Embed Size (px)
Citation preview


Surgical Anatomy Of
The Retina
BY
Mohamed Abdel-Aziz (MSc,ICO,Egyption Board)

Eye from outside

The conjunctiva
-Is adherent to the sclera at the limbus,
- So the radial incisions to enter the subconjunctival plane have to
be made just behind the limbus.

Tenon’s capsule
-Is a layer of fascia that envelops the globe from the limbus to the optic nerve . -It is pierced by the extraocular muscles.-A glove-like sleeve of fascia extends anteriorly (to the rectus insertions) and posteriorly (for several mm) along the muscles from the points at which they pierce Tenon’s capsule.
-Between the rectus muscles anteriorly these sleeves are joined by a layer of fascia.
-Care must be taken when stripping fascia off the rectus
muscles because ligaments from the recti to the wall of the
orbit are functionally important in the actions of the muscle.

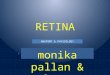
(a) Conjunctiva and (b) anterior Tenon’s have been dissected to revealthe (c) “posterior Tenon’s” glove-like extensions of tenons capsule alongthe recti and the associated intermuscular septum. (d) Bare sclera liesunder this.

The sclera
-The thickness of the sclera varies. It is thickest around the optic
nerve (1.2 mm) and thinnest under the recti behind their insertions
-So attempts to pass scleral sutures under the muscles are
particularly hazardous.Where scleral mattress sutures are more
typically passed, at the equator, it is approximately 1 mm thick.


Extra ocular muscles
-The recti are adherent to the sclera at the spiral of Tillaux. The location of
this ring corresponds approximately to that of the ora serrata .
-Circumferential scleral tires are therefore often placed as anteriorly as the
rectus muscle insertions will allow. In this position they support the retina asfar anteriorly as the ora serrata (“break ora occlusive buckling”).
-The superior oblique muscle runs laterally from the trochlea to its insertion
under the superior rectus.
-Passage of a superior rectus muscle hook from the temporal side of themuscle reduces the risk of inadvertently “hooking” the superior oblique as
well as does keeping the sweep of the hook pre-equatorial.

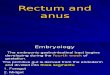
The ora serrata and the spiral of Tillaux (rectus insertions).The sclera has been rendered transparent to reveal the relationship between the ora serrata and the muscle insertions. Buckling anteriorly as far as the rectus insertions prevents anterior leakage.

Choroidal vasculature
-The long posterior arteries (as well as their correspondingnerves) run anteriorly from the equator at 3 and 9 o’clock .
-They may be damaged by subretinal fluid drainage in these
meridia .
-The anatomy of the vortex veins is somewhat variable but one
tends to leave the globe either side of the vertical recti just behind
the equator.
-They may be inadvertently hooked along with a vertical rectus
muscle if the muscle hook is passed behind the equator.
-Injury to the vortex veins may result in interruption to the venous
drainage from the choroid and choroidal detachment.


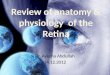
vortex veins (v), optic nerve (on), muscular tendon of inferior oblique (io), tendon of superior oblique (so), short posterior ciliary arteries (arrows), short posterior ciliary nerves (n), and long posterior ciliary artery and nerve (arrowhead).

-When operating near the vertical recti the vortex veins
should be identified to prevent injury.
- Because the vortex veins tend to be located near the vertical
recti subretinal fluid drainage is carried out closer to the
horizontal than to the vertical recti whenever possible.
-The anterior ciliary arteries are useful indicators of the meridia
of the rectus muscle insertions .
-As they supply the arterial circles of the iris surgical trauma
(including diathermy) should be minimized.

A, anterior ciliary artery; B, long posterior ciliary artery; C, vortex ampulla;D, vortex vein; E, greater arterial circle of the iris

Innervation
-Sensory nerves from the globe and bulbar conjunctiva pass
through the ciliary ganglion.
- Local anesthesia in this region, for example, sub-Tenon’sanesthesia, will therefore anesthetize the globe effectively.
-The innervation of the lids and palpebral conjunctiva is by the
lacrimal, frontal and infraorbital nerves, which do not pass
through the muscle cone.
-Blockage of the ciliary ganglion alone does not therefore
reliably provide adequate analgesia for buckling surgery.


The macula
the macula to the inferior oblique muscle was 1.35±0.42 mm.
Relationships among the optic nerve, superior oblique muscle (SO), inferior oblique muscle (IO), and macula (M). Right eye.

Eye from inside

-The vitreous can be considered as a three-dimensional matrix of
collagen fibers and hyaluronic acid gel .
-In the normal state, the outer surface of the vitreous is in contact
with the retina, pars plana, and ciliary body.
The vitreous

The vitreous is a three-dimensional matrix of collagen fibers and hyaluronic acid gel.

-Area centralis
-It measures 5.5 to 6 mm in diameter(outermost circle) and its subdivisions(inner circles).
-The central area of the macular regionis represented by the fovea centralis(2),approximately 1.85 mm in diameter,which has a central pit, the foveola(1),0.35 mm in diameter.
- The anatomically retinal belts thatsurround the fovea centralis are theparafovea (3), 0.5 mm wide, andperifovea (4), 1.5 mm wide.

Peripheral Retina
Pars plana
Ora serrata

-The ciliary body starts 1 mm from the limbus and extends posteriorly
for about 6 mm.
-The first 2 mm consist of the pars plicata and the remaining 4 mm comprises the flattened pars plana
Pars plana

The inner aspect of the ciliary body showing the pars plicata (a) and the pars plana (b). The ora-serrata is at (c), and posterior to it the retina shows cystoid degeneration (d).



ORA SERRATA
It is the last region where the retinaends and ciliary body starts.
consist of tooth like projection .
Retina is attached both to the vitreous& retinal pigmented epithelium.

Normal VariantS of Ora Serrata
-Meridoneal fold
-Enclosed oral bay
- Granulation tissue

Choroidal vasculature and nerves from
inside




Inferior short posterior ciliary nerve
(arrow) adjacent to vortex vein complex


Temporal long posterior ciliary nerve

-The long posterior
ciliary arteries (as well
as their corresponding
nerves) run anteriorly
from the equator at 3
and 9 o’clock .
-They may be damaged
by heavy
photocoagulation or
subretinal fluid
drainage in these
meridia .