Embed Size (px)
Citation preview


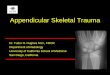
Plain RadiographsFirst modality
NM Bone ScanOccult # e.g femoral neck ,
scaphoid+ve scan may not be seen for 24
hrs after injury

HRUSJoints Soft tissuesBones e.g rib #

• Multislice CT Scanless time consuming and offer
good assessment of bones in 2d and 3d manner
Give volume of information
• MRImod of choice for inj of and
around joints soft tissue detail

• FRACTURE–Break in the continuity of the bone

– CLOSED #=== covered with skin
–OPEN #===== obvious protrusion of bone fragments beyond soft tissue margins
absence of bone piecesgross soft tissue disruption
extending to bone surface subcutaneous gasforeign material within the #


• SINGLE # LINE• Transverse• Oblique • Spiral
• MORE THAN 1 # LINE• Comminuted #-----contains the butterfly
fragment



COMPLETE #
INCOMPLETE #•In bones having greater resilience in children

THREE TYPES•Plastic #---bending or acute angulation of bone with no cortical disruption•Torus or buckle #---# of cortex on compressive side of bone while the cortex on tension side remains intact•Greenstick #----converse of torus #


AP (A, C) and lateral (B, D) radiographs of the right forearm demonstrate a buckle fracture (arrows) of the distal radial metaphysis without significant angulation. Buckle fractures (or torus fractures) are an impaction type of fracture identified by a focal widening (or outward buckling) of the cortex


• SEGMENTAL #• segment of bone is isolated by #s
at each end


APPOSITION•The position of major fragments with respect to each other
DISTRACTION•Non apposed fragments and when the displacement is along the long axis


• Description is according to the direction of displacement of the distal fragment distal fragment relative to the proximal

IMPACTION•When bone fragments are driven into each other
ABNORMALITY OF ROTATION•Of the distal fragment•Both ends of the same bone should be checked in the same film

• ANGULATION• Direction of the apex of the angle at the #
site
• Varus angulation --angulation of distal fragment towards the midline
• Valgus angulation-- angulation of distal fragment away from the midline


CLUES TO #•Joint effusion / hemarthrosis---# around a joint----e.g. elbow
•Fat-Fluid level(lipohemarthrosis)---knee joint #


Paravertebral soft tissue shadowing (DD PV abscess) due to hemorrhage in thoracic spine #
Soft tissue swelling in retropharyngeal spacecervical spine trauma


Delayed union
•Poor apposition or inadequate stabilization
•Vit C Deficiency•Infection•Age—decreased osteoblastic activity•Underlying skeletal pathology

Non union
•Idiopathic (tibia)•Poor stabilization•Infection•Pathological #•Massive initial trauma

Malunion
•Healing in unsatisfactory anatomical position•Excessive fragment overlap ----shortening•Unsatisfactory angulation•Displacement


Dislocation •Complete loss of normal articular contact btw the bones comprising the joint
Subluxation•Partial loss of articular contact
Diastasis•Separation of fibrous joints—SI , pubic symphysis



Avulsions ----indicator of ligamentous injury
•Base of proximal fragment of the thumb•Avulsion of medial lateral maleoli


STRESS #s
•Chronic repetitive insufficient forces•Sites are characteristic•March # of 2nd and 3rd MT heads•# of proximal fibula in paratroopers

NM---increase activity before radiographic signs
RADIOGRAPH---sign depends upon stage of healing e.g lucent line to new bone formation

Bilateral stress fracture of the distal fibula: Initial radiographs and Bone scintigraphy at 2 weeks follow up.

Pathological #
•In bones weakened by underlying disease•E.g. osteoporosis , osteomalacia , bone tumors


Post traumatic AVN
•Femoral neck •Proximal pole of scaphoid
•Necrotic bone is denser•Disuse cause surrounding osteopenia

Drillers disease / vibration syndrome
•Use of vibrating machines 5-10 yrs usage
•Degenerative cysts in bones of hand and wrist

Post traumatic myositis ossificans•Ossification of hematoma or periosteal elements which are displaced into the soft tissue. •Commonest site is thigh•DD---Parosteal osteosarcoma•Radiograph•MRI•Biopsy

Post-traumatic myositis ossificans. A well-defined bone density arises from the cortex of the distal femur and extends into the soft tissues. There was a history of blunt trauma, but even so, this lesion needs to be differentiated from parosteal osteosarcoma.

Compartment syndrome
•In areas of the limbs surrounded by rigid osseous and fascial planes•Skeletal trauma—hemorrhage / edema---rising pressure•Progressive ischemia -----necrosis

Vascular injury•Penetrating trauma / bone fragments•Supracondylar #brachial artery•Knee 3 / dislocationPopliteal artery•Pelvic ring #branches of internal iliac artery
•Spiral CT –superior to angiography

Traumatic avulsion of the right superior gluteal artery (arrow) from pelvic trauma. Bleeding from branches of the internal iliac artery is also seen (open arrows). Marked diastasis of the right sacroiliac joint has occurred.

Post traumatic reflex dystrophy / reflex sympathetic dystrophy / Sudecks atrophy
•Injury to limb—intense pain and swelling—severe disuse osteoporosis

Sudeck's atrophy: there was minor trauma to the forearm some weeks earlier. Note gross osteoporosis of the bones of the hand, wrist and forearm, most marked at the bone ends, but also causing cortical 'thinning' and resorption

Ionizing radiation
•Osteonecrosis at the site of insult•Patchy sclerosis with spontaneous # •secondary malignant degeneration to osteosarcoma after 5 yrs or so

Frost bite•Acro-osteolysis •Premature epiphyseal closure and growth arrest in children

Frostbite > acro-osteolysis of the toes, with almost complete resorption of the distal phalanges.

Caissons disease
•In deep sea divers and tunnel workers•Poor decompression----nitrogen bubbles in blood----capillary blockage•Avascular necrosis•Irregular bone densities usually in long bones•Medullary infarctions •NM and MRI detect changes earlier

Avascular necrosis of the hips. Note mixed sclerosis and lucency of the femoral heads, with collapse of the weight-bearing surface but maintenance of the joint spaces, indicating intact articular cartilage.

THANKS