Embed Size (px)
DESCRIPTION
Citation preview

A hormone is a chemical substance produced in the body by an organ, cells of an organ, or scattered cells, having a specifi c regulatory eff ect on the activity of
an organ or organs. 15 Hormones are produced at one site in the body and exert their action(s) at distant sites through what is called the endocrine system. It is increasingly recog-nized that many hormones exert actions locally through what is termed the paracrine system. Finally, some hormones exert their action on the cells of origin, regulating their own syn-thesis and secretion via an autocrine system. Th e classic endo-crine hormones include insulin, thyroxine, and cortisol. Neurotransmitters and neurohormones are examples of the paracrine system, and certain growth factors that stimulate synthesis and secretion of true hormones from the same cell are examples of an autocrine system.
Table 29-1 lists hormones that are commonly measured in clinical practice plus a few others to illustrate concepts. Biochemical, clinical, and analytical information for specifi c hormones may be found in Chapters 26 and 46 through 57 .
CLASSIFICATION Hormones are classifi ed as (1) polypeptides or proteins, (2) steroids, or (3) derivatives of amino acids.
Polypeptide or Protein Hormones Adrenocorticotropic hormone (ACTH), insulin, and para-thyroid hormone (PTH) are examples of polypeptide or protein hormones. Th ey are generally water soluble and cir-culate freely in plasma as the whole molecule or as active or inactive fragments. Th e half-life of these hormones in plasma is short ( ≤ 10 to 30 minutes), and wide fl uctuations in their concentration may be seen in several physiologic and patho-logic circumstances. Th ese hormones initiate their response by binding to cell membrane receptors (on or in the mem-brane) and exciting a “ second messenger ” system, which con-tinues the specifi c actions of these hormones.
Steroid Hormones Steroid hormones (e.g., cortisol, estrogen) are hydrophobic and insoluble in water. Th ese hormones circulate in plasma,
reversibly bound to transport proteins (e.g., cortisol-binding globulin, sex hormone-binding globulin) with only a small fraction free, or unbound available to exert physiologic action. 5,8,17 Th e half-life of steroid hormones is 30 to 90 minutes. Free steroid hormones, being hydrophobic, enter the cell by passive diff usion and bind with intracellular recep-tors in the cytoplasm or the nucleus. 3
Amino Acid – Related Hormones Th yroxine and catecholamine are examples of hormones that are derived from amino acids; they are water soluble and cir-culate in plasma bound to proteins (thyroxine) or free (cate-cholamines). Th yroxine binds avidly to three binding proteins and has a half-life of about 7 to 10 days; free and unbound catecholamines such as epinephrine have a very short half-life of a minute or less. As do the water-soluble peptide and protein hormones, these hormones interact with membrane-associated receptors and use a second messenger system.
RELEASE AND ACTION OF HORMONES Th e physiologic functions of hormones have been broadly categorized into those that (1) aff ect growth and develop-ment, (2) exert homeostatic control of metabolic pathways, and (3) regulate the production, use, and storage of energy. Th e descriptions that follow illustrate examples of these func-tions and mechanisms of control of hormone secretion.
Growth and Development Normal growth and development of the whole human organ-ism is dependent on the complex integrative function of many hormones, including gonadal steroids (estrogen and androgen), growth hormone, cortisol, and thyroxine. Several pituitary hormones are responsible specifi cally for the growth and development of endocrine glands themselves, and thus are responsible for control of synthesis and secretion of other hormones. Th ose other hormones can provide negative feed-back on secretion of the pituitary hormones. Other regulators of secretion of the pituitary hormones include circadian rhythms and a hypothalamic pulse generator that controls the
CHAPTER 29
837
Hormones Michael Kleerekoper , M.D., F.A.C.B.,
F.A.C.P., M.A.C.E. *
* Th e author gratefully acknowledges the original contribution by Dr. Ronald J. Whitley on which portions of this chapter are based.
Text continued on page 842

838 Section III ■ Analytes
TABLE 29-1 Major Hormones and Frequently Measured Hormone Precursors and Cytokines
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Hypothalamus Th yrotropin-releasing hormone
(TRH)Peptide (3aa, Glu-His-
Pro) a Anterior pituitary Release of TSH and prolactin (PRL)
Gonadotropin-releasing hormone (Gn-RH) or luteinizing hormone- releasing hormone (LH-RH)
Peptide (10aa) Anterior pituitary Release of LH and FSH
Corticotropin-releasing hormone (CRH)
Peptide (41aa) Anterior pituitary Release of ACTH and β -lipotropic hormone (LPH)
Growth hormone-releasing hormone (GH-RH)
Peptides (40, 44aa) Anterior pituitary Release of growth hormone (GH)
Somatostatin b (SS) or growth hormone-inhibiting hormone (GH-IH)
Peptides (14, 28aa) Anterior pituitary Suppression of secretion of many hormones [e.g., GH, TSH, gastrin, vasoactive intestinal polypeptide (VIP), gastric inhibitory polypeptide (GIP), secretin, motilin, glucagon, and insulin]
Prolactin-releasing peptide Peptide (20aa) Anterior pituitary Release of PRLProlactin-releasing/inhibiting
factorDopamine Anterior pituitary Suppression of synthesis and
secretion of PRL
Anterior Pituitary Lobe Th yrotropin or thyroid-
stimulating hormone (TSH)Glycoprotein,
heterodimer c ( α , 92aa; β , 112aa)
Th yroid gland Stimulation of thyroid hormone formation and secretion
Follicle-stimulating hormone (FSH)
Glycoprotein, heterodimer c ( α , 92aa; β , 117aa)
Ovary Growth of follicles with LH, secretion of estrogens, and ovulation
Testis Development of seminiferous tubules; spermatogenesis
Luteinizing hormone (LH) Glycoprotein, heterodimer c ( α , 92aa; β , 121aa)
Ovary Ovulation; formation of corpora lutea; secretion of progesterone
Testis Stimulation of interstitial tissue; secretion of androgens
PRL Peptide (199aa) Mammary gland Proliferation of mammary gland; initiation of milk secretion; antagonist of insulin action
Growth hormone (GH) or somatotropin
Peptide (191aa) Liver Production of IGF-1 (promoting growth)
Liver and peripheral tissues
Anti-insulin and anabolic eff ects
Corticotropin or adrenocorticotropin (ACTH)
Peptide (39aa) Adrenal cortex Stimulation of adrenocortical steroid formation and secretion
β -Endorphin ( β -END) b,h Peptide (31aa) Brain Endogenous opiate; raising of pain threshold and infl uence on extrapyramidal motor activity
Chorionic gonadotropin (CG) or choriogonadotropin
Glycoprotein, heterodimer c ( α , 92aa; β , 145aa)
α -Melanocyte-stimulating hormone ( α -MSH)
Peptide (13aa) Skin Dispersion of pigment granules, darkening of skin
Leu-enkephalin (LEK) b,h and met-enkephalin (MEK) b,h
Peptide (5aa) Brain Same as β -endorphin

Chapter 29 ■ Hormones 839
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Posterior Pituitary Lobe Vasopressin or ADH Peptide (9aa) Arterioles
Renal tubulesElevation of blood pressure; water
reabsorptionOxytocin Peptide (9aa) Smooth muscles
(uterus, mammary gland)
Contraction; action in parturition and in sperm transport; ejection of milk
Pineal Gland Serotonin or
5-hydroxytryptamine (5-HT)Indoleamine Cardiovascular,
respiratory, and gastrointestinal systems; brain
Neurotransmitter; stimulation or inhibition of various smooth muscles and nerves
Melatonin Indoleamine Hypothalamus Suppression of gonadotropin and GH secretion; induction of sleep
Th yroid Gland Th yroxine (T 4 ) and
triiodothyronine (T 3 )Iodoamino acids General body tissue Stimulation of oxygen consumption
and metabolic rate of tissueCalcitonin or thyrocalcitonin Peptide (32aa) Skeleton Uncertain in humans
Parathyroid Gland Parathyroid hormone (PTH) or
parathyrinPeptide (84aa) Kidney Increased calcium reabsorption,
inhibited phosphate reabsorption; increased production of 1,25- dihydroxycholecalciferol
Skeleton Increased bone resorption
Adrenal Cortex Aldosterone Steroid Kidney Salt and water balanceAndrostenedione d Steroid Hormone precursor Converted to estrogens and
testosteroneCortisol Steroid Many Metabolism of carbohydrates,
proteins, and fats; anti-infl ammatory eff ects; others
Dehydroepiandrosterone (DHEA) and dehydroepiandrostenedione sulfate (DHEAS)
Steroids Hormone precursors Converted to estrogens and testosterone
17-Hydroxyprogesterone Steroid Hormone precursor Converted to cortisol
Adrenal Medulla Norepinephrine and
epinephrineAromatic amines Sympathetic
receptorsStimulation of sympathetic nervous
systemEpinephrine Liver and muscle,
adipose tissueGlycogenolysis Lipolysis
Ovary Activin A Peptides e
2 β A subunitsPituitary, ovarian
follicleStimulates release of FSH; enhances
FSH action; inhibits androgen production by theca cells
Activin B Peptides e 2 β B subunits beta
See activin A above See activin A above
DHEA and DHEAS Steroids Hormone precursors Converted to androstenedione
TABLE 29-1 Major Hormones and Frequently Measured Hormone Precursors and Cytokines—cont’d
Continued

840 Section III ■ Analytes
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Estrogens Phenolic steroids Female accessory sex organs
Development of secondary sex characteristics
Bone Control of skeletal maturation et alFollistatin Peptides (288aa,
315aa)Pituitary, ovarian
folliclesInhibits FSH synthesis and secretion
by binding activinInhibin A Peptide ( α subunit
and β A subunit)Hypothalamus,
ovarian follicleInhibits FSH secretion; stimulates
theca cell androgen productionInhibin B Peptide ( α subunit
and β B subunit)See inhibin A above See inhibin A above
Progesterone Steroid Female accessory reproductive structure
Preparation of the uterus for ovum implantation, maintenance of pregnancy
Relaxin Peptide f Uterus Inhibition of myometrial contraction
Testis Inhibin B See above Anterior pituitary,
hypothalamusControl of LH and FSH secretion
Testosterone Steroid Male accessory sex organs
Development of secondary sex characteristics, maturation, and normal function
Placenta Estrogens See above See above See aboveProgesterone See above See above See aboveRelaxin See above See above See aboveChorionic gonadotropin (CG)
or choriogonadotropinGlycoprotein,
heterodimer c ( α , 92aa; β , 145aa)
Same as LH Same as LH; prolongation of corpus luteal function
Placental growth hormone (GH-V)
Peptides (22 and 26 kDa)
Same as GH Same as GH
Chorionic somatomammotropin (CS) or placental lactogen (PL)
Peptide (191aa) Same as PRL Same as PRL
Pancreas Amylin Peptide (37aa) Pancreas Inhibits glucagon and insulin
secretionGlucagon Peptide (29aa) Liver GlycogenolysisInsulin Peptide g Liver, fat, muscle Regulation of carbohydrate
metabolism; lipogenesisPancreatic polypeptide (PP) Peptide (36aa) Gastrointestinal tract Increased gut motility and gastric
emptying; inhibition of gallbladder contraction
Somatostatin (SS) h Peptide (14aa) Pancreas Inhibition of secretion of insulin, glucagon
Gastrointestinal Tract Gastrin h Peptide (17aa) Stomach Secretion of gastric acid, gastric
mucosal growthGhrelin h (GHRP) Peptide (28aa) Anterior pituitary Secretion of GHSecretin Peptide (27aa) Pancreas Secretion of pancreatic bicarbonate
and digestive enzymes
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Ovary—cont’d
TABLE 29-1 Major Hormones and Frequently Measured Hormone Precursors and Cytokines—cont’d

Chapter 29 ■ Hormones 841
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Cholecystokinin-pancreozymin (CCK-PZ) h
Peptide (33aa) Gallbladder and pancreas
Stimulation of gallbladder contraction and secretion of pancreatic enzymes
Motilin Peptide (22aa) Gastrointestinal tract Stimulation of gastrointestinal motility
VIP h Peptide (28aa) Gastrointestinal tract Neurotransmitter; relaxation of smooth muscles of gut and of circulation; increased release of hormones and secretion of water and electrolytes from pancreas and gut
Gastric inhibitory peptide (GIP)
Peptide (42aa) Gastrointestinal tract Inhibition of gastric secretion and motility; increase in insulin secretion
Glucagon-like peptide-1 Peptide (30-31aa) Gastrointestinal tract Increase insulin and decrease glucagon secretion; inhibit gastric emptying
Bombesin h Peptide (14aa) Gastrointestinal tract Stimulation of release of various hormones and pancreatic enzymes, smooth muscle contractions and hypothermia, changes in cardiovascular and renal function
Neurotensin h Peptide (13aa) Gastrointestinal tract and hypothalamus
Uncertain
Substance P (SP) h Peptide (11aa) Gastrointestinal tract and brain
Sensory neurotransmitter, analgesic; increase in contraction of gastrointestinal smooth muscle; potent vasoactive hormone; promotion of salivation, increased release of histamine
Kidney 1,25-(OH) 2 cholecalciferol Sterol Intestine
BoneFacilitation of absorption of calcium
and phosphorus; increase in bone resorption in conjunction with PTH
Kidney Increase in reabsorption of fi ltered calcium
Erythropoietin Peptide (165aa) Bone marrow Stimulation of red cell formationRenin-angiotensin-aldosterone
systemPeptides (renin, 297aa;
Ang I, 10aa; Ang II, 8aa, produced from Ang I by angiotensin converting enzyme)
Renin (from kidney) catalyzes hydrolysis of angiotensinogen (from liver, 485aa) to ang I in the intravascular space
Ang II increases blood pressure and stimulates secretion of aldosterone (see adrenal)
Liver IGF-1, formerly called
somatomedinPeptide (70aa) Most cells Stimulation of cellular and linear
growthIGF-2 Peptide (67aa) Most cells Insulin-like activity
TABLE 29-1 Major Hormones and Frequently Measured Hormone Precursors and Cytokines—cont’d
Continued

842 Section III ■ Analytes
Endocrine Organ and Hormone
Chemical Nature of Hormone
Major Sites of Action Principal Actions
Th ymus Th ymosin and thymopoietin Peptides (28, 49aa) Lymphocytes Maturation of T lymphocytes
Heart Atrial natriuretic peptide (ANP,
Atriopeptin)Peptide with an
intrachain disulfi de bond (28aa)
Vascular, renal, and adrenal tissues
Regulation of blood volume and blood pressure
B-type natriuretic peptide (BNP)
Peptide with an intrachain disulfi de bond (32aa)
Vascular, renal, and adrenal tissues
Regulation of blood volume and blood pressure
Adipose Tissue Adiponectin Peptide oligomers of
30 kDa subunitsMuscle Liver
Increases fatty acid oxidation Suppresses glucose formation
Leptin Peptide (167aa) Hypothalamus Inhibition of appetite, stimulation of metabolism
Resistin Peptide (94aa) Liver Insulin resistance
Multiple Cell Types Estrogens See above See above See aboveGalanin Peptide (30aa) Brain, pancreas,
gastrointestinal (GI) tract
Regulates food intake, memory, and cognition; inhibits endocrine and exocrine secretions of pancreas; delays gastric emptying; prolongs colonic transport times
Parathyroid hormone-related peptide (PTH-RP)
Peptides (139, 141, 173aa)
Kidney, bone Physiologic function conjectural; PTH-like actions; tumor marker
Growth factors (e.g., epidermal growth factor, fi broblast growth factor, transforming growth factor family, platelet-derived growth factor, nerve growth factors)
Peptides Many Stimulation of cellular growth
Monocytes/Lymphocytes/Macrophages Cytokines (e.g., interleukins 1
to 18, tumor necrosis factor, interferons)
Peptides Many Stimulation or inhibition of cellular growth; other
a aa, Amino acid residues. b Also produced by gastrointestinal tract and pancreas. c Glycoprotein hormones composed of two dissimilar peptides. Th e α -chains are similar in structure or identical; the β -chains diff er among hormones and confer specifi city. d Androstenedione is also produced in the ovary and testis. e Each activin and inhibin is found in multiple forms. f Two chains linked by two disulfi de bonds: α , 24aa; β , 29aa. g Two chains linked by two disulfi de bonds: α , 21aa; β , 30aa. h Also produced in the brain.
TABLE 29-1 Major Hormones and Frequently Measured Hormone Precursors and Cytokines—cont’d
pulsatile secretion of gonadotropins. Examples of hormones of the anterior pituitary gland include the following: • Gonadotropins [luteinizing hormone (LH) and follicle-
stimulating hormone (FSH)] that regulate the develop-ment, growth, and function of the ovary and testis (see
Chapter 56 ). Ovarian and testicular hormones in turn reg-ulate pubertal growth; development and maintenance of secondary sex characteristics; growth, development, and maintenance of the skeleton and muscles; and distribution of body fat.

Chapter 29 ■ Hormones 843
Regulation of the Production, Use, and Storage of Energy Under normal conditions, regulation of energy production, use, and storage is under tight hormonal control. Under con-ditions of changing demands that require more energy (e.g., exercise, starvation, infection or trauma, emotional stress), many hormones are upregulated to control not only circulat-ing levels of nutrients but also the metabolism of these nutri-ents into necessary energy. Th is very complex activity, which may involve hormones from diff erent organs, as already alluded to in the preceding section, is under neurologic control, with numerous neuroendocrine hormones partici-pating actively in this integrative metabolic process, which aff ects most organs in the body and modulates, for example, heart rate, sweating, fertility, and reproduction.
ROLE OF HORMONE RECEPTORS Th e “ unique ” or specifi c action of a hormone on its target tissue is a function of the interaction between the hormone and its receptor. As discussed previously, several types of hormone-receptor interactions may occur. 3,5,8,17 Th e hormone-receptor complex provides the very high specifi city of the action of the hormone, allowing the target tissue to accumu-late the hormone from among all the molecules to which it is exposed. Th is is essential because hormones generally cir-culate in picomolar or nanomolar concentrations (10 − 9 to 10 − 12 mol/L).
Hormone receptors may be on the cell surface or may be intracellular within the cytoplasm or nucleus.
Cell-Surface Receptors Peptide hormones bind to cell surface receptors, and the con-formational change resulting from this binding activates an eff ector system, which in turn is responsible for the down-stream actions of the hormone ( Figure 29-1 ). 11,12 For most peptide hormones, the intracellular eff ector that is activated by the hormone-receptor interaction is a specifi c G-protein (guanyl-nucleotide – binding protein), 4,10,13,18 and the receptors are called G-protein – coupled receptors (GPCRs; Figure 29-2 ). GPCRs are hepta-helical molecules with seven membrane-spanning domains. Th e amino terminus is extra-cellular, and the carboxy terminus is intracellular. Th e major structural classes of GPCRs have been identifi ed, each con-taining receptors for specifi c subsets of hormones ( Figure 29-3 ). Group I is the largest group, containing receptors for many peptide hormones and catecholamines. Group II con-tains receptors for the family of gastrointestinal hormones (secretin, glucagons, and vasoactive intestinal polypeptide). Group III contains the CaSR and the glutamate receptor. Stimulation of a G-protein initiates the intracellular processes of signal transduction that characterize the specifi c action of the hormone. G-proteins are composed of α , β , and γ sub-units and are classifi ed according to the α subunit, of which 20 have been identifi ed to date (see Figure 29-3 ). G-proteins may stimulate adenylate cyclase (G S type of G-proteins) or may inhibit adenylate cyclase (G i type). Th e many classes of
• ACTH that regulates growth of the adrenal glands and synthesis and secretion of adrenal gland hormones (see Chapters 53 and 54 ).
• Th yroid-stimulating hormone (TSH) that regulates growth of the thyroid gland and iodination of amino acids to produce the thyroid hormones triiodothyronine and thy-roxine (see Chapter 55 ). 1
Homeostatic Control of Metabolic Pathways Th e metabolic pathways under hormonal control are diverse and complex. Th e following important examples illustrate the feedback control of hormone secretion, which is critical for homeostasis: • Regulation of blood glucose: In response to a glucose load,
insulin is promptly released from the pancreas, which regu-lates the dispersal of glucose into cells (fat, muscle, liver, and brain) for the metabolism necessary to produce energy from glucose (see Chapter 26 ). As circulating glucose con-centrations thus return to preload concentrations, insulin secretion slows. Several counter-regulatory hormones come into play to further regulate this process to ensure that blood glucose concentrations do not become too low. Th ese include glucagon, cortisol, epinephrine, and growth hormone. Recent attention has focused on a group of gas-trointestinal hormones termed incretins (see Chapter 46 ) that are released during eating and stimulate insulin secre-tion from the pancreas in advance of any measurable increase in blood glucose. Incretins also aff ect the rate of absorption of nutrients from the gut by slowing down the rate of gastric emptying. Another mechanism by which incretins have a role in the regulation of blood glucose is by delaying release of the counter-regulatory hormone glu-cagon from the alpha cells of the pancreatic islets. Th e most studied incretins are glucagon-like peptide-1 (GLP-1) and gastric inhibitory peptide (GIP).
• Regulation of serum calcium (see Chapter 52 ): Th e calcium-sensing receptor (CaSR) on the parathyroid gland recog-nizes the ambient concentration of ionized calcium, which in turn regulates the synthesis and secretion of PTH. When ionized calcium concentrations fall (so imperceptibly that most analytical methods could not detect the change), PTH synthesis and secretion are stimulated. Th is additional PTH will attempt to restore serum ionized calcium by enhancing renal tubular reabsorption of calcium and calcium effl ux from the skeleton. PTH also catalyzes the synthesis of the renal hormone calcitriol (1,25-dihyroxycholecalciferol), which acts on the gut to increase intestinal absorption of calcium. Th ese very rapid responses of PTH and calcitriol quickly restore ionized calcium to concentrations where the CaSR is no longer activated, and PTH and calcitriol synthesis and secretion return to basal rates.
• Water and electrolyte metabolism is regulated by aldoste-rone from the adrenal gland, renin from the kidney, and vasopressin [antidiuretic hormone (ADH)] from the pos-terior pituitary gland (see Chapters 48, 53, and 54 ).

844 Section III ■ Analytes
polypeptide hormones with cell surface receptors changes the conformation of the receptor protein, the binding of a lipid-soluble hormone with its specifi c hormone-binding domain on the intracellular receptor changes the molecular confor-mation of the intracellular receptor. Th is conformational change, or activation of the receptor, enables the hormone-receptor complex to bind to specifi c regulatory DNA sequences of a target gene, permitting control of specifi c gene expression (see Figure 29-1 ). 7
POSTRECEPTOR ACTIONS OF HORMONES Cell surface and intracellular receptors have diff erent postre-ceptor actions.
Cell Surface Receptors Once GPCRs are occupied by a hormone, G-protein subunits begin a cascade of activation of specifi c enzymes that generate molecules that serve as second messengers to eff ect the hormone response. Th e best known of these are adenylyl cyclase, which generates cyclic adenosine monophosphate (cAMP), and phospholipase C, which generates both inositol 1,4,5-trisphosphate (IP 3 ) and diacylglycerol (see Figure 29-2 ). Th e production of second messengers and the subsequent magnitude of the eff ect of the hormone are functions of the amount of hormone bound to the GPCR. Th e binding of a small number of hormone molecules on the cell surface leads to the production of many molecules of the second messen-ger, thus amplifying the signal sent by the hormone (which can be thought of as the fi rst messenger).
cAMP-dependent protein kinases (PKAs) are a family of enzymes that, in the presence of cAMP, phosphorylate a number of intracellular enzymes and other proteins to acti-vate or inactivate the function of these enzymes and proteins, thereby regulating their function. As a further means of regu-lating hormone action, these cAMP-dependent kinases consist of two catalytic and two regulatory subunits (C and R, respectively, in Figure 29-4 ). Th e regulatory subunits exist as a dimer that can bind two molecules of cAMP, and the binding of cAMP releases the catalytic subunits, which then are activated as phosphorylating enzymes. When cAMP is removed from the regulatory subunit, this dimer is not able to associate two catalytic subunits and amplify the signal of the hormone.
Phospholipase C ( Figure 29-2 ) acts on inositol phospho-lipids within the cell membrane to produce IP 3 , which opens up ion channels to facilitate entry of calcium into the cyto-plasm, where it acts as a messenger, and diacylglycerol, which modulates protein kinase C activity.
Th e insulin receptor represents a somewhat diff erent class of cell surface receptors that contain intrinsic hormone-activated tyrosine kinase activity and do not otherwise involve a second messenger. 16 Th e insulin receptor, the prototype of this type of receptor, consists of two α and two β subunits joined by disulfi de bridges. Th e extracellular hormone-binding domains are the α subunits, and the β subunits are intracellular. Th ey contain an ATP-binding site and a catalytic
GPCRs and G-proteins briefl y described in this section provide some insight into the mechanisms responsible for the specifi city of hormone action. Some nonpeptide hormones also use cell surface receptors.
Intracellular Receptors Lipid-soluble hormones such as progesterone (see Figure 29-1 ) are transported in plasma bound to carrier proteins, with only a small fraction of the hormone being in the free or unbound state. Th e free hormone enters the cell via passive diff usion and binds to intracellular receptors in the cytoplasm or, more oft en, the nucleus (see Figure 29-1 ). Th ese receptors are characterized by a hormone-binding domain, a deoxyri-bonucleic acid (DNA)-binding domain, and an amino-terminal variable domain. Just as the interaction of protein or
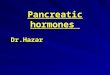
Figure 29-1 Hormonal signaling by cell surface and intracellular receptors. Receptors for the water-soluble polypeptide hormones, luteinizing hormone (LH) and insulin-like growth factor (IGF)-1, are integral membrane proteins located at the cell surface. They bind the hormone using extracellular sequences and transduce a signal through the generation of second messengers — cyclic adenosine monophosphate (cAMP) for the LH receptor and tyrosine-phosphorylated substrates for the IGF-1 receptor. Although effects on gene expression are indicated, direct effects on cellular proteins (e.g., ion channels) are also observed. In contrast, the receptor for the lipophilic steroid hormone progesterone resides in the cell nucleus. It binds the hormone and becomes activated and capable of directly modulating target gene transcription. Tf, Transcription factor; R, receptor molecule. (From Conn PM, Melmed S. Textbook of endocrinology. Towanta NJ: Humana Press, 1997.)
Progesterone
o
o
o
o
o
o
o
o
o
o
Target GenePP
P IGF-I
R
R
R
TFPKA
TFTyr
XTyr
XTyrR
mRNAs
Proteins
Biological Responses
LH
ATPGR
AC
cAMP
ss
s
AAAAA
sss

Chapter 29 ■ Hormones 845
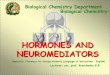
Figure 29-2 Signal transduction by cell surface receptors that are coupled to G-proteins. Two seven-transmembrane domains, coupled to different G-proteins (G S and G q ), are shown. Activation of G S leads to stimulation of the effector enzyme adenylate cyclase and production of a cyclic adenosine monophosphate (cAMP) second messenger, causing the activation of protein kinase A (PKA) and the initiation of potential phosphorylation cascades. Activation of G q leads to stimulation of the effector enzyme phospholipase C- β and the production of inositol 1,4,5-trisphosphate (IP 3 ) and diacylglycerol (DAG) second messengers, one effect of which is to activate protein kinase C (PKC) and initiate a potential phosphorylation cascade. (From Conn PM, Melmed S, eds. Textbook of endocrinology. Towanta NJ: Humana Press, 1997.)
NH2
ATP
cAMP
COOH COOH
PhosphorylatedSubstrate
PhosphorylatedSubstrate
ATP ATP
DAG
CalmodulinKinases
Ca2�
(MembraneAssociated)
Extracellular
ER Stores
PI(4,5)P2
Cellular Responses
P P
cAMPcAMP
R�
NH2
Gs�GTP
Gq�GTP
� �� �
H
AC PLC
PKA PKC
IP3
H
kinase domain through which tyrosine kinase is activated immediately upon insulin binding to the receptor.
Because hormones largely serve a regulatory function, there are of necessity many self-limiting steps in the previous processes. Without these self-limiting processes, hormone action would continue unabated. For cAMP, cessation of hormone action involves the inactivation of G-protein stimu-lation of adenylate cyclase by guanosine triphosphatase (GTPase) ( Figure 29-5 ). In the absence of hormone interac-tion with the GPCR (basal or unstimulated state), G S is bound to guanosine diphosphate (GDP). Once the hormone is bound to the receptor, GDP is released from G s and is replaced by GTP, and the G s -GTP complex activates adenylate cyclase. Th e G s -GTP complex is inactivated by GTPase, restoring the G S -GDP state, which cannot stimulate formation of cAMP until further hormone binding to the GPCR takes place. Within a few minutes (or less) of hormone-GPCR interaction and the initiation of hormone action, the receptor is phos-phorylated by protein kinase A and protein kinase C. Th is
phosphorylation of the hormone receptor permits inter-nalization of the complex from the cell surface into the cytoplasm where dephosphorylation occurs, permitting degradation of the hormone and recycling of the GPCR to its original transmembrane location, awaiting coupling with more hormone.
Intracellular Receptors As noted, lipid-soluble hormones bind to the hormone-binding domain of cytosolic or nuclear receptors. 11,12 Th is results in a conformational change that enables the hormone-receptor complex to bind to specifi c regulatory DNA sequences in the 5 ′ end of the target gene. 7 Th e binding speci-fi city of the (hormone-bound) receptor for specifi c regions of the DNA of the target gene is determined by zinc fi nger structures in the receptor ’ s DNA-binding domain. It is the binding of the hormone-receptor complex to DNA regulatory elements that enhances or represses gene transcription. Th e messenger ribonucleic acid (RNA) that is enhanced or

846 Section III ■ Analytes
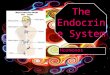
Figure 29-3 Classifi cation and basic architecture of cell surface receptors that couple to G-proteins. A, Lists the major families and groups of G-protein – coupled receptors (GPCRs). The mammalian receptors are confi ned to families A, B, and C. Family A is the largest and includes the diverse odorant receptors and prototypic GPCRs such as rhodopsin and the β -adrenergic receptor. B, Shows a schematic structure of one of the most extensively characterized GPCRs, the β -adrenergic receptor. Major structural features are indicated and are expanded on in the text. (From Conn PM, Melmed S, eds. Textbook of endocrinology. Towanta NJ: Humana Press, 1997.)
G Protein-Coupled Receptor (GPCR) Superfamily
Family A:
Group I:Group II:Group III:Group IV:Group V:Group VI:
Receptors Related to Rhodopsinand the �-Adrenergic Receptor
Olfactory, Adenosine, Melanocortin RsAdrenergic, Muscarinic, Serotonin, DA RsNeuropeptide Rs and Vertebrate OpsinsBradykinin R and Invertebrate OpsinsPeptide and GP Hormone, Chemokine RsMelatonin and Orphan Rs
Family B:
Group I:Group II:Group III:
Receptors Related to the Calcitoninand Parathyroid Hormone Receptors
Calcitonin, Calcitonin-like, CRF RsPTH and PTHrP RsGlucagon, Secretin, VIP, GHRH Rs
Family C:
Group I:Group II:
Receptors Related to the MetabotropicGlutamate Receptors
Metabotropic Glutamate RsExtracellular Calcium Ion Sensor Rs
Family D:
Group I:
Receptors Related to the STE2Pheromone Receptor
Alpha Factor Pheromone Rs
Family E:
Group I:
Receptors Related to the STE3Pheromone Receptor
A Factor Pheromone Rs
Family F:
Group I:
Receptors Related to the cAMPReceptor
Dictyostelium cAR1-4 Rs
A
Glycosylation
Agonist Binding
Antagonist BindingConserved Cysteines
TMD1 TMD2 TMD3 TMD4 TMD5 TMD6 TMD7
PKA Phosphorylation
Palmitoylation
G-Protein Coupling
�ARK Phosphorylation
P
COOH
B
Required for CatecholamineBinding and Activation
Asp 113 Ser 204, 207
P
P P P P P P

Chapter 29 ■ Hormones 847
hormones that bind to intracellular receptors are rapid and do not depend on synthesis of protein, suggesting that these hormone-receptor complexes exert actions by mechanisms diff erent from binding to DNA.
From these descriptions, one can begin to deduce both the complexity and the specifi city of hormone action, in terms of an “ on and/or off ” concept and in terms of an “ eff ect size ” concept.
CLINICAL DISORDERS OF HORMONES Although several chapters of this textbook detail a variety of endocrine disorders, a brief introduction is appropriate here. In general, endocrine diseases may result from a defi ciency or an excess of a single hormone or several hormones, or from resistance to the action of hormones. Hormone defi -ciency can be congenital or acquired, and hormone excess can result from endogenous overproduction (from within the body) or exogenous overmedication. Hormone resistance can occur at several levels but can most simply be character-ized as receptor mediated, postreceptor mediated, or at the level of the target tissue. Th e clinical manifestations will depend on the hormone system aff ected and the type of abnormality.
Diabetes mellitus (DM) is an example of an endocrine disorder; it is the most common endocrine disorder in the United States (see Chapter 46 ). It is classifi ed as type 1 or type 2. DM type 1 results from failure of the pancreas to secrete insulin even though the pancreas is otherwise normal. Type 2, the most common form of DM, results from end-organ resistance to the action of insulin, which, in this case, is secreted from the pancreas in abundant amounts and circu-lates at high concentrations. Secondary DM occurs when a nonendocrine disease such as pancreatitis destroys the pan-creas, including the insulin-secreting cells. Th e biochemical hallmark of DM is hyperglycemia.
In contrast to diabetes, there are uncommon, insulin-producing tumors of the pancreas (insulinomas) in which the production of insulin is not regulated by the blood glucose concentration and the biochemical hallmark of the tumors is hypoglycemia. Th us hyperglycemia can be present when there is insulin defi ciency or insulin excess, and insulin excess can accompany both hyperglycemia and hypoglycemia. Th is simple illustration underscores the homeostatic and/or regu-lating nature of the endocrine system.
MEASUREMENTS OF HORMONES AND RELATED ANALYTES Hormones are measured by a variety of analytical techniques, including bioassay, receptor assay, immunoassay, and instru-mental techniques such as mass spectrometry interfaced with liquid or gas chromatography. A general overview of these techniques is given here. Analytical details for indi-vidual hormones using such techniques are found in the discussion of the individual hormones in their respective chapters.
diminished by hormone receptor binding to the target gene regulates the synthesis of specifi c proteins that mediate the hormone ’ s physiologic actions. Th e system is further regu-lated by the presence or absence of coactivators or core-pressors of gene expression. In addition, many actions of
Figure 29-4 Signaling by G S . The alpha, beta, and gamma subunits of G s are shown. The alpha subunit, when bound to GTP, activates adenylyl cyclase which catalyzes the formation of cyclic AMP (cAMP) from ATP. Then cAMP binds to the regulatory subunit (R) of protein kinase A (PKA, cyclic AMP-dependent protein kinase), releasing PKA ’ s catalytic subunit (C) and thus leading to phosphorylation of target proteins. (Image from Conn PM, Melmed S, eds. Textbook of endocrinology. Towanta NJ: Humana Press, 1997.)
Ligand
Receptor Adenylylcyclase
InactivePKA
GDP
R
R R
C
R
C
C C
�s
�s
GTP
ATP
cAMP
cAMP
cAMP
cAMP
cAMP
Targetproteins
ActivePKA
�s
�
�
Figure 29-5 The G-protein cycle. The alpha, beta, and gamma subunits of G s are shown. The alpha subunit, when bound to GTP, activates the effector molecule (such as adenylyl cyclase, see Figure 29-4 ). GTP then is hydrolyzed to GDP, stopping the activation of the effector molecule and leading to reformation of the GDP-bound state of the G protein. (Image from Conn PM, Melmed S, eds. Textbook of endocrinology. Towanta NJ: Humana Press, 1997.)
Ligand
Receptor Effectormolecule
GDP
GDP
GDP
GTP
GTP
�� �
�
�
�
�
�
�
�

848 Section III ■ Analytes
electrospray ionization techniques that allow sequencing of peptides and mass determination of picomole quantities of analytes.
Compared with older methods, tandem mass spectrome-try off ers greater analytical sensitivity, accuracy, and speed, and may allow simultaneous determination of multiple hor-mones related to a clinical condition. 14
Specimen Requirements As can be seen from the brief descriptions of hormone action given previously and amplifi ed in the hormone-specifi c chap-ters, particular attention must be paid to the clinical material sent to the laboratory for assay. Some hormones are directly aff ected by food (e.g., insulin) or by circadian variability (e.g., cortisol). In many clinical circumstances, the metabolic envi-ronment plays a crucial role in hormone production, and it is essential to obtain a simultaneous sample for measurement of both the hormone and the molecule(s) regulated by that hormone. An isolated measurement of plasma insulin without concurrent knowledge of the plasma glucose, or measure-ment of parathyroid hormone independent of serum calcium, is of little if any value. When a patient is evaluated for possible hormone defi ciency or hormone excess, it is oft en necessary to perform a stimulation or suppression test. Most hormone assays can be performed on plasma or serum, and many can be performed on urine samples, usually a 24 hour collection. Increasingly, saliva has become a convenient body fl uid for hormone analysis, particularly for hormones secreted in a diurnal rhythm such as cortisol. Unlike blood sampling, which requires the patient to present to a blood drawing facil-ity, patients can be provided with salivary collection material such that they can provide to the laboratory specimens col-lected at multiple times during the day or at unusual (but biologically very relevant) times such as 11 pm — a commonly used time for obtaining a specimen for measurement of cortisol.
REFERENCES 1. Brent GA . Th e molecular basis of thyroid hormone action . N Engl J
Med 1994 ; 331 : 847 - 53 . 2. Chace DH . Mass spectrometry in the clinical laboratory . Chem Rev
2001 ; 101 : 445 - 77 . 3. Edwards DP . Th e role of co-activators and co-repressors in the biology
and mechanism of action of steroid hormone receptors . J Mammary Gland Biol Neoplasia 2000 ; 5 : 307 - 24 .
4. Farfel Z , Bourne HR , Iiri T . Th e expanding spectrum of G protein disease . N Engl J Med 1999 ; 340 : 1012 - 20 .
5. Funder JW . Mineralocorticoids, glucocorticoids, receptors and response elements . Science 1993 ; 259 : 1132 - 3 .
6. Giese RW . Measurement of endogenous estrogens: analytical challenges and recent advances . J Chromatogr A 2003 ; 1000 : 401 - 12 .
7. Glass CK . Diff erential recognition of target genes by nuclear receptor monomers, dimers, and heterodimers . Endocr Rev 1994 ; 15 : 391 - 407 .
8. Klinge CM . Estrogen receptor interaction with estrogen response elements . Nucleic Acids Res 2001 ; 29 : 2905 - 19 .
9. Lagerstedt SA , O ’ Kane DJ . Measurement of plasma free metanephrine and normetanephrine by liquid chromatography-tandem mass spectrometry for diagnosis of pheochromocytoma . Clin Chem 2004 ; 50 : 603 - 11 .
10. Lefk owitz RJ . G proteins in medicine . N Engl J Med 1995 ; 332 : 186 - 7 .
Bioassay Techniques Bioassays are based on observations of physiologic responses specifi c for the hormone being measured. In vivo bioassays usually involve the injection of test materials (such as blood or urine from a patient) into suitably prepared animals; target gland responses such as growth or steroidogenesis are then measured. In vitro bioassays involve the incubation of tissue, membranes, dispersed cells, or permanent cell lines in a defi ned culture medium, with subsequent measurement of an appropriate hormone response. Most in vitro bioassays measure responses proximal or distal to a second messenger such as stimulation of cAMP formation. Bioassays tend to be imprecise and are rarely necessary in clinical medicine.
Receptor-Based Assays Receptor assays depend on the in vitro interaction of a hormone with its biological receptor. In this type of assay, unlabeled hormone displaces trace amounts of radioactively labeled hormone from receptor sites. A second approach is to measure a response, such as production of cAMP, when a test sample is added to a preparation that includes the recep-tor and necessary cofactors. In general, receptor assays are simpler to perform and have greater sensitivity than bioas-says. Receptor assays also have an advantage over immunoas-says in that they refl ect the biological function of a hormone, namely, the capacity to combine with specifi c receptor sites. By contrast, immunoassays may measure active hormone and inactive prohormone, hormone polymer, and metabolites when all share a common antigenic determinant or set of determinants. In general, receptor assays are not as sensitive as immunoassays, and enzymes in the biological specimen may degrade the receptor or destroy the labeled tracer. Th e added complexity and lability of receptor preparations also contribute to the limited application of these assays in the routine clinical laboratory.
Immunoassay Techniques Immunoassays employing antibodies are widely used to quantify hormones (see Chapter 16 ). Currently labeled anti-body (immunometric) assays with nonisotopic labels are the method of choice for measuring most hormones, especially peptides and proteins. Immunometric assays use saturating concentrations of two or more antibodies (oft en monoclonal) that are prepared against diff erent epitopes of the protein molecule. One of the two antibodies is usually attached to a solid phase separation system and extracts the hormone from the serum specimen. Th e second antibody is linked to a signal molecule, which is then measured. Th e resultant signal is used to quantify the bound hormone.
Instrumental Techniques Mass spectrometers (see Chapter 14 ) coupled with gas and liquid chromatographs (see Chapter 13 ) are powerful qualitative and quantitative analytical tools that are widely used to measure hormones. 2,6,9,14 Technical advancements in mass spectrometry have resulted in the development of matrix-assisted laser desorption/ionization (MALDI) and

Chapter 29 ■ Hormones 849
11. Mangelsdorf DJ , Th ummel C , Beato M , Herrlich P , Schutz G , Umesono K , et al . Th e nuclear receptor superfamily: the second decade . Cell 1995 ; 83 : 835 - 9 .
12. McKenna NJ , Lanz RB , O ’ Malley BW . Nuclear receptor coregulators: cellular and molecular biology . Endocr Rev 1999 ; 20 : 321 - 44 .
13. Neer EJ . Heterotrimeric G proteins: organizers of transmembrane signals . Cell 1995 ; 80 : 249 - 57 .
14. Nelson RE , Grebe SK , O ’ Kane DJ , Singh RJ . Liquid chromatography-tandem mass spectrometry assay for simultaneous measurement of estradiol and estrone in human plasma . Clin Chem 2004 ; 50 : 373 - 84 .
15. Newman WA . Dorland ’ s illustrated medical dictionary , 30th edition . Philadelphia, Pa : WB Saunders , 2003 .
16. Olefsky JM . Th e insulin receptor: a multifunctional protein . Diabetes 1990 ; 39 : 1009 - 16 .
17. Pike AC , Brzozowski AM , Hubbard RE . A structural biologist ’ s view of the oestrogen receptor . J Steroid Biochem Mol Biol 2000 ; 74 : 261 - 8 .
18. Vaughan M . Signaling by heterotrimeric G proteins minireview series . J Biol Chem 1998 ; 273 : 667 - 13 .