Embed Size (px)
Citation preview

K.SRINIVAS
Ist yr pg
Department of general medicine

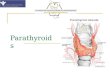
PARATHYROID GLANDS Two pairs of parathyroid
glands positioned behind the outer wings of thyroid.
Superior and inferior parathyroid glands.
Secretes parathyroid hormone

PARATHYROID HORMONE(PTH) 84 aminoacid single chain peptide.
Primary function is to maintain the ECF calcium concentration with in normal range.
Acts directly on
bone(calcium resorption)
kidney(calcium reabsorption)
Stimulates 1 alpha hydroxylase activity, increases production of 1,25(OH)2D,which increases the efficiency of calcium absorption.

PTH secretion increases steeply to a maximum value
of about 5 times the basal rate of secretion as calcium
concentration falls to the range of 7.5-8mg/dl.
ECF calcium controls PTH secretion by interaction
with a calcium sensor, a G protein coupled
receptor(GPCR)


PTHrP(parathyroid hormone related protein)
Responsible for most instances of hypercalcemia of malignancy.
A syndrome that resembles hyperparathyroidism but without elevated PTH levels.
Produced by brain,pancreas,heart,lung,mammorytissue,placenta and endothelial cells.

PRIMARY HYPER PARATHYROIDISM.
A generalized disorder of calcium,phosphate and
bone metabolism due to increased secretion of
PTH leading to hypercalcemia and
hypophosphatemia.

parathyroid tumors
solitary adenoma
rarely a parathyroid carcinoma
MEN syndromes.
MEN1 (wermers syndrome)
MEN2A
Hyperparathyroid jaw tumors.
Non syndromic familial isolated hyperparathyroidism.
Etiology

Secondary hyperparathyroidism
Is an adaptive process that develops in response to
declining kidney function, impaired phosphate excretion and failure to bioactivate vitD.
Teritiary hyperparathyroidism
Is a state of severe hyperparathyroidism in patients with renal failure that requires surgery .

SECONDARY HYPERPARATHYROIDISMEtiology Kidney failure requiring dialysis.
Stomach or intestine bypass surgery for obesity surgery.
Celiac disease.
Crohns disease.
Severe vit D deficiency.

Pathophysiology
Continuous stimulation of the parathyroid glands by a combination of
increased phosphate concentration and decreased calcium concentration and markedly reduced serum calcitriol
increased PTH secretion and synthesis
parathyroid hyperplasia



vitaminD Is an essential factor for regulation of calcium and
phophorous.
Active form is 1,25dihydroxy vitaminD .
Increases the intestinal absorption of calcium and phosphorous.
Increase reabsorption of calcium and phosphorous in the renal tubules.
Direct effect on the parathyroid glands to supress PTH secretion

Vitamin D metabolism

FGF23(fibroblast derived growthfactor)
Secreted mainly by osteocytes (and possibly osteoblasts).
Now consider to be the most important factor for regulation of phosphorous homeostasis.
Acts mainly on the kidneys to increase phosphorous clearance.
Inhibits 1αhydroxylase activity causing a low 1,25, dihydroxyvitamin D level.
Hyperphosphatemia is the main stimulant for FGF23


Calcium and phosphorous metabolism in renal failure
When GFR falls,the phopsphorous clearance decrease leading to phopshate retention.
Hyperphosphatemia induces PTH secretion by 3 ways
1. Direct stimulatory effect on parathyroid.
2. Induction of mild hypocalcemia by precipitating with calcium to form (caHpo4).

3. Stimulation of FBG23
Decreased 1αhydroxylase
Decreased 1,25 dihydroxyvitaminD
Down regulation of vitD receptors parathyroidgland


Clinical features
Renal osteodystrophy
bone and joint pains.
bone deformation and fractures during late stages .
Some times called as silent crippler .
Osteitis fibrosis cystica.
A dynamic or aplastic bone disease.

Osteitis fibrosis cystica
Classic and former most common form of osteodysrophy.
High bone turn over caused by high circulating PTH.
Histologically ,an increase in gaint multinucleated osteoclasts on the surface of the bone and replacement of normal cellular and marrow elements with fibrofattytissue.
Xray changes include sub periosteal resorption of the phalangeal tufts.

Subperiostel resorption

Aplastic or adynamic bone disease
Low bone turn over by excessive supression of PTH during late stages of disease.
The number of PTH receptors is downregulated in the skeleton leading to skeletal resistance.
It is a normal mechanism of the bone to defend itself against high circulating levels of PTH.


Treatment Management of secondary hyperparathyroidism in CKD
should start at the beginning of stage 3
It can be divided in to 3 steps
1. Optimize the levels of serum calcium and phosphate.
2. Control of PTH and vitaminD
3. The dosages of phosphate binders, calcimimmetics and vitD analogues should be adjusted to achieve K/DOQI value

1st step is to optimize the levels of serum phosphate and calcium through dietary restriction of phosporous and phosphate binders
Dietary restriction of phosphorous
For ptnts with CKD stage 3 and 4 when serum phosphorous is more than 4.6 and 5.5 mg/dl in CKD 5.
Dietary restriction of phosphorous to 800-1000mg/day
Two main sources dietary proteins and phosphorous additives
Additives are manily present in the processed foods such as meat,beverages,cheese and dietary products.


Phosphate binders
main stay of therapy in secondary hyperparathyroidism.
To limit the dietary absorption of phopsphorous.
Aluminium hydroxide forms aluminium precipitates in the intestine and lowers phosphatemia levels.
Used when serum phosphorous is >7mg/dl for lessthan 4 weeks
Aluminium toxicity leads to severe refractory microcyticanemia,osteomalacia,dementia
Calcium salts as calcium carbonates and calcium acetates

Sevelamer hydrochloride is non calcium,non aluminium and non magnesium compound.
it forms a cationic polymer that binds to dietary phosphorous through ion exchange.
Sevelamer carbonate replacement of chloride ion with a carbonate.
decrease s the chances of metaboilic acidosis caused by sevalmerhydrochloride.
Lanthum carbonates is a rare earth element and has the property of phosphorous binding.

Step 2 is to control of PTH and vitD by the use of vit D analogues and calcimimetics.
vitD and its derivatives is the oldest treatment for secondary hyperparathyroidism.
Calcitriol deficiency and resistance are the major contributors to the pathophysiology of the disease.
Calcitriol(1,25dihydroxyvitaminD3)is the natural form of vitamin D produced by the humanbody.
Intermittent and IV administration is more effective than oral calcitriol
Ergocalciferol s vitamin D2 or the nutritional vitamin D
Is only indicated if 25-hydoxy vitamin D levels<30ng/ml;

Selective vitamin D analogues are paricalcitol and
doxercalciferol.
Selective agents that have more affinity towards kidney rather than intestinal receptors.
Calcimimetics are the newer agents that allostericallyincrease the sensitivity to calcium and calcium sensing receptors in the parathyroid gland thus supressing PTH.
Cinacalcet is indicated in dialysis patients when sercalcium>8.4mg/dl and PTH levels>300pg/ml.
Side effects include GI symptoms and qt prolongation syndrome.

parathyroidectomy
Indications
Medical therapy is insuccessful
Extraskeletal calcification.
Calciphylaxis
Refractory pruritis
Severe hypercalcemia
PTH levels>800pg/ml

It can be performed by either subtotal or total parathyroidectomy with autotransplantation.
Small amounts of resected parathyroid tissue can be autografted in the muscles of the forearm or neck as well as in subcutaneous tissues of chest or abdomen.
Hungry bone syndrome is the lack of osteoclasticactivity caused by decreased PTH postoperatively causes fall in calcium levels.
Monitoring of calcium levels is important in follow up after surgery.