Embed Size (px)
Citation preview

STEROIDSLyndon Woytuck
MBBS ProgrammeSheba Medical Center, SGUL at UNIC

Introduction to steroids
• Brief review of physiology• Mechanisms of action• Common uses and indications• Adverse effects and alternative treatment• HPA axis suppression and tapering

What are steroids?
• Steroids are endogenous hormone products of the body which have an affect on the expression of gene products by acting within the nucleus• By binding to intracellular receptors, they form hormone-
receptor complexes and act as transcription factors• Commonly prescribed steroids are synthetic, including
mineralocorticoids and glucocorticoids• Androgens (AKA anabolic) have a high potential for abuse, but
may be prescribed in disorders of sexual differentiation or sex transition (muscle mass, libido, sense of well being)

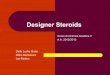
Adrenal Gland

Mineralocorticoids
• Maintain salt and fluid balance• Increase resorption of Na+ and water • Increase excretion of K+ (Na+/K+ ATPase in tubules, eccrine, salivary, colon)
• Aldosterone is primary driver• Cortisol has some small effect at mineralocorticoid receptors• Spironolactone is an aldosterone receptor antagonist
• Indicated in primary hyperaldosteronism, edematous liver cirrhosis or nephrotic syndrome, essential HTN, CHF, and hypokalaemia
• Indicated for NYHA class II/IV heart failure (provided CrCl >30 mL/min and serum K <5 mEq/dL)
• A/E: HTN, Na and H2O retention, K/Ca loss

Glucocorticoids
• Catabolic, immunomodulatory and reduce inflammation• Gluconeogenesis during fasting (liver)• Lipid breakdown and inhibition of glucose and lipid storage• Glucocorticoid-receptor on DNA influences inflammatory gene expression• Lipocortin enzyme inhibits phospholipase A2 involved in arachidonic acid• Direct inhibition of COX2
• Prednisone, dexamethasone, hydrocortisone (predominance only)• Treats inflammatory conditions• A/E: Immunosuppression, fluid shifts, brain, psychology changes,
suppresses Ca2+ absorption, diabetes• Tapering required

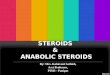
Primary effects of glucocorticoids
Anti-inflammatory:
Inhibit inflammation by blocking the action of inflammatory mediators (transrepression), or by inducing anti-inflammatory mediators (transactivation)
Immunosuppressive:Suppress delayed hypersensitivity reactions by directly affecting T-lymphocytes
Anti-proliferative: Inhibition of DNA synthesis and epidermal cell turnover
Vasoconstrictive:Inhibit the action of histamine and other vasoconstrictive mediators
http://aacijournal.biomedcentral.com/articles/10.1186/1710-1492-9-30

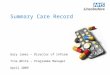
Approximate equivalent dose* (mg)
Relative glucocorticoid activity
Relative mineralocorticoid activity Duration of action (hours) General therapeutic
indicationsGlucocorticoidsShort-acting
Hydrocortisone 20 1 1 8-12• Relatively high mineralocorticoid activity makes it suitable for use in adrenal insufficiency
Cortisone 25 0.8 0.8 8-12 • Similar to hydrocortisoneIntermediate-acting
Prednisone 5 4 0.8 12-36• High glucocorticoid activity makes it useful for long-term treatment, and as an anti-inflammatory/ immunosuppressant
Prednisolone 5 4 0.8 12-36 • Similar to prednisone
Methylprednisolone 4 5 Minimal 12-36• Anti-inflammatory/immunosuppressant
Long-acting
Dexamethasone 0.75 30 Minimal 36-72
• Anti-inflammatory/immunosuppressant; used especially when water retention is undesirable given its minimal mineralocorticoid activity
• Usually reserved for short-term use in severe, acute conditions given its high potency and long-duration of action
Betamethasone 0.6 30 Negligible 36-72 • Similar to dexamethasoneMineralocorticoids Fludrocortisone ** 10-15 125-150 12-36 • Used for aldosterone
replacement

Prednisone (Prednisolone): Mechanism of Action)• Most commonly used glucocorticoid due to high activity• Prednisone prednisolone in liver• mild mineralocorticoid activity and moderate anti-inflammatory effects• controls or prevents inflammation by controlling rate of protein synthesis• suppresses migration of PMNs and fibroblasts, • reverses capillary permeability, and stabilizes lysosomes at cellular level• corticosteroids are administered in physiologic doses to replace deficient
endogenous hormones and in larger (pharmacologic) doses to decrease inflammation

Prednisone: Pharmacology
• Absorption• Bioavailability: 92%• Duration: Plasma, 60 min; biologic, 8-36 hr• Peak plasma time: PO (immediate release), 2 hr; PO (delayed release), 6.0-6.5 hr
• Distribution• Protein bound: 65-91%
• Metabolism• Extensively metabolized in liver; hydroxylated to active metabolite; conversion can be
impaired in liver disease• Elimination
• Half-life: 2.6-3 hr• Dialyzable: Hemodialysis, no• Excretion: Urine (mainly)

Prednisone: Dosage and uses
• Initially up to 10-20mg daily (severe up to 60mg/day) PO in single daily dose or divided q6-12hr (immediate-release or delayed-release formulation ~4 hours to release active substances) preferably taken in morning after breakfast. Can often be reduced in a few days, but may need to be continued weeks or months.
• Maintenance usually 2.5-15mg daily; >7.5mg daily increases risk of Cushingoid effects
• IM 25-100mg once or twice weekly• Exogenous steroids suppress adrenal cortex activity least during maximal
natural adrenal cortex activity (between 4:00 and 8:00)• Acute asthma, Giant cell arteritis, ITP, Rheumatoid arthritis, Advanced
Tuberculosis, Autoimmune hepatitis, IBD, Eye, Ear
Approximate equivalent dose* (mg)
Relative glucocorticoid activity
Relative mineralocorticoid activity
Duration of action (hours)
Hydrocortisone 20 1 1 8-12 Cortisone 25 0.8 0.8 8-12 Prednisone 5 4 0.8 12-36
Dexamethasone 0.75 30 Minimal 36-72
Fludrocortisone ** 10-15 125-150 12-36

Dexamethasone MOA
• High glucocorticoid to little mineralocorticoid activity so can be used in high doses• Suppresses PMN migration, • Reduces capillary permeability; • Stabilizes cell and lysosomal membranes, • Increases surfactant synthesis, increases serum [Vit A], • Inhibits PG and proinflammatory cytokines; • Suppresses lymphocyte proliferation through direct
cytolysis, inhibits mitosis, breaks down granulocyte aggregates, and improves pulmonary microcirculation

Dexamethasone: Pharmacology
• Absorption• Onset: Between a few minutes and several hours; dependent on indication and
route of administration• Peak serum time: 8hr (IM); 1-2 hr (PO)
• Distribution• Vd: 2 L/kg
• Metabolism• Metabolized in liver
• Elimination• Half-life: 1.8-3.5 hr (normal renal function)• Excretion: Urine (mainly), feces (minimally)

Dexamethasone: Dosage and uses
• Inflammation• 0.5-10 mg daily PO divided q6-12hr (20-200micrograms/kg daily in child)• IM/IV 0.5-24mg initially (200-400micrograms in child)• Intra-articular, intralesional, or soft tissue: 0.2-6 mg/day
• Cerebral Edema associated with malignancy• IV 10mg initially then 4mg IM q6hr for 2-4days tapered 5-7days
• Adjunct to bacterial meningitis, Severe or intractable allergy, Shock, Multiple Sclerosis (Acute Exacerbation), CAH, N/V w/ chemotherapy, rheumatic disease
• Paediatric: Airway oedema, croup, inflammation, meningitis, SOL oedema, spinal cord compression
• Dexamethasone suppression test

Dexamethasone suppression test
• Low-dose test: Screening for Cushing syndrome• Overnight test: 1 mg PO between 23:00-24:00; cortisol level tested between 8:00 and 9:00
on following morning• Standard 2-day test: 0.5 mg PO q6hr (9:00, 15:00, 21:00, 3:00) for 2 days; cortisol level
tested 6 hours after final dose (9:00)• High-dose test: Confirmed Cushing syndrome for further workup to determine
cause • Standard 2-day test: determine baseline serum cortisol or 24-hr urinary free cortisol, then
2mg PO q6hr for 2 days; urine free cortisol is collected, and serum cortisol is checked 6 hours after final dose
• Overnight test: After determination of baseline serum cortisol, 8 mg (typically) PO between 23:00 and 24:00; cortisol level tested between 8:00 and 9:00 on following morning
• IV test: After determination of baseline serum cortisol, 1 mg/hr by continuous IV infusion for 5-7 hours

Hydrocortisone
• Glucocorticoid with mild mineralocorticoid activity and moderate anti-inflammatory effects• Much more mineralocorticoid activity than others, therefore
not suitable for long term use internally• Topical use most common• controls or prevents inflammation by controlling rate of
protein synthesis, suppressing migration of PMNs and fibroblasts, and reversing capillary permeability

Hydrocortisone: Pharmacology
• Absorption• Bioavailability: PO, 96%• Short-acting duration
• Distribution• Protein bound: 90%• Vd: 34 L
• Metabolism• Metabolized in tissues and liver• Metabolites: Glucuronide and sulfates (inactive)
• Elimination• Half-life: Plasma, 1-2 hr; biologic, 8-12 hr• Excretion: Urine (mainly), feces (minimally)

Hydrocortisone: Dosage and uses
• Inflammation• 15-240 mg PO/IM/IV q12hr
• Status Asthmaticus• 1-2 mg/kg IV q6hr initially for 24 hours; maintenance: 0.5-1 mg/kg q6hr
• Acute Adrenal Insufficiency• 100 mg IV bolus, then 300 mg/day IV divided q8hr or administered by continuous infusion for 48
hours• When patient is stable: 50 mg PO q8hr for 6 doses, then tapered to 30-50 mg/day PO in divided doses
• Chronic Adrenal Insufficiency• 20-30 mg daily PO divided q8-12hr (child 10-30mg)
• Dosage Considerations• Usual PO dosing range: 10-320 mg/day divided q6-8hr• Usual IV/IM dosing range (sodium succinate): 100-500 mg PRN initially; may be repeated q2hr, q4hr,
or q6hr PRN• Shock, hypersensitivity reactions, severe IBD, haemorrhoids, rheumatic disease, eye,
skin

Fludrocortisone
• Potent mineralocorticoid with high glucocorticoid activity; promotes increased reabsorption of sodium and excretion of potassium from renal distal tubules
• Absorption• Bioavailability: 100%• Peak plasma time: ≤1.7 hr
• Distribution• Protein bound: 42%
• Metabolism• Metabolized in liver
• Elimination• Half-life: Plasma, 3.5 hr; biologic, 18-36 hr

Fludrocortisone: Dosage and uses
• Adrenocortical Insufficiency/Addison Disease• Primary and secondary adrenocortical insufficiency in Addison
disease• Usually 0.1 mg/day PO; ranges from 0.1 mg PO 3 times weekly - 0.2
mg/day PO• If hypertension occurs: 0.05 mg/day PO
• Salt-Losing Forms of Congenital Adrenogenital Syndrome (CAH)• 0.1-0.2 mg/day PO
Approximate equivalent dose* (mg)
Relative glucocorticoid activity
Relative mineralocorticoid activity
Duration of action (hours)
Hydrocortisone 20 1 1 8-12 Cortisone 25 0.8 0.8 8-12 Prednisone 5 4 0.8 12-36
Dexamethasone 0.75 30 Minimal 36-72
Fludrocortisone ** 10-15 125-150 12-36

Neuro: Arachnoiditis, convulsions, depression, emotional instability,
euphoria, headache, increased ICP (pseudotumor cerebri; usually
following discontinuation), insomnia, meningitis, mood swings, neuritis, neuropathy,
paraparesis/paraplegia, paresthesia, personality changes,
sensory disturbances, vertigo
Ophthalmic: Exophthalmos, glaucoma, increased IOP, posterior
subcapsular cataracts, central serous chorioretinopathy
Musculoskeletal: Osteonecrosis of femoral and humeral heads,
Charcot-like arthropathy, loss of muscle mass, muscle weakness, osteoporosis, pathologic fracture of long bones, steroid myopathy,
tendon rupture, vertebral compression fractures
CV: arrest, arrhythmias, hypertrophy, CHF, fat embolism, HTN, myocardial rupture post-MI,
pulmonary edema, syncope, thromboembolism,
thrombophlebitis, vasculitis
Derm: Acne, allergic dermatitis, cutaneous and SC atrophy, dry scalp, edema, facial erythema, hyper- or hypopigmentation,
impaired wound healing, hyperhidrosis, petechiae and
ecchymoses, rash, sterile abscess, striae, suppressed reactions to
skin tests, thin fragile skin, thinning scalp hair, urticaria
Endo: Abnormal fat deposits, cushingoid state, hirsutism, metabolic state requiring
glycaemic control, menstrual irregularities, moon facies, 20
adrenocortical + pituitary unresponsiveness (in times of
stress, trauma, surgery, or illness), growth suppression
GI: Abdominal distention, high LFTs (often reversible), hepatomegaly,
hiccups, malaise, nausea, pancreatitis, peptic ulcers,
ulcerative esophagitis
Allergic: Anaphylaxis, angioedema
Immunosuppression: susceptible to invasive fungal and viral
infections, reduced febrile and inflammatory response
Fluid and electrolytes: Fluid retention, potassium loss, HTN, hypokalemic alkalosis, sodium
retention
General: Increased appetite and weight gain
Metabolic: Negative nitrogen balance due to protein catabolism
Reproductive: Alteration in motility and number of spermatozoa
Adverse effects

Adverse effects
Adrenal suppression:
• Weakness/fatigue• Malaise• Nausea• Vomiting• Diarrhea• Abdominal pain• Headache (usually in the morning)• Fever• Anorexia/weight loss• Myalgia• Arthralgia• Psychiatric symptoms• Poor linear growth in children• Poor weight gain in children
Adrenal crisis:
• Hypotension• Decreased consciousness• Lethargy• Unexplained hypoglycemia• Hyponatremia• Seizure• Coma
• GC-associated toxicity appears to be related to both the average dose and cumulative duration of GC use
• Tapering has not been proven to improve outcomes, despite abrupt withdrawal having empirically shown to induce symptoms of adrenal suppression
• Before long-term therapy, a thorough history and examination should assess risk or pre-existing conditions, such as diabetes, dyslipidemia, CVD, GI, affective disorders, or osteoporosis.
• Baseline measures of body weight, height, BMD and blood pressure should be obtained, along with laboratory assessments that include a complete blood count (CBC), blood glucose values, and lipid profile
• In children, nutritional and pubertal status should also be examined.

Prevention of adverse events• Treat pre-existing comorbid conditions that may increase risk of GC-associated AEs• Prescribe lowest effective GC dose for minimum period of time required to achieve treatment goals• Administer as single daily dose (given in the morning), if possible• Consider intermittent or alternate-day dosing, if possible• Use GC-sparing agents whenever possible (e.g., omalizumab in severe asthma, azathioprine/cyclophosphamide in vasculitis, methotrexate in rheumatoid arthritis)• Advise patients to: ▪ Carry a steroid treatment card ▪ Seek medical attention if they experience mood or behavioural changes ▪ Avoid contact with persons that have infections, such as shingles, chickenpox, or measles (unless they are immune) ▪ Not discontinue GC therapy abruptly unless advised to do so by their physician ▪ Adopt lifestyle recommendations to minimize the risk of weight gain or other AEs: ▫ Eat a healthy balanced diet, including adequate calcium intake ▫ Smoking cessation ▫ Reduction in alcohol consumption ▫ Regular physical activity• Regularly monitor for signs/symptoms of AEs

GC Sparing
• GC-sparing agents should be considered whenever possible• In severe asthma, use of the anti-immunoglobulin E (IgE)
monoclonal antibody, omalizumab (presently reserved for patients with difficult to control asthma with documented allergies and remain uncontrolled despite ICS therapy)• In SLE, mycophenolate mofetil, and also in rheumatoid
arthritis, azathioprine may be used to greatly reduce the amount of GC used

PrednisoneTapering
1. Reduce dose by 2.5- to 5.0-mg decrements every 3–7 days until physiologic dose (5 to 7.5 mg of prednisone per day) is reached; slower tapering of GC therapy may be recommended if risk of disease relapse is a concern2. Switch to hydrocortisone 20 mg once-daily, given in the morning3. Gradually reduce hydrocortisone dose by 2.5 mg over weeks to months4. Discontinue/continue hydrocortisone based on assessment of morning cortisol:
< 85 nmol/L:HPA-axis has not recovered→ continue hydrocortisone→ re-evaluate patient in 4–6 weeks
85-275 nmol/L:
Suspicious for AS→ Continue hydrocortisone→ Further testing of HPA axis or re-evaluate in 4–6 weeks→ If further evaluation of HPA axis is selected: ▪ ITT (gold-standard but not widely available) ▪ ACTH stimulation testing (see below)
276-500 nmol/L:HPA-axis function is likely adequate for daily activities in a non-stressed state, but may be inadequate for preventing adrenal crisis at times of stress or illness
→ Discontinue hydrocortisone → Monitor for signs & symptoms of AS
→ Consider further evaluation of HPA axis to determine if function is also adequate for stressed states or consider empiric therapy with high-dose steroids during times of stress
> 500 nmol/L: HPA axis is intact→ discontinue hydrocortisone
↓If ACTH stimulation testing is performed and:
Peak cortisol rises to > 500 nmol/L: HPA axis intact and GC can be discontinuedPeak cortisol < 500 nmol/L: Steroids required at times of stress and illness until normal
ACTH response is noted
• Consider screening to assess adrenal function as GC therapy is being withdrawn
• Screening should occur before tapering to less than a physiologic dose
• Symptomatic AS should be treated with daily replacement plus “stress doses” during physiological stress (intercurrent illness, injury or surgery)

Conclusion
• Corticosteroid therapy is ubiquitous throughout medical therapy• They have many benefits and AEs through sustained use,
but have the potential to be prevented• Differences in the monitoring and care of adults versus
children• Patients should be informed • Steroids can do good!

References
• MedLinePlus https://www.nlm.nih.gov/medlineplus/steroids.html• Wikipedia images https://en.wikipedia.org/wiki/Adrenal_gland https://en.wikipedia.org/wiki/Renin%E2%80%93angiotensin_system • HOPES http://web.stanford.edu/group/hopes/cgi-bin/hopes_test/glucocorticoids/ • http://www.cvphysiology.com/Blood%20Flow/AA%20metabolism.gif • Mineralocorticoids http://www.vivo.colostate.edu/hbooks/pathphys/endocrine/adrenal/mineralo.html • Medscape Drugs & Diseases
http://reference.medscape.com/drug/decadron-dexamethasone-intensol-dexamethasone-342741 • http://classconnection.s3.amazonaws.com/319/flashcards/1117319/jpg/addisons_disease1332524676283.jpg • Mayo Clinic – Addison’s
http://www.mayoclinic.org/diseases-conditions/addisons-disease/symptoms-causes/dxc-20155757 • A practical guide to corticosteroid therapy
http://aacijournal.biomedcentral.com/articles/10.1186/1710-1492-9-30 • BNF 57 March 2009• http://www.nature.com/jhh/journal/v19/n1/fig_tab/1001777f1.html