Embed Size (px)
DESCRIPTION
ecg
Citation preview

INTERESTING ECGSModerator- Dr. Thomas JohnPresenter-Dr. Pradeep katwal

ECG included
• SINUS EXIT BLOCK type II• Anteroseptal wall myocardial infraction• SVT with aberrant conduction• WPW syndrome• Inferior wall MI with right ventricular extension• Burgada syndrome• Acute pericarditis• Takasubo cardiomyopathy• Hypothermia• CAD with single vessel disease presenting initially with
complete heart block and later with SVT.

rca gpcr.pptx

What is ECG?
• ECG is graphical recording of electrical activity of heart from body surface using multiple electrode placed over the body.

The Normal Conduction System

All Limb Leads

Precordial Leads

Interpretation
• Systematic approach to reading EKGs :
• Rate
• Rhythm (including intervals and blocks)
• Axis
• Hypertrophy
• Ischemia

Waveforms
The electrical pattern of the cardiac cycle shows waves and intervals.

Electrical axis deviation of heart

Case 1
• 68 ys old male presented in emergency with history of progressive shortness of breath and generalized swelling of body.
• Vitals– Pulse-32/min– B.P.-90/60 mm hg


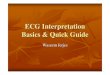
INTITIAL ECG

• SINUS EXIT BLOCK type II
• PP intervals fairly constant (unless sinus arrhythmia present) until conduction failure occurs
• The pause is approximately twice the basic PP interval

• 2ND DEGREE AV BLOCK

• S.creat: 4.5 mg%• S. potassium: 7.1 mEq/l• Urea : 164 mg/dl
• DIGNOSIS- CHRONIC KIDNEY DISEASE SATGE 5-METABOLIC ACIDODIS, HYPERKALEMIA, ANEMIA OF CHRONIC DISEASE


CASE 2
• 76 Yrs old male, emergency• C/O – Epigastric pain * 2 days– Vomiting *2 episodes
• Vitals– Pulse-72/min– B.P.-100/68 mmhg

Initial ECG

At 12 p.m.
• Call was given for sudden onset shortness of breath.– pulse rate- 280/min
• ECG showed-

ecg2

VT versus SVT with aberrancy
• Very broad complexes (>160ms)• A V dissociation • Capture beats • Fusion beats Positive or negative concordance throughout
the chest leads, i.e. leads• V1-6 show entirely positive (R) or entirely negative (QS)
complexes, with no RS complexes seen.• Brugada’s sign – The distance from the onset of the QRS
complex to the nadir of the S-wave is > 100ms• Josephson’s sign – Notching near the nadir of the S-wave• RSR’ complexes with a taller left rabbit ear .



• Angiography-coronary artery disease, single vessel disease-Right coronary artery occlusion
• Stenting was done with BMS

ECG3

Case 3
16 yrs old male without significant past medical history presented with H/O palpitation on and off.
Vitals• Pulse-76/min

ECG2


ECG criteria include all of the following
Short PR interval (<0.12s)
Initial slurring of QRS complex (delta wave) representing early ventricular activation through normal ventricular muscle in region of the accessory pathway
Prolonged QRS duration (usually >0.10s)
Secondary ST-T changes due to the altered ventricular activation sequence


ECG1

AVRT With Orthodromic Conduction
• Rate usually 200 – 300 bpm.• Wide QRS complexes due to abnormal
ventricular depolarisation via accessory pathway.

CASE 4
• 68 yrs old male –Chest pain since 4 HOURS–a/w Shortness of breath, vomiting
Vitals–Pulse-86 JVP-raised–B.P.-100/60 mmhg

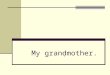
ECG 1

observe
• ST elevation in V1• ST elevation in lead III > lead I

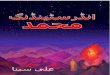
ECG 2
• RIGHT SIDE ECG

• Right ventricular infarction is confirmed by the presence of ST elevation in the
right-sided leads (V3R- V6R).
The most useful lead is V4R, which is obtained by placing the V4 electrode in the 5th right intercostal space in the midclavicular line.


Right venticular infraction on EKG
ST elevation of 1 mm or more in lead V1 and lead V4R.
Failure of development of reciprocal changes in right precodial leads.
Decrease in magnitude of ST elevation in leads V1-V5
Discordant relationship of ST changes(ST elevation in lead V1 and depression in lead V2)

CASE 5
• 34 YRS OLD HYPERTENSIVE MALE– ASYMPTOMATIC– DURING ROUTINE CHEAK UP

Diagnosis

Burgada syndrome
St-segment elevation in V1–V3 in sinus rhythm
Elevated ST segment (≥2 mm) descends with
an upward convexity to an inverted T wave
Provoked with the sodium channel-blocking
drugs
Risk of polymorphic ventricular arrhythmias

CASE 6• 19 ys/F, with 5 days history of central chest pain and
fever. Her pulse rate was 74 beats/min and her ECG showed-


EKG Manifestations of Acute pericarditis
Sinus tachycardia
Taller, Peaked and symmetrical T waves
Elevated Concave upwards S-T segment
without reciprocal changes
The PR segment elevation on lead AVR.

• Stage Ieverything is UP (i.e., ST elevation in almost all leads - see below)
• Stage IITransition ( i.e., "pseudonormalization").
• Stage IIIEverything is DOWN (inverted T waves).
• Stage IV Normalization

Case -7
• 63 year old lady is brought Emergency with central crushing chest pain.
• She has no previous medical history and was in the mortuary to see the body of her son who’d just died from a subarachnoid haemorrhage..

ECG

She’s taken to angiography where she’s found t o have normal coronary arteries.

Mayo Clinic criteria for tako-tsubo cardiomyopathy
1. New ECG changes (St elevation or T wave inversion) or moderate troponin rise.2. Transient akinesis / dyskinesis of left ventricle (apical and mid-ventricular segments) with regional wall abnormalities extending beyond a single vascular territory.3. Absence of coronary artery stenosis >50% or culprit lesion.

Left ventriculogram

CASE 8
• 45 yrs old male, following exposure during a cold winter night as a result of alchohol intoxication was brought to ER.

ECG

• Sinus Bradycardia• Low amplitude P waves• Increased venticular activation time• HUMP LIKE DEFECTION of the distal limb of
QRS complex with S-T segment: OSBORN W AVES
• Prolonged Q-Tc interval



Thank you