Embed Size (px)
Citation preview

Acute Coronary Syndrome(ACS)
Prof. Dr. M Zak Khalil, MD,FACC, FESC, FAHA, FKSUProfessor of MedicineConsultant Interventional Cardiologist

Contents
• Definitions• Assessment• Treatment• Discussion

Ischemic symptoms (Angina)
• Dull sub-sternal discomfort variably described as a pressure or tightness
• Radiating to the left arm, neck, or jaw• Associated with nausea, vomiting,
sweating, shortness of breath, or palpitations.
• Precipitated by stress• Relieved by rest or nitroglycerin SL

Angina-equivalent(No pain)
• Lightheadedness• Shortness or breath• Nausea• Faintness• Cold sweat

Coronary arteries.

Mechanical obstruction
Thrombus
Dynamic obstruction
Development of Coronary artery disease


Circulation. 2001;104:365-372
Atherosclerosis Unstable angina MI
ACSThrombosis

Unstable Angina (UA)
• Ischemic symptoms (history) • No ST elevation or new Q waves (EKG) • A normal serum CK-MB (enzymes)
WHO task force. Circulation 1979

Unstable Angina (UA)
• Ischemic symptoms suggestive of an ACS• No elevation in troponins or CK-MB• With or without ECG changes indicative of
ischemia (ST segment depression or transient elevation or new T wave inversion)
The Joint ESC/ACC Committee.



Major Role of Platelets in ACS
Activated platelets
• Adhesion1
• Activation2
• Aggregation3
Plaquerupture
FibrinogenTxA2
ADP
Platelets
ADP = adenosine diphosphateTxA2= thromboxane A2

Plaque rupture Fibrinogen-mediated platelet aggregation
Platelet-rich thrombusformation and vessel occlusion
Acute coronarysyndrome
FibrinogenGP IIb/IIIa receptorFibrin
Key to figures
Platelet adhesion & activation
Platelet Adhesion and Aggregation

CK- MB or Troponin Troponin elevated or not
ACS without persistent
ST-segment elevation
ACS with persistent ST-segment elevation

ACS


MI (acute, evolving, or recent) ESC/ACC/AHA 2012
Typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis with at least one of the following:
• Symptoms of ischemia• New (or presumably new) significant ST/T wave
changes or LBBB• Development of pathological Q waves on ECG• Imaging evidence of new loss of viable myocardium or
regional wall motion abnormality• Identification of intracoronary thrombus by angiography
or autopsy

0 1 2 3 4 5 6 78
Cardiac troponin-no reperfusion
Days After Onset of STEMI
Mul
tiple
s of t
he U
RL
Upper reference limit1
2
5
10
20
50
URL = 99th %tile of Reference Control Group
100
Cardiac troponin-reperfusion CKMB-no reperfusion CKMB-reperfusion
Cardiac Biomarkers in STEMI
Alpert et al. J Am Coll Cardiol 2000;36:959.Wu et al. Clin Chem 1999;45:1104.

NSTEMI
• NSTEMI = UA + myocardial damage
(as evidenced by release of detectable quantities of a marker of myocardial injury).

Acute coronary syndromes
Unstable angina (UA) Myocardial infarction
Stable angina NSTEMI STEMI

Ischemic Discomfort at Rest
No ST-Segment Elevation
NSTEMIUnstable Angina
STEMI
ST-Segment Elevation
( : positive cardiac biomarker)
EmergencyDepartment
In-Hospital
Presentation
Spectrum of Acute Coronary Syndromes

European Survey of Acute Coronary Syndromes:the ENACT Study
05
101520253035404550
UA/non-ST elevation MI Definite MI Suspected ACS
Hos
pita
lizat
ions
(%)
17 Western European countries Fox KA et al. Eur Heart J 2000; 21: 1440–9.

Repeat after GTN

Acute STEMI:Chest pain duration to FMC = 30 min.
SK




• All patients with ACS will receive the same therapy.
• True: • False:

• All patients with ACS will have the same outcome.
• True: • False:

• The mortality rate at one year is higher with NSTEMI than STEMI.
• True:• False:

Mortality STEMI NSTEMI UA
30 days 6.1% 5.7% 2.4%
6 months 8.0% 8.8% 5.0%
1 year 9.6% 11.1% 7.0%
GUSTO-IIb Investigators. Circulation 1998; 98:1860.
Prognosis of ACS

Mortality in Non-ST ACS Patients WithMyocardial Infarction During Hospitalization
Fintel D, ACC, 2000
18.3%
5.5%
12.8%
(P = 0.0001)
Patients with MI within 72 hours (n=593)
Patients without MI within 72 hours (n=8,868)
Days following randomization
% M
orta
lity
30 60 90 120 150 180
20
15
10
5

Assessment
• TIMI risk score• GRACE risk models• Killip class

TIMI risk score
• Age > or =65 years • Presence of at least three risk factors for CHD • Prior coronary stenosis of > or =50 percent • Presence of ST segment deviation on admission
ECG • At least two anginal episodes in prior 24 hours • Elevated serum cardiac biomarkers • Use of aspirin in prior seven days

Mortality & Morbidity(all-cause mortality, new or recurrent MI, or severe
recurrent ischemia requiring revascularization)
• Score of 0/1 – 4.7 % • Score of 2 – 8.3 % • Score of 3 – 13.2 % • Score of 4 – 19.9 % • Score of 5 – 26.2 % • Score of 6/7 – 40.9 %


GRACE risk models
• Age • Killip class • Systolic blood pressure • Presence of ST segment deviation • Cardiac arrest during presentation • Serum creatinine concentration • Presence of elevated serum cardiac biomarkers • Heart rate

Killip class
• Class I - no evidence of HF • Class II - findings consistent with mild to
moderate HF (S3, lung rales less than one-half way up the posterior lung fields, or jugular venous distension)
• Class III - overt pulmonary edema • Class IV - cardiogenic shock

Assessment
• It is essential that initial assessment and management be:
• 1-Rapid• 2-Methodical

Diagnostic evaluation in ER:
• Acute coronary syndrome• Stable angina pectoris• Nonischemic chest pain

All patients with ACS:
• Airway, breathing, and circulation • 12-lead ECG • Resuscitation equipment • Cardiac monitor • Oxygen • IV access and blood work obtained• Aspirin 300 mg • Nitrates and morphine (unless contraindicated)

ST elevation (persistent):
• ST segment elevation > or =1 mm is present in two or more anatomically contiguous leads.
• The elevations are considered to represent ischemia and not pericarditis or left ventricular aneurysm.




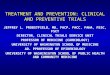
ST elevation:

Coronary angiograms displayed a normal right coronary artery (A), which became totally occluded during the ergonovine provocation test (B).
RCARCA

STEMI (ACS)
• Relief of ischemic pain • Assessment of the hemodynamic state • Clopidogrel • Reperfusion with PCI or thrombolysis • ACE-I (or ARB) • Beta blocker • Statin • Anticoagulation for LV thrombus or chronic
atrial fibrillation to prevent embolization

Thrombolysis and ASA in Acute STEMI: ISIS-2
1. ISIS-2 Collaborative Group. Lancet 1988; 2: 349360.
12.0%
9.2% 9.4%
11.8%13.2%
8.0%
Placebo versusstreptokinase
Placebo versus ASA 162 mg
Neitherversus both
5-w
eek
mor
talit
y (%
)
25%*p <0.00001
23%*p <0.00001
42%*p <0.00001
*Odds reduction; ASA=acetylsalic acid
0
2
4
6
8
10
12
14

PCI versus Fibrinolysis
Favors PCI
Favors fibrinolysis with a fibrin-specific agent
13 RCTsN = 5494 P = 0.04
Abs
olut
e R
isk
Diff
eren
ce in
Dea
th (%
)
30 40 50 60 70 80PCI-Related Time Delay (minutes)
10 −
5 −
0 −
-5 − ┬ ┬ ┬ ┬ ┬ ┬
Nallamothu and Bates. Am J Cardiol 2003;92:824.

Reperfusion
• It is not possible to say definitively that a particular reperfusion approach is superior for all pts, in all clinical settings, at all times
• The appropriate & timely use of reperfusion therapy is more important than the choice of therapy


Assessing Reperfusion Options for Patients with STEMI
STEP 1: Assess time and risk (time from symptom onset, risk of STEMI, risk of thrombolysis, time for transport to PCI lab)
STEP 2: Determine whether fibrinolysis or invasive strategy is preferred*
Antman EM et al. Circulation 2004; 110: 588–636.
Fibrinolysis preferred if: Invasive strategy preferred if:• Early presentation (<3 hours)• Invasive strategy not an option• Delay of invasive strategy
• Skilled PCI lab with surgical backup available
• High risk (i.e. cardiogenic shock)• Contraindications to fibrinolysis• Late presentation (>3 hours)• Diagnosis of STEMI is in doubt
*If presentation is <3 hours from onset and there is no delay to an invasive strategy, there is no preference for either strategy

2013 ACC/AHA Guidelines


















Contraindications and Cautionsfor Fibrinolysis in STEMI
Absolute Contraindications
• Any prior intracranial hemorrhage• Known structural cerebral vascular lesion (e.g.,
arteriovenous malformation)• Known malignant intracranial neoplasm (primary
or metastatic)• Ischemic stroke within 3 months EXCEPT acute
ischemic stroke within 3 hours
NOTE: Age restriction for fibrinolysis has been removed compared with prior guidelines.

Contraindications and Cautionsfor Fibrinolysis in STEMI
Absolute Contraindications
• Suspected aortic dissection• Active bleeding or bleeding diathesis
(excluding menses)• Significant closed-head or facial trauma within
3 months

Contraindications and Cautionsfor Fibrinolysis in STEMI
• History of chronic, severe, poorly controlled hypertension
• Severe uncontrolled hypertension on presentation (SBP > 180 mm Hg or DBP > 110 mm Hg)
• History of prior ischemic stroke greater than 3 months, dementia, or known intracranial pathology not covered in contraindications
• Traumatic or prolonged (> 10 minutes) CPR or major surgery (< 3 weeks)
RelativeContraindications

Contraindications and Cautionsfor Fibrinolysis in STEMI
RelativeContraindications • Recent (< 2 to 4 weeks) internal bleeding
• Noncompressible vascular punctures • For streptokinase/anistreplase: prior exposure (> 5
days ago) or prior allergic reaction to these agents• Pregnancy• Active peptic ulcer • Current use of anticoagulants: the higher the INR,
the higher the risk of bleeding

Primary PCI for STEMI:General Considerations
Patient with STEMI (including posterior MI) or MI with new or presumably new LBBB
PCI of infarct artery within 12 hours of symptom onset
Balloon inflation within 90 minutes of presentation Skilled personnel available (individual performs > 75
procedures per year) Appropriate lab environment (lab performs > 200
PCIs/year of which at least 36 are primary PCI for STEMI)
Cardiac surgical backup available
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

PCI After Fibrinolysis
In patients whose anatomy is suitable, PCI should beperformed for the following:
Objective evidence of recurrent MI
Moderate or severe spontaneous/provocable myocardial ischemia during recovery from STEMI
Cardiogenic shock or hemodynamic instability.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII

Early vs. Late PCI

Hospital CareClopidogrel Therapy
Aspirin + clopidogrel, for up to 1 month*Aspirin + clopidogrel, for up to 12 monthsWithhold clopidogrel for 5-7 days for CABG
* For patients managed with an early conservative strategy, and those who are planned to undergo early PCI

CLopidogrel as Adjunctive ReperfusIon TherapY1
Purpose:To investigate whether clopidogrel would produce greater angiographic and clinical benefits over placebo for patients with acute STEMI treated with fibrinolytics& ASA and other standard care
1. Sabatine MS et al. New Engl J Med 2005; 352 (available at www.nejm.org)

Clopidogrel Improved Coronary Perfusion1
*Based on odds of an occluded infarct-related artery (TFG 0/1), death or MI by angiography for clopidogrel versus placebo (OR: 0.64 [0.53 to 0.76]; p <0.001)
Placebo(n=1739)
Clopidogrel(n=1752)
21.7
15.0
5
10
15
20
25Pr
imar
y en
dpoi
nt*
(%)
36% reduction*p <0.001
1. Sabatine MS et al. New Engl J Med 2005; 352 (available at www.nejm.org)

COX (cyclo-oxygenase)ADP (adenosine diphosphate)TXA2 (thromboxane A2)
CLOPIDOGREL
ASA COX
ADP
ADP
C
GPllb/llla(Fibrinogen receptor)
Collagen thrombinTXA2
Activation
TXA2
ASA
Synergistic Mode of Action with Clopidogrel and ASA
. Schafer AI. Am J Med 1996; 101: 199–209.

Copidogrel in ACS (NSTEMI) CURE
20% RRRp=0.00009n=12,562
Benefits were seen within hours and continued to increase over the 12 months
0 1 2 3 4 5 6 7 8 9 10 11 12Months of follow-up
% of patients with recurrent ischemic event*
0
10
14
12
4
8
6
2
Standard therapy‡
Clopidogrel + standard therapy‡
The CURE Investigators. N Eng J Med August 2001
‡including ASA*cardiovascular death, MI, or stroke


In patients for whom PCI is planned, clopidogrel
should be started and continued:
• ≥ 1 month after bare-metal stent• ≥ 3 months after sirolimus-eluting stent• ≥ 6 months after paclitaxel-eluting stent• Up to 12 months in absence of high risk for
bleeding.

Safety1
Clopidogrel Placebo(n=1733) (n=1719) p value
Primary bleeding endpoint (%)TIMI major 23 (1.3) 19 (1.1) 0.64
Secondary bleeding endpoints (%) TIMI minor 17 (1.0) 9 (0.5) 0.17TIMI major or minor 40 (2.3) 28 (1.6) 0.18 Intracranial hemorrhage 8 (0.5) 12 (0.7) 0.38
Bleeding through 30 days (%)TIMI major 33 (1.9) 30 (1.7) 0.80TIMI minor 27 (1.6) 16 (0.9) 0.12TIMI major or minor 59 (3.4) 46 (2.7) 0.24
1. Sabatine MS et al. New Engl J Med 2005; 352 (available at www.nejm.org)




NSTEMI (ACS)

4.8
10.8
13.8
17.4
0.6
3.9
7.1
10.3
0
5
10
15
20
48 Hours 7 Days 30 Days 180 Days
Dea
th /
MI
(%)
Placebo
Tirofiban
-90%
-68%
P = 0.04 P = 0. 02
Theroux, Am J Car 2001
-49%
P = 0.04
-54%
P = 0.03
Value of GPIIb/IIIa Antagonists (Tirofiban) Upstream in NSTEMI (ACS)- Hospital with out catheterization facilities -

Theroux, Circulation 2000 – Roffi, Circulation 2001
9.3
15.5
19.2
1.2
4.7
11.2
0
5
10
15
20
25
7 Days 30 Days 180 Days
Dea
th /
MI
(%)
-88%
-70%
P = 0.005 P = 0.001
-47%
P = 0.04
Placebo
Tirofiban
Value of Tirofiban upstream in high risk ACS - Diabetics -

EnoxaparinLMWH

Time to First Event (Triple Endpoint):Superior efficacy of enoxaparin maintained to 43 days
UFHEnoxaparin
Days from randomization
% o
f pat
ient
s w
ith e
vent
s
Relative risk reduction 12%P=0.048
19.7%
17.3%
4
8
12
16
20
0 8 16 24 32 40 43
Circulation 1999;100:1593-1601
Triple endpoint, death/myocardial infarction/urgent revascularization UFH, unfractionated heparin
The TIMI 11B Study

25
20
15
10
5
0
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
UFHEnoxaparin
Days from randomization
% o
f pat
ient
s w
ith e
vent
s
P=0.019
P=0.017
Cohen M, et al. N Engl J Med 1997;337:447-52
MI, myocardial infarctionRA, recurrent anginaUFH, unfractionated heparin
Time to First Event over 30 Days: Death, MI, RASuperior efficacy of enoxaparin was maintained to 30 days
The ESSENCE Study

Fondaparinuxin ACS

Action
• Synthetic heparin pentasaccharide• Binds to AT with a higher affinity than the
native pentasaccharide of UFH or LMWH, causing a conformational change in AT that significantly increases the ability of AT to inactivate factor Xa

OASIS 5: Efficacy and Safety of Fondaparinux vs Enoxaparin in ACS
• Fondaparinux is compared to enoxaparin with substantially lower rates of important bleeds.
• At 1- and at 6-month follow-up, the use of fondaparinux is associated with a significant reduction in mortality.
• Strokes were also significantly reduced by fondaparinux.
• Similar results were observed in patients undergoing intervention.
• Therefore, according to the results of the OASIS-5 trial, fondaparinux is the preferred anticoagulant for the treatment of acute coronary syndromes.

Fondaparinux
• Significant advantages compared to enoxaparin in patients with a non-ST elevation ACS
• Reductions in major bleeding during the initial hospitalization
• Reductions in late mortality

Non ST-elevation ACSACS initial management
ECG monitoring, Blood samples
GpIIb/IIIa antagonist first
e.g., Tirofiban
Low risk
Positive Twice negative
DischargeStress test
Fondaparinux or Enoxaparin(or UFH), ASA,
Clopidogrel*, Betablockers, Nitrates
Second troponin measurement
PCI, CABG or medical managementDepending upon clinical and angiographic
features
Followd by Cor. Angiography
High riskTIMI score > 5
infusion of a GP IIb/IIIa receptor inhibitor followed by
(level of evidence A).

Conclusions:
• The key for correct treatment of ACS is proper and swift assessment.
• STEMI needs rapid revascularization.
• Remember not to harm your patients while acting fast!

1) The preferred anticoagulant for the treatment of acute coronary syndrome (ACS) is:A] FondaparinuxB] HeparinC] EnoxaparinD] TinzaparinE] Warfarin
2) The mortality is higher at one year in patients with ACS diagnosed with:A] STEMIB] NSTEMIC] Unstable anginaD] Chronic stable angina
3) The following is/are absolute contraindication for the use of thrombolytics:A] PregnancyB] Active peptic ulcerC] Recent (< 2 to 4 weeks) internal bleedingD] Suspected aortic dissectionE] Any prior intracranial hemorrhage

4) Clopidogrel is indicated in the following ACS:A] STEMIB] NSTEMIC] Unstable anginaD] Patients who are candidates for CABGE] None of the above
5) All patients with ACS should proceed for coronary angiogram.A] TrueB] False
6) All patients with ACS should be administered GPIIb/IIIa antagonist.A] TrueB] False
7) CABG remains the standard of care for patients with three-vessel or left main coronary artery disease, since the use of CABG, as compared with PCI, resulted in lower rates of the combined end point of major adverse cardiac or cerebrovascular events at 1 year. (NEJM Feb.19, 2009).A] TrueB] False