Embed Size (px)
Citation preview

SAMIR EL ANSARY
DefinitionsSepsis = suspected or proven infection
and some of the following:General VariablesInflammatory VariablesHemodynamic VariablesOrgan Dysfunction VariablesTissue Perfusion Variables
Sepsis VariablesGeneral InflammatoryFeverHypothermiaTachycardiaAltered Mental StatusEdemaHyperglycemia
LeukocytosisLeukopeniaNormal WBC with > 10
% immature formsC-reactive protein > 2
SDProcalcitonin > 2 SD

Sepsis VariablesHemodynamic Organ DysfunctionSBP <90MAP < 70SBP decrease > 40
Tissue PerfusionLactate > 1MottlingDecreased Capillary
Refill
P/F < 300UO < .5 ml/kg for 2
hours despite volume resuscitation
Cr increase > .5INR > 1.5IleusPlt < 100 KBili > 4
Severe Sepsis DefinitionSepsis induced organ dysfunction, hypoperfusion,
or hypotensionHypotensionElevated Lactic AcidOliguriaALI with P/F < 250 without pneumoniaALI with P/F < 200with pneumonia
Cr > 2Bili > 2Plt < 100KINR > 1.5
Septic Shock
Sepsis-induced hypotension that persists despite adequate fluid resuscitation
*All definitions cited from “Surviving Sepsis Campaign” published in Critical Care Medicine Feb 2013
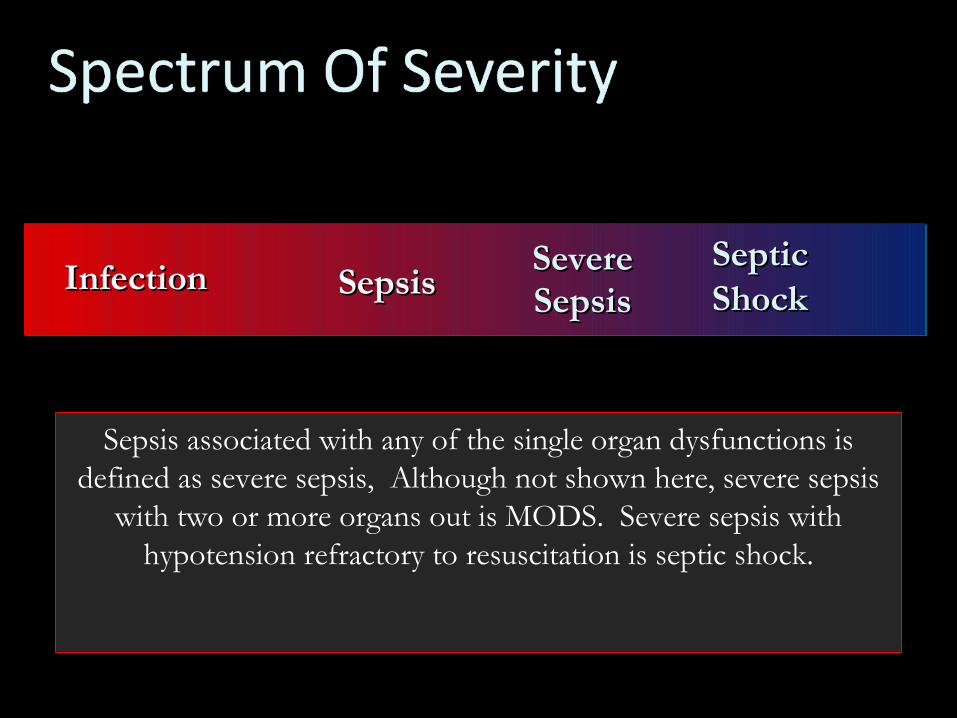
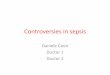
SepsisSepsisInfectionInfection Severe Severe SepsisSepsis
Septic Septic ShockShock
Sepsis associated with any of the single organ dysfunctions is defined as severe sepsis, Although not shown here, severe sepsis
with two or more organs out is MODS. Severe sepsis with hypotension refractory to resuscitation is septic shock.
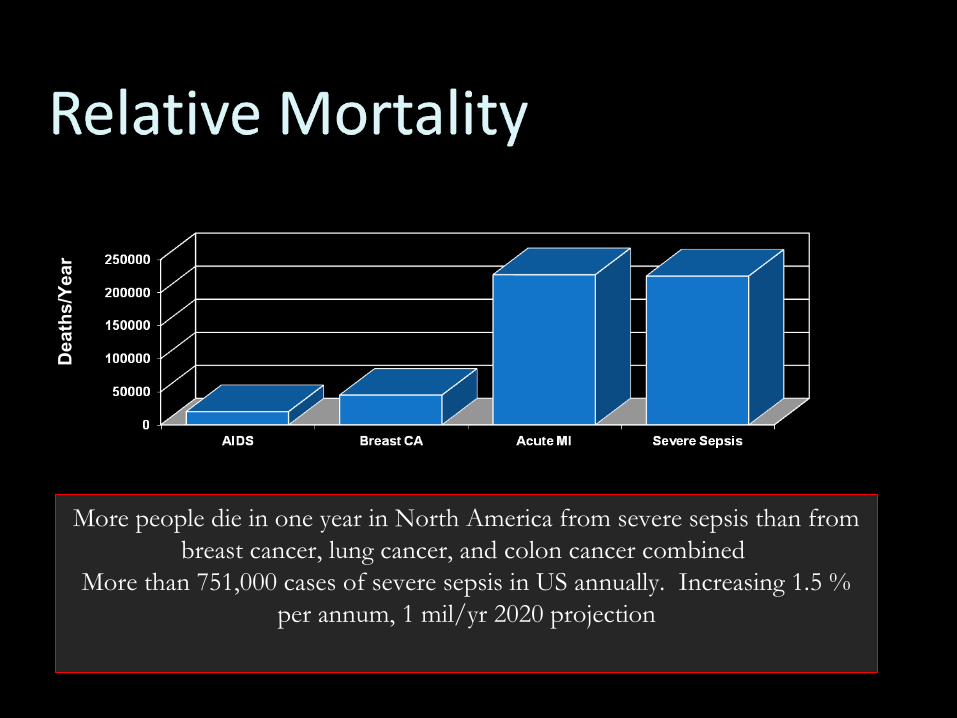
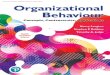
Deaths/Year
More people die in one year in North America from severe sepsis than from breast cancer, lung cancer, and colon cancer combined
More than 751,000 cases of severe sepsis in US annually. Increasing 1.5 % per annum, 1 mil/yr 2020 projection
Source control is most vital factor
Adequate resuscitation or re-established perfusion in 6 hours
Appropriate antibiotic therapy within 1 hr of hypotension
Determinants of Mortality
InterventionsEarly Goal Directed Therapy
(EGDT)Anti-microbialsSteroidsGlucose ControlLung Protective Ventilation
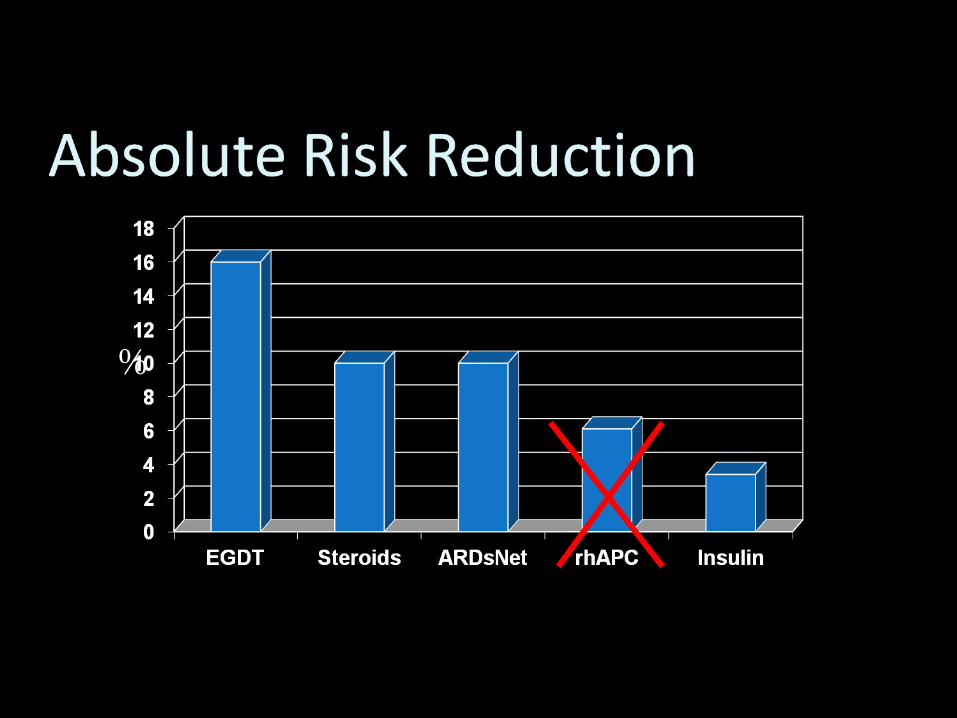
%
EGDT ResuscitationBegin at onset of hypotension or
lactate >4Do not delay while awaiting ICU
admissionInitial bolus is 30 ml/kg
crystalloid
Or mixed venous greater than or equ to 65%; Dobut infusion to max 20 microgr/kg/minute.
Early goal-directed resuscitation has been shown to The consensus panel judged use of central venous and
mixed venous oxygen saturation targets to be equivalent.
Either intermittent or continuous measurements of oxygen saturation were judged to be acceptable. Studies of patients with shock indicate that mixed venous oxygen saturation runs 5–7% lower than
central venous oxygen saturation (Scvo2)
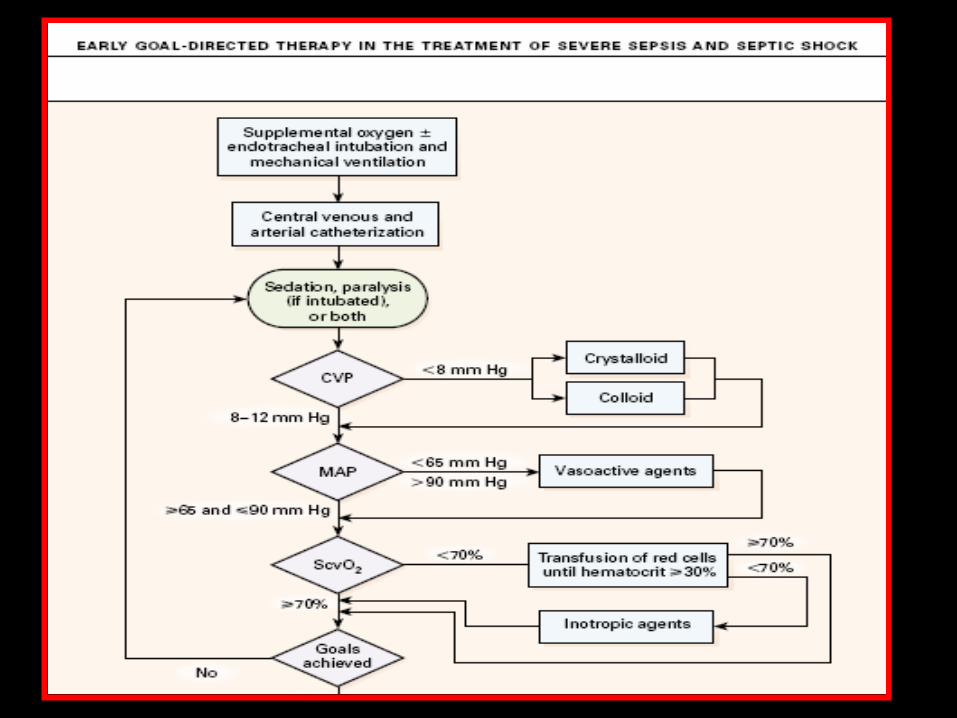
EGDTInitial Resuscitation targets
CVP 8-12 (12-15 if mechanically ventilated)Mean arterial pressure ≥65Urine output ≥ 0.5 ml/kg/hourCentral venous oxygen saturation ≥ 65%If venous oxygen target still not achieved:
trial of fluid or transfuse PRBCs to HCT ≥30% and/or start dobutamine infusion
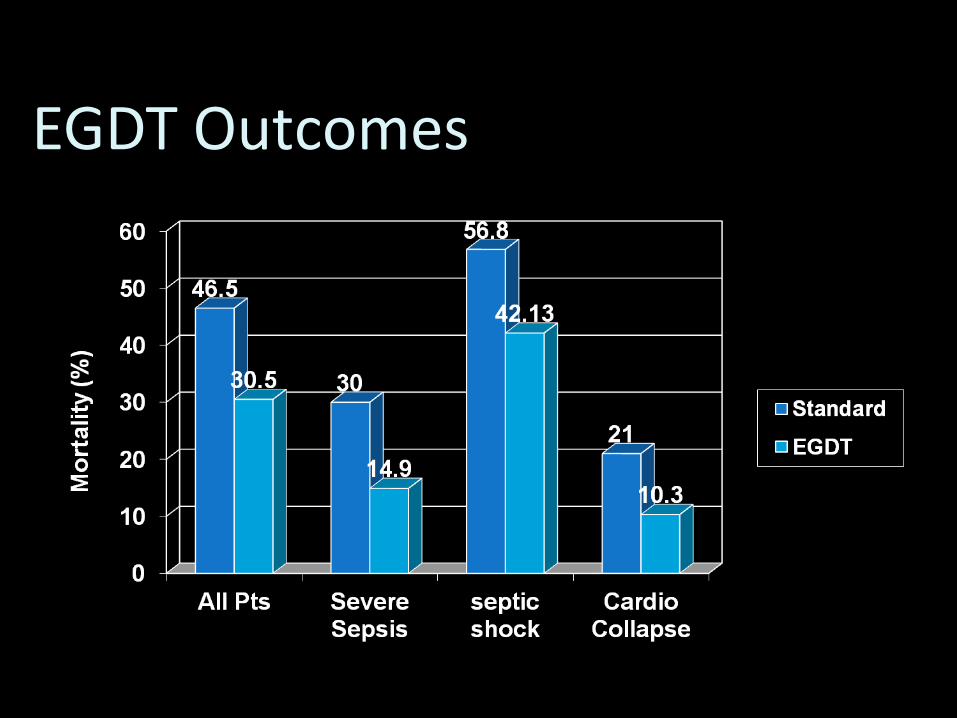
EGDT Outcomes
EGDT Cost23% reduction in hospital costMean reduction of 4 days per
hospital admissionCost per life savedReduction in hospital charges
What to Use?
Guideline: Colloid or crystalloid may be
usedUse of either 4 percent albumin or normal saline for fluid
resuscitation results in similar outcomes at 28 days.
EGDT (and we mean EARLY)
Adequate initial fluid resuscitation (AIFR) groupAdministration of an initial fluid bolus of ≥ 20
mL/kg prior to and achievement of a central venous pressure of ≥ 8 mm Hg within 6 h after the onset of therapy with a vasopressor
Conservative late fluid management (CLFM) Even-to-negative fluid balance measured on at least
2 consecutive days during the first 7 days after septic shock onset
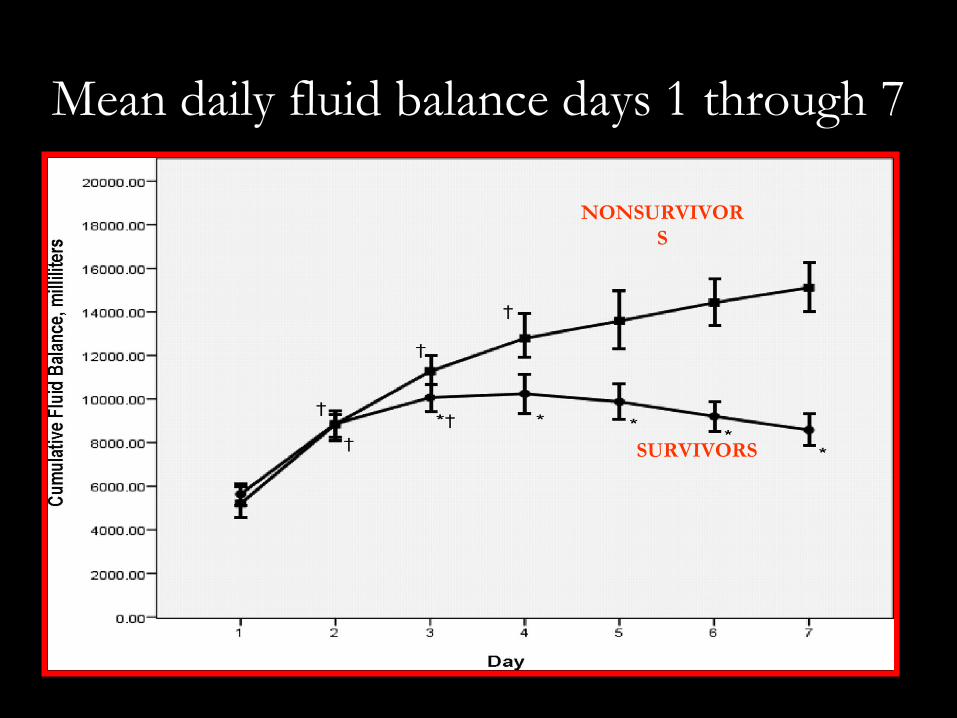
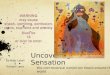
Mean daily fluid balance days 1 through 7
NONSURVIVOR
S
SURVIVORS
VasopressorsMean arterial pressure (MAP)
maintained ≥ 65First choice: norepinephrine or
epinephrineVasopressin 0.03 units/min may be
added
Inotropes
Dobutamine infusion for suspected myocardial dysfunction suggested by elevated cardiac filling pressures and low cardiac output
Recommend against a strategy to increase cardiac index to supranormal levels
InterventionsEarly Goal Directed Therapy (EGDT)
Anti-microbialsSteroidsGlucose Control
AntimicrobialsBegin therapy within the first hour of recognizing
severe sepsis or septic shockBroad spectrum: one or more agents against likely
bacterial or fungal pathogensConsider combination therapy for potentially
resistant gram negative pathogensConsider combination therapy in neutropenic
patientsNarrow coverage when culture data available
InterventionsEarly Goal Directed Therapy
(EGDT)Anti-microbialsSteroidsGlucose Control
Steroid GuidelinesThe ACTH stimulation test should not be used to
identify the subset of adults with septic shock who should receive hydrocortisone.
Do not use corticosteroids in the treatment of sepsis in the absence of shock.
Corticosteroid therapy may be weaned when vasopressors are no longer required.
Recommended: hydrocortisone 50 mg iv q 6 hours
Also most cortisol assays measure total and free cortisol, while free is likely the pertinent
measurement. The corticol assays may over or underestimate the
the actual cortisol level since the relationship between free and total cortisol depends on serum
protein concentration.Dex can lead to profound and prolonged supression of the adrenal axis and along with no ACTH test, no
need for dex.
InterventionsEarly Goal Directed Therapy
(EGDT)Anti-microbialsSteroidsGlucose Control
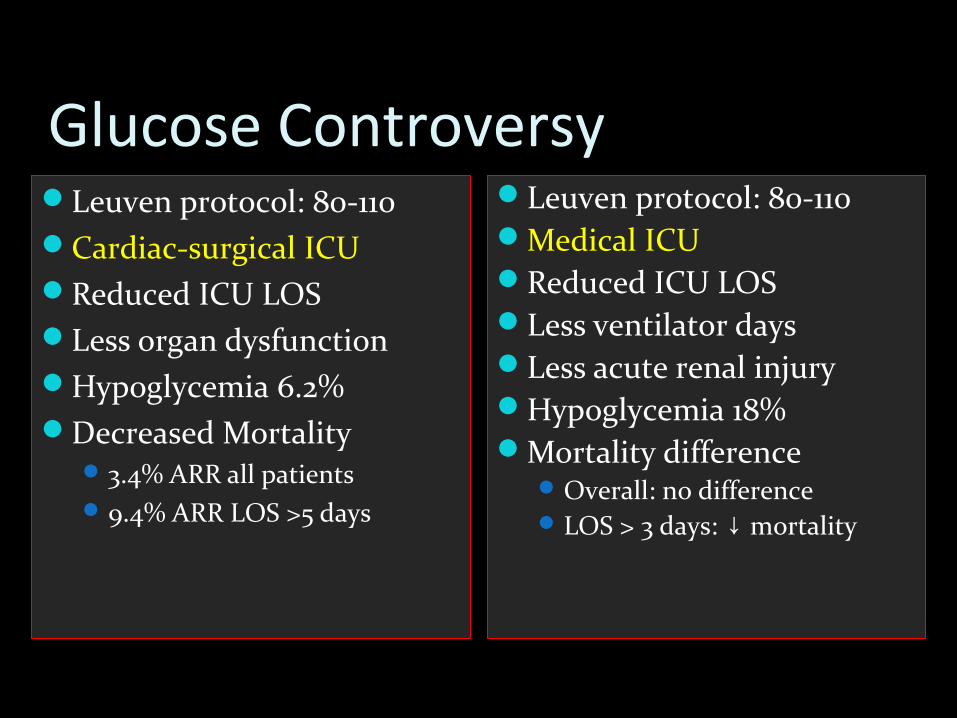
Glucose ControversyLeuven protocol: 80-110Cardiac-surgical ICUReduced ICU LOSLess organ dysfunctionHypoglycemia 6.2%Decreased Mortality
3.4% ARR all patients9.4% ARR LOS >5 days
Leuven protocol: 80-110Medical ICU Reduced ICU LOSLess ventilator daysLess acute renal injuryHypoglycemia 18%Mortality difference
Overall: no difference LOS > 3 days: mortality↓
Glucose Control Guidelines
Patients with severe sepsis and hyperglycemia in the ICU should receive intravenous insulin.
Use validated protocol for insulin dose adjustment with a target glucose <180.
All patients on intravenous insulin receive a glucose calorie source.
Resuscitation “Bundles”Severe Sepsis 3 Hour Bundle
RecognitionFluid ResuscitationAntimicrobial TherapyOxygen Delivery
Severe Sepsis 6 Hour BundleLow-dose Steroids Glucose ControlLung Protective Ventilation
GOOD LUCK
SAMIR EL ANSARY