Embed Size (px)
Citation preview

CLINICAL REDESIGN Looking back to see the future

▪What is redesign all about?
▪Why do it?
▪What has it got to offer?



A FUNDAMENTAL ASSUMPTION OF MEDICAL DECISION MAKING
▪ “Our minds are interpreters of evidence. We can accurately convert all forms of evidence into conclusions, which in turns determines our actions”
▪ “Therefore, no one has to tell us what to do. Just give us the evidence and we will work it out. Besides there are lots of other factors to be considered. That can only be done with clinical judgement.”
▪ Dr David Eddy

LEAVE CLINICIANS TO SORT IT OUT?

THE FUNDAMENTAL ASSUMPTION IS WRONG
Poor evidence for most practices The inherent complexity of modern medicine , versus the limitations
of the human mind
Lead to
High variations in beliefs Well documented, massive variations in practices
High rate of inappropriate care Unacceptable rates of preventable patient injury
Wasted resources on a large scale Dr David Eddy

PROCESS MANAGEMENT DESIGNS
Do they work for medicine?

SCIENTIFIC MANAGEMENT Developed by Frederick Taylor Approx 1911
Defined mass production
Based on the idea of process, management led design
uneducated workers, cogs in a machine
Very successful

TAYLORISM CONTINUED Hardly a competent workman can be found who does not devote a considerable part of time to studying just how slow he can work and still convince his employer that he is going at a good pace…Under our system a worker is told just what to do and how he is to do it It is only through the enforced standardisation of methods, enforced adoption of best implements and working conditions, and enforced cooperation that this faster work can be assured. The duty of enforcing the adoption of standards and of enforcing this cooperation rests with management alone. Any of those who after proper teaching can not or will not work in accordance with the new methods must be discharged by management
Frederick Taylor The Principles of Scientific Management 1911

SCIENTIFIC MANAGEMENT
Scientific Management fails in the face of
Complexity

THE CRAFT OF MEDICINE
An individual doctor placing patients health needs above any other goal, drawing on extensive clinical knowledge gained through formal education and experience
Can Craft
A unique diagnostic and treatment plan customized for an individual patient

THE CRAFT OF ADMINISTRATION
Under the craft of medicine the role of the organisation is to create an environment within
which individual, independent medical professionals can interact with their patients
without undue distractions that could harm care
So we see the development of business solutions to solve business problems and financial measures to
manage facilities

OPPOSING IDEALS
Administrative management versus clinical management

QUALITY IMPROVEMENT AND PROCESS MANAGEMENT
1911 Frederick Taylor 1931 Walter Shewhart Economic Control of Manufactured Product 1939 Statistical Method from the Viewpoint of Quality Control 1951 W. Edwards Deming Elementary Principles of the Statistical Control of Quality

W.EDWARDS DEMING
Organize everything around value added (front line) work processes
Quality Improvement is the science of process management

SHEWHART/DEMING PDSA CYCLE

Taylor Top Down Deming Bottom Up Hardly a competent worker can be found
Almost all failures come from underlying processes
Critize/Control Empower
Judgement playing God Learning
Heroic Individuals Teams (fundamental knowledge)
Unfunded mandates assumes unlimited time and attention
Integrated Tools built into workflow
Motivate incentivize (payment)
Make it easy to do right

QUALITY IMPROVEMENT AND PROCESS MANAGEMENT
1911 Frederick Taylor 1931 Walter Shewhart Economic Control of Manufactured Product 1939 Statistical Method from the Viewpoint of Quality Control 1951 W. Edwards Deming Elementary Principles of the
Statistical Control of Quality
1990 Womack Jim The Machine that changed the World (Lean)

LEAN OR PULL THROUGH PRODUCTION
Standardisation processes with
Smart cogs that
Adapt to individual needs
Mass customisation
Efficient processes that can deal with complexity

PROTOCOLS CAN IMPROVE CARE
Shared baselines (lean production)
A multidisciplinary team of health care professionals • Select a high priority care process
• Generate an evidence based “best practice” guideline • Blend the guideline into the flow of clinical work
• Staffing • Training • Supplies
• Physical building • Education
• Measurement

PROTOCOLS CONTINUED
Use guidelines as a shared baseline with clinicians free to vary based on individual patient needs Measure and learn from and (over time) eliminate variation from professionals; retain variation arising from patients

PRACTICAL LIMITATIONS ON PROTOCOL USE
When abstract guidelines hit real patient care, experience clearly shows
No protocol fits every patient
More importantly
No protocol perfectly fits any patient

HEALTHCARE IS CHANGING From
Craft Based Practice • Individuals, working alone, • Handcrafting a customized solution for each patient • Based on a vast personal knowledge gained from training and experience
To
Professional based practice • Groups of peers, treating similar patients in a shared setting • Plan coordinated care delivery processes • Which are adaptable to specific patient needs

WHAT ARE THE BENEFITS? 1.It produces better outcomes for our patients
2. It eliminates waste, reduces costs and increases available
resources for patient care
3.It puts healthcare professionals in control of care delivery
4.It is the foundations for useful electronic data collection

WE ARE ALL READY DOING THIS AREN’T WE
Insufficient evidence for most treatment choices Expert opinion is essentially random Practice guidelines don’t change practice Most guidelines lack sufficient evidence to actually guide practice Most guidelines have no validation data

IMPROVING QUALITY
Eliminate inappropriate variation
(process steps)
Document continuous improvement (outcomes)

MIN MAX RANGE MEDIAN MEAN CASES OUTLIERS DAYS
OVERSTAYED
F62A 1 44 43 days 6 8.7 128 8 263
F62B 1 40 39 days 3 3.7 227 7 145
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44
LOS (days)
F62B
F62A
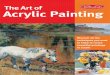
Distribution of LOS - DRG F62
An example of how we are examining variation as part of process redesign

75%
05
10
15
20
Fre
qu
en
cy
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46
los
Distribution of days of stay - F62A25% 50%
• 25% of patients stay between 1-3 days.
• 25% of patients stay between 3-6 days
• 25% of patients stay between 6-11 days
• 25% of patients stay between 11-44 days
Heart Failure
020
40
60
Fre
qu
en
cy
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
LOS (days)
Distribution of days of stay - F62B25% 50%
75%
• 25% of patients stay between 3-5 days
• 25% of patients stay between 5-40 days
• 25% of patients stay 1 day.
• 25% of patients stay between 1-3 days

First Second Third Fourth Total
Total Separations 32 32 32 32 128
Total Bed Days 58 (5.2%) 131 (11.8%) 256 (23.1%) 664 (59.9%) 1109
Mean Age 80.0 80.2 76.1 79.4 78.9
Male % 46.9% 59.4% 50.0% 59.4% 53.9%
Variation in LOS 1-3 3-6 6-11 11-44 1-44
Admissions
in 12 months
One 22 22 24 22 90 (70.3%)
Two 9 8 7 8 32 (25%)
Three 1 2 1 2 6 (4.7%)
Heart Failure
25% of patients accounted for 59.9% of bed days. If all 32 of the cases in the fourth quartile could
be reduced to 11 days stay (the maximum of the third quartile – effectively making 11 days the
maximum LOS for DRG F62A) a total of 312 bed days could be saved within this DRG^.
Multiple admissions for same patients during the 2012/13 period:
• 70.3% = single admission
• 25.0% = two admissions
• 4.7% = three admissions
The number of prior admissions remained equal within all quartiles, meaning there is no association
between multiple admissions and longer LOS. ^(Current 664 days minus (32 cases * 11 days = 352 days) = 312 bed days saved)

First Second Third Fourth Total
Total Separations 32 32 32 32 128
Comorbidities 32 (100%) 32 (100%) 32 (100%) 32 (100%) 128 (100%)
Heart 30 (93.8%) 32 (100%) 32 (100%) 32 (100%) 126 (98.4%)
Hypertension 16 (50%) 17 (53.1%) 8 (25.0%) 10 (31.3%) 51 (39.8%)
Diabetes Type 1 - 1 (3.1%) - - 1 (0.8%)
Diabetes Type 2 14 (43.8%) 21 (65.6%) 18 (56.3%) 14 (43.8%) 67 (52.3%)
Renal 2 (14.3%) 9 (42.9%) 9 (50.0%) 5 (35.7%) 25 (37.3%)
Diabetic Neuropathy 7 (50.0%) 9 (42.9%) 14 (77.8%) 7 (50.0%) 37 (55.2%)
Ophthalmology 1 (7.1%) 7 (33.3%) 2 (11.1%) 4 (28.6%) 14 (20.9%)
Diabetic Ulcers - - 4 (22.2%) 1 (7.1%) 5 (7.5%)
Diabetic Hypoglycaemia 3 (21.4%) 2 (9.5%) 3 (16.7%) - 8 (11.9%)
Lactic Acidosis - - 1 (5.6%) - 1 (1.5%)
Peripheral Angiopathy 2 (14.3%) 2 (9.5%) 3 (16.7%) 1 (7.1%) 8 (11.9%)
Multiple micro-vascular complications - 4 (19.0%) 9 (50.0%) 4 (28.6%) 17 (25.4%)
Other Diabetic Complications 1 (7.1%) 2 (9.5%) 4 (22.2%) 7 (50.0%) 14 (20.9%)
Heart Failure
The number of co-morbidities did not change significantly between quartiles for F62A, with all patients
experiencing at least one co-morbidity.

T a i l a n a l y s i s
. . . a s s u m e s t h a t , i f s e r i o u s f a i l u r e s a r e
i n s p e c t e d a n d e l i m i n a t e d , w h a t r e m a i n s
i s s o m e h o w e x c e l l e n t . . .

F o c u s o n t h e T a i l
b e t t e r w o r s e
Q u a l i t y
Q A t h r e s h o l d ( s t a n d a r d )
AB
Fr
eq
ue
nc
y
(#
o
f
pr
ov
id
er
s
at
ta
in
in
g
a
pa
rt
ic
ul
ar
q
ua
li
ty
l
ev
el
)
` a c c e p t a b l e ' q u a l i t y ` u n a c c e p t a b l e ' q u a l i t y

T r a d i t i o n a l Q u a l i t y A s s u r a n c e
w o r s eb e t t e r
w o r s eb e t t e r
Q u a l i t y
Q u a l i t y
t h r e s h o l d
B e f o r e
A f t e r

Q u a l i t y I m p r o v e m e n t
w o r s eb e t t e r
w o r s eb e t t e r
Q u a l i t y
Q u a l i t y
B e f o r eA f t e r

Better has no Limits

Questions


















![Automating Verification of State Machines with Reactive ... · 2 Simon Foster et al. RoboChart [1,23] is a diagrammatic language for the description of robotic controllers with denotational](https://img.pdfslide.net/doc/110x75/60e39494d9393942a254d1df/automating-verification-of-state-machines-with-reactive-2-simon-foster-et-al.jpg)