991)
• Individual focused
– “Collective mindfulness” of employees (Weick &
Roberts, 1993; Weick & Sutcliffe, 2006)
• Management practices and interventions

Human Factors & Ergonomics
• Emphasis on application not theory
production
• Derived from deductive methodologies
– Critical incident (Flanagan, 1954; Woods & Chattuck, 2000)
– Critical decision (Carlisle, 1986)
Note: Aviation research related to behavioral markers
is incomplete, early in development, and not
psychometrically validated (Yule at al., 2006)

CONSTRUCTS &
FRAMEWORK

Research Assumptions
Four assumptions guide the majority of safety
culture research:
1. Safety focused cultures produce better outcomes
2. Improved safety performance are produced by
positive safety cultures
3. Organizations can improve culture by making
safety a priority
4. Management practices influence employee safety
performance

Safety Culture Characteristics
• Four cultural characteristics permit the
organization of work to support safety
1. Learning
2. Reporting
3. Justice and Fairness
4. Flexibility (e.g. Reason, 1998b)

Safety Culture Framework
• Frameworks and models undefined
– No arrows, no lines connecting boxes
• Possible antecedents
– Error reporting (Piotrowski & Hinshaw, 2002)
– Non-punitive climate (Dekker, 2007)
– Trust (Dirks & Ferrin, 2002)
– Management involvement and practices (Thomas et al.,
2005; Wong, Helsinger, & Petry, 2002)
– System and processes perspective (Barach & Johnson, 2006)

FINDINGS

Basic Conceptual Issues
• Unsystematic, fragmented, and “underspecified in
theoretical terms” (Pidgeon ,1998; Zhan et al., 2002)
• Considerable disagreement among safety experts
about the definition of safety culture and how this
is operationalized (Flin et al., 2000; Guldenmund, 2000; Hale, 2000;
Wiegmann et al., 2004)
– Culture & climate terms often used interchangeably (e.g. Cox and Flin, 1998, Colla et al., 2005)
• Safety culture research provides management
with data for benchmarking and trends analysis (Mearns, Flin, & Whitaker, 2001)

“The applicability of safety culture as
a universal concept across disciplines
and specialties within healthcare as
well as the relationship to specific
safety performance measures
remains questionable and unsettled .”
Flin et al., 2006
Healthcare Safety Culture

RECOMMENDATIONS

“Only the lack of theoretical
grounding, scarcity of conceptual
framework, and the presence of a
dimension related to leadership and
management practices was common
across the reviews.”
Theoretical Framework
e.g. Flin et al., 2000; Guldenmund, 2000;
Colla et al., 2005; Scott et al., 2003a

“Merely developing more
measurement scales and re-testing
climate-behavior relationships will
hold back scientific progress.”
Zohar, 2008
Measurement Instruments

Research Methods
Measuring individual perceptions within
studies designed to analyze data at the
group or organizational level is
“theoretically incompatible”
Hoffman & Stetzer, 1996; Zohar, 2003

Psychometric Properties
The science is limited by the
inadequate attention to establishing
suitable psychometric properties, such
as reporting essential validity and
reliability standards
Colla et al., 2005; Flin et al., 2006; Flin, 2007

Conclusion
Safety culture “is a concept whose time has come”
and we should “develop a clearer theoretical
understanding of these organizational issues to
create a principled basis for more effective culture-
enhancing practices”. Reason (1998b)
We agree…
but we also believe… Inadequate theoretical frameworks and the
associated instrument and methodological issues limit
further development as a translational science where
interventions might be designed, implemented, and
tested as methods to improve outcomes.

Contact Information
Patrick A. Palmieri
Lori A. Peterson
CITATION: Palmieri, P. A., & Peterson, L. T. (2009). Safety culture as a
healthcare construct. Presented at the Annual Meeting of the Academy of
Management (August 9): Chicago, Illinois, USA.