Embed Size (px)
DESCRIPTION
We in Chinthamani Laser Dental Clinic & Implant Centre ,cover every speciality and subspeciality in dentistry so that all kind of your dental problems can be treated efficiently and effectively. Contact us: Chinthamani Laser Dental Clinic & Implant Centre 1/464,Mount Poonamallee High Road, Iyyapanthangal, Chennai-56 Phone no.044-43800059 , 92 83 786776 Email: [email protected], [email protected] Website: www.chinthamanilaserdentalclinic.com
Citation preview

SOFT TISSUE ORAL SOFT TISSUE ORAL LESIONS IN CHILDRENLESIONS IN CHILDREN
Chinthamani Laser Dental Clinic

Drug induced gingival Drug induced gingival hyperplasia (PIGO)hyperplasia (PIGO)
Also known as phenytoin induced gingival Also known as phenytoin induced gingival overgrowth.overgrowth.
Dilantin hyperplasia.Dilantin hyperplasia.ETIOLOGY: MultifactorialETIOLOGY: Multifactoriala)a) Disturbance in adrenocortical functionDisturbance in adrenocortical functionb)b) Local response to metabolic products of phenytoin in Local response to metabolic products of phenytoin in
salivasalivac)c) Direct action on phenytoin on fibroblast.Direct action on phenytoin on fibroblast. It is related to the efficacy of oral hygiene and, thus It is related to the efficacy of oral hygiene and, thus
to the amount of plaque, and inadequate amounts of to the amount of plaque, and inadequate amounts of antimicrobial factors in the oral cavity could antimicrobial factors in the oral cavity could contribute to greater plaque accumulation.contribute to greater plaque accumulation.

Clinical featuresClinical features
Appears as early as 2 to 3 weeks after initiation of Appears as early as 2 to 3 weeks after initiation of drug therapy, peaks at 18 to 24 months.drug therapy, peaks at 18 to 24 months.
Painless enlargement of interproximal gingiva.Painless enlargement of interproximal gingiva. The buccal & anterior segment are more affected than The buccal & anterior segment are more affected than
the lingual & posterior segments.the lingual & posterior segments. Gingiva appears pink and firm Gingiva appears pink and firm Does not bleed on probing.Does not bleed on probing. Lesion is purely fibrotic in nature or…Lesion is purely fibrotic in nature or… Secondary infection superimposes and combined type Secondary infection superimposes and combined type
of inflammatory enlargement ensues.of inflammatory enlargement ensues.

Clinical featuresClinical features
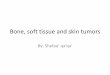
As interdental As interdental lobulations grow, lobulations grow, clefting becomes clefting becomes apparent at the midline apparent at the midline of tooth.of tooth.
Lobulations coalesce at Lobulations coalesce at the midline forming the midline forming pseudopockets and pseudopockets and covering most of crown covering most of crown toothtooth

TREATMENTTREATMENT
Symptomatic treatment:Symptomatic treatment:-Antihistamines -Antihistamines -Topical steroids-Topical steroids-Folic acid-Folic acid-Ascorbic acid-Ascorbic acid-Topical antibiotics-Topical antibiotics-Alkaline mouth washes-Alkaline mouth washes Vigorous gingival massage coupled with efficient Vigorous gingival massage coupled with efficient
tooth brushing and gum stimulators.tooth brushing and gum stimulators.

TreatmentTreatment
Surgical approach:Surgical approach: Gingivectomy with Gingivectomy with
periodontal knives.periodontal knives. LaserLaser ElectrosurgeryElectrosurgery Internal bevel flap Internal bevel flap
surgerysurgery

CONDITIONED ENLARGEMENTSCONDITIONED ENLARGEMENTS
Occurs when the systemic condition of the Occurs when the systemic condition of the patient exaggerates or distorts the normal patient exaggerates or distorts the normal response to the dental plaque.response to the dental plaque.
Includes:Includes:
Pubertal gingivitisPubertal gingivitis
Non-specificNon-specific
Nutritional Nutritional
AllergicAllergic

Hormonal (pubertal gingivitis)Hormonal (pubertal gingivitis)
ETIOLOGY:ETIOLOGY: Hormonal changesHormonal changes
Direct effect on perio. tissue metabolismDirect effect on perio. tissue metabolism
Permeability of the vascular systemPermeability of the vascular system
Microbiota react specifically to availability of Microbiota react specifically to availability of hormones in oral fluids. hormones in oral fluids.

Clinical featuresClinical features
Circumpubertal enlargementCircumpubertal enlargement SexSex: both in males and females: both in males and females Appears in areas of local irritationAppears in areas of local irritation SizeSize of gingival enlargements far exceeds that of gingival enlargements far exceeds that
usually seen in comparable local factors.usually seen in comparable local factors. After puberty, the enlargement undergoes a After puberty, the enlargement undergoes a
spontaneous reduction.. But does not disappear spontaneous reduction.. But does not disappear until local factors are removed. until local factors are removed.

Treatment Treatment
Removing sources of irritationRemoving sources of irritation
ScalingScaling
CurettageCurettage
Surgical removal in severe casesSurgical removal in severe cases

NUTRITIONAL(SCURVY)NUTRITIONAL(SCURVY)
ETIOLOGYETIOLOGY Deficiency of Deficiency of
vitamin cvitamin c

Clinical featuresClinical features Gingiva :Gingiva : -bluish red -bluish red -soft and friable-soft and friable -smooth shiny surface-smooth shiny surface Spontaneous Spontaneous hemorrhagehemorrhage
on slight provocationon slight provocation Surface necrosis with Surface necrosis with
pseudomembrane pseudomembrane formationformation
Enlarged tissue cover the Enlarged tissue cover the clinical crownclinical crown
Typical Typical foul breathfoul breath with with fusospirochetal stomatitisfusospirochetal stomatitis
Superinfection Superinfection leading to leading to ulceration and necrosis of ulceration and necrosis of papillaepapillae

Treatment Treatment Ingestion of vit. C Ingestion of vit. C
tabletstablets Diet rich in citrus Diet rich in citrus
fruitsfruits Oral Oral prophylaxis prophylaxis Maintainence of good Maintainence of good
oral hygieneoral hygiene

Non specific enlargements Non specific enlargements (granuloma pyogenicum)(granuloma pyogenicum)
The lesion varies from a The lesion varies from a discrete spherical , discrete spherical , tumour like mass with a tumour like mass with a pendulated attachment to pendulated attachment to a flattened , keliod like a flattened , keliod like enlargement with a broad enlargement with a broad base.base.
Bright red , Bright red , Either friable or firm, Either friable or firm, surface ulceration surface ulceration Purulent exudation Purulent exudation

Treatment Treatment
Removal of lesionRemoval of lesion Eliminating irritating local factorsEliminating irritating local factors

Allergic (plasma cell gingivitis)Allergic (plasma cell gingivitis)
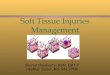
The use of drugs may The use of drugs may evoke an allergic evoke an allergic rasponse manifested as rasponse manifested as an inflammatory an inflammatory reaction.reaction.
May be associated with May be associated with generalised allergic generalised allergic response.response.
The gingival and buccal The gingival and buccal mucosa on the left side show mucosa on the left side show pronounced erythema and pronounced erythema and slight swelling. Diffuse slight swelling. Diffuse ulcerations can also be seen.ulcerations can also be seen.

The inflammatory infiltrate is composed predominately of plasma cells (He x 400).

Treatment Treatment
Stoppage of drugs generally reverses this Stoppage of drugs generally reverses this condition.condition.
Anti – allergic drugs are of help.Anti – allergic drugs are of help.

Juvenile periodontitis Juvenile periodontitis
Uncommon form of severe periodontal disease Uncommon form of severe periodontal disease belonging to a group termed as anbelonging to a group termed as an
EARLY ONSET AGGRESSIVE PERIODONTAL EARLY ONSET AGGRESSIVE PERIODONTAL DISEASE.DISEASE.
Described by Wannenmacher(1938)Described by Wannenmacher(1938) AgeAge: teenagers: teenagers 3 3 typestypes of disease: of disease:
a) chronic slowly progressive a) chronic slowly progressive
b) fairly generalizedb) fairly generalized
c) acute progressive and more generalc) acute progressive and more general

Etiology Etiology
PMN dysfunctionPMN dysfunction
Susceptibility to infectionSusceptibility to infection
A. ActinomycetemcomitansA. Actinomycetemcomitans
Serum amplification leukotoxin antibody neutralisationSerum amplification leukotoxin antibody neutralisation
Local PMN & macrophage destructionLocal PMN & macrophage destruction
Accelerated diseaseAccelerated disease

Clinical featuresClinical features
Loss of attachmentLoss of attachment
Bone loss(3-4 times)Bone loss(3-4 times)
Mobility of teethMobility of teeth
Denuded root surfaceDenuded root surface
Periodontal abscessPeriodontal abscess

Clinical features (cont.)Clinical features (cont.) Teeth involved: permanent incisors and first molars.Teeth involved: permanent incisors and first molars. The attack sequence appear to follow eruption The attack sequence appear to follow eruption
chronology.chronology. Most striking feature : Lack of clinical inflammation Most striking feature : Lack of clinical inflammation
despite the presence of deep pockets.despite the presence of deep pockets. Starts as a localized form Starts as a localized form
if not treated if not treated generalized formgeneralized form

Clinical features (cont.)Clinical features (cont.)
Advanced bone loss in the primary dentition Advanced bone loss in the primary dentition does exit but without destinctive localization.does exit but without destinctive localization.
Every third case presents with Every third case presents with lymphadenopathylymphadenopathy
Clinically only thin layer of plaque is presentClinically only thin layer of plaque is present Classically, distolabial migration of the Classically, distolabial migration of the
maxillary incisorsmaxillary incisors
Diastema formationDiastema formation

Radiographic findingsRadiographic findings
•A full mouth series of radiographs would be beneficial in this case rather than routine bite wing x-rays.
• Bilateral bone loss is discovered around all first molars and incisors.
• Vertical bony defects are Characteristic in LJP.

Treatment Treatment
Root resectionRoot resection Subgingival irrigation Subgingival irrigation
with iodine and hydrogen with iodine and hydrogen peroxide.peroxide.
Scalling and root planingScalling and root planing Tetracycline is antibiotic Tetracycline is antibiotic
of choiceof choice Oral hygiene Oral hygiene
maintainencemaintainence Bone graftingBone grafting

Preoperative and post operativePreoperative and post operative

Papillon lefevre syndrome Papillon lefevre syndrome Described by : Papillon and LefevreDescribed by : Papillon and Lefevre Characterized by hyperkeratosis of palms and soles + Characterized by hyperkeratosis of palms and soles +
precocious periodontal destruction and shedding of the precocious periodontal destruction and shedding of the deciduous and permanent dentition.deciduous and permanent dentition.
ETIOLOGY:ETIOLOGY: Suggested to be due to Suggested to be due to 1.1. Defective local Defective local vitamin Avitamin A metabolism metabolism2.2. Deep subgingival flora assocaited with PLS is composed of Deep subgingival flora assocaited with PLS is composed of
great no. of motile, gram –ve great no. of motile, gram –ve anaerobic rodsanaerobic rods , including , including bacteroids gingivalis and capnocytophagia.bacteroids gingivalis and capnocytophagia.
3.3. Cellular Cellular immune defectimmune defect with a decreased stimulation of with a decreased stimulation of lymphocytes.lymphocytes.
4.4. Now generally accepted as the Now generally accepted as the homozygosity of autosomal homozygosity of autosomal recessive genes.recessive genes.

Clinical featuresClinical features
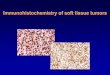
a)a) Skin lesions: Skin lesions: start b/w start b/w first and fourth year first and fourth year after birth.after birth.
Hyperkeratotic lesions Hyperkeratotic lesions of palms and soles of palms and soles bilaterally.bilaterally.
Hyperkeratosis is Hyperkeratosis is usually progressive usually progressive and becomes dry and and becomes dry and scaly.scaly.

Clinical featuresClinical featuresb)b) Dental signs and symptomsDental signs and symptoms:: Swollen gingiva, migration Swollen gingiva, migration
and mobility of teethand mobility of teeth PocketsPockets Fetor-ex-orisFetor-ex-oris Painless exfoliationPainless exfoliation By 3.5 to 4.5 years all the By 3.5 to 4.5 years all the
deciduous teeth are lost.deciduous teeth are lost. Eruption of permanent Eruption of permanent
enhancedenhanced Disease progress recycles & Disease progress recycles &
by ages 13-14 & all by ages 13-14 & all permanent teeth exfoliated.permanent teeth exfoliated.

Radiographic findingsRadiographic findings
Severe horizontal Severe horizontal alveolar bone loss.alveolar bone loss.
Alveolar bone and basal Alveolar bone and basal bone resorbs beyond bone resorbs beyond apices of roots.apices of roots.
Incomplete root Incomplete root resorption.resorption.

Treatment Treatment
Vitamin C metabolitesVitamin C metabolites (retinoids):are involved (retinoids):are involved in regulation of growth and differentiation of in regulation of growth and differentiation of the epithelial cells. Profound effect on the epithelial cells. Profound effect on keratinization by dec. the total keratin content keratinization by dec. the total keratin content of the keratinocytes.of the keratinocytes.
Antbiotics Antbiotics