Embed Size (px)
Citation preview

SURGICAL APPROACHES TO HIP Jt
Dr.SATEESH CHANDRA ORTHO PG
GMC

APPROACHES OF HIP4 Basic approaches : Anterior -Less commonly used for THR ;
b/w sartorious & TFL. Anterolateral - Most common approach for
THR; b/w TFL & G.medius Posterior- Most common approach around
hip; b/w GL.medius & maximus Medial-rarely used

ANTERIOR APPROACH:(SMITH PETERSON APPROACH)
Gives safe access to hip & iliumINDICATIONS: Open reduction of congenital dislocations of hip when
dislocated femoral head is anterosup. To the true acetabulum
Synovial biopsies Intra articular fusions THR Hemiarthroplasty Excision of tumors Pelvic osteotomies using upper part of approach

POSITION:
Supine with sand bag under the buttock for pelvic osteotomy

LANDMARKS:ASIS, iliac crest.
INCISION:Long incision over anterior half of the iliac
crest to the ASIS.Curve down from ASIS vertically for 8-10cms
heaving towards lateral side of patella.

INTERNERVOUS PLANE:
Superficial plane b/w sartorius (innervated by femoral N.) & TFL(innervated by sup.glut.N)
Deep plane lies b/w RF(by femoral N.) & GL.medius(supplied by sup.glut.N.)

SUPERFICIAL DISSECTION Externally rotate the leg to stretch sartorius. Carefully cut through the gap b/t sartorius and TFL
about 3” distal to the ASIS. Avoid cutting Lat. cut .N. of thigh, incise deep fascia. Retract sartorius upwards & medially; TFL down &
laterally Detach the TFL at iliac origin. Ligate the ascending branch of Lat.circumflex Fem A.
in this plane.

DEEP DISSECTION: Separating sartorius & TFL exposes 2 muscles the GL. Medius &
Rectus femoris. Pass into the plane b/w Rect,F & GL.medius which is lateral to
the Femoral.A. Retract the R.F ,expose the capsule of hip jt. Retract the iliopsoas passing medially towards lesser trochanter. Adduct & externally rotate the leg to stretch the capsule. Incise the capsule as required ( T/longitudanal)& dislocate the
hip by ext.rotation.

DANGERS: NERVES:LFCN. of thigh may be injured b/w sartorius & TFL.Femoral N. – may be injured if plane is missed during
deep dissection as it lies anterior to hip , medial to RF,lateral to the femoralA.
VESSELS: Ascending branch of lat.circumflex F.A. may be injured
in the plane b/t TFL & sartorius.
ENLARGING THE APPROACH:In superficial dissection - by detaching sartorius at the
origin.In deep dissection- origin of GL.medius ,minimus to be
detached.

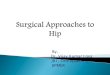
EXTENSILE MEASURES:Can be extended posteriorly to expose iliac crest.Can be extended distally along anterolateral thigh into
plane b/w V.lateralis & Rectus .femoris gives good exposure of entire shaft of femur.
Can be extended to allow inner & outer walls of plvis at hip for osteotomies
V.LAT
R.F
Periosteum femur

ANTEROLATERAL APPROACH:( WATSON-JONES APPROACH)
Most commonly used for THR Releases all abductor mechanism, hence hip can be
adducted fully hence acetabulum is fully exposed. Abducor mechanism released either by trochanteric
osteotomy / by cutting the ant.part of GL.medius & the whole Gl.minimus off the G.T
INDICATIONS: THR ORIF of # NOF Hemiarthroplasty Synovial biopsy Biopsy Femoral N.

POSITION: Supine so close to the edge that thebuttock of the
affected side hangsover. Flex the leg upto 30 deg. , adduct it so that leg lies
across the opposite knee. Tilt the table away, drape the pt. so that the limb
can be moved during surgery.
LANDMARKS: ASIS GT Femoral shaft V.Lat ridge

INCISION: 8-15cm longitudanal&straight centered over the Tip of
GT. Incision crossess the post.3rd of the GT before running
down the shaft.
INTERNERVOUS PLANE: No internervous plane. Surgical plane is b/w TFL & GL.medius(supplied by
sup.GT N.) Nerve to TFL enters the muscle at its origin. So as long as the plane is extended upto the illium the
TFL remains uneffected.

SUPERFICIAL DISSECTION: cut the S.C tissue to reach the fascia over posterior margin of GT & incise
fascia lata there to enter the overlying bursa. Divide the fibers of fascia lata proximally & anteriorly in the direction of
ASIS, & also distally to expose the vast,lateralis muscle. Lift the ant. Flap & detach few fibers of GL.medius to develop a plane b/w
TFL & GL.medius. Series of vessels come across the plane act as guide & need to be ligated. Retract the GL.med. & mins proximally & laterally to uncover the sup
margin of Jt, capsule.

Externally rotate the hip to stretch the capsule
Inscise it
To expose V lat. origin
Reflect v.lat origin for ~1cm to expose the jt. Anteriorly keeping the fat pad intact

DEEP DISSECTION: Detach abdutor mechanism & dissecting up the
femoral neck superficial to the capsule until a retractor can be placed over ant. Lip of acetabulum
2 techniques for good exposure of acetabulum by
Neutralising abductor mechanism &allowing femur to fall posteriorly.
Trochanteric osteotomy % detachment of abductor mechanism. Dissect ant surface if hip jt.capsule in line with
femoral neck & head. Detach reflected head of Rect.F from Jt. Capsule
to expose the ant. rim of acetabulum


Elevate the psoas tendon from capsulePlace Homan retractor over ant lip of acetabulum
beneath the RF & psoas as the nervous bundle is anterior to the psoas.
Incise the capsule longitudinally T H.DANGERS:NERVESFemoral N. Most commonly neuropraxia due to
excess medial retraction. FemoralA/V due to poor handling.Prevented by proper placing of retractor 1 o’ clock position for Rt. Hip 11 o’ clock position for Lt. hip Profunda femoris A.# of femoral shaft

ENLARGING THE APPROACH:Post. Fascia lata may prevent adduction of hip
which is needed for hip dislocation.Overcome by incision over post.flap of TFL
obliquely upwards in line with Gl. Max.EXTENSILE MEASURES:Can be extended distally to expose the lateral
aspect of femur.Can’t be extended proximally.

LATERAL APPROACH TO HIP: Exellent approach to hip replacement. No need for trochanteric osteotomy. Early mobilisation of pt possible as the
Gl.medius is preserved. But not a wider approach as anterolateral
approach.POSITION:Supine with GT at the edge of the table.LANDMARKS:ASISG.TShaft of femur

INCISION:Start about 5cm above the tip of GT pass over centre of tip of GT
to extend ~8cm down the shaft.
INTERNERVOUS PLANE:No internervous plane as G.M & V.L split in their own line.SUPERFICIAL DISSECTION: Cut through the fat & deepfascia Pull the TFL anteriorly,GMposteriorly Detach fibers of GL.medius & develop a plane b/w V.lat &
glut.medius.

DEEP DISSECTION: Split the GL. Medius starting in the middle of GT. Don’t go beyond 3cm up the GT.to preserve sup.GL.N. Split the fibers of V.lats at the base of the GT, Develop ant. f;lap consisting of ,GL.MED , GL.MIN & V.L Detach muscles from GT Continue disection anteriorly along femoral neck till
ant.capsule of hip. Develop space b/w hip capsules & muscles Enter the capsule using T shaped incision Ostetomise the neck , extract the head with cork screw to
expose the acetabulum.

DANGERS:NERVES: Sup.GL.N. damage at the upper end of incision
above GT. Prevented by stay suture in the GL. Med Femoral N. damaged by inadvertly placed
retraction Prevented by placing retractor strictly on the
bone.VESSELS: Fem. Vessels by retractor ENLARGING THE APPROACH: EXTENSILE MEASURE: Can be extended down to expose the shaft of
femur.

POSTERIOR APPROACH:(MOORES APPROACH)
Most commonly used approach & practical Easy ,safe, quick Not used for# neck of femurINDICATIONS:HemiarthroplastyTHR including revisionORIF of post. Acetabular #Dependent drainage in hip sepsisRemoval loose bodiesPedicle bone grafting OPEN reduction of posterior dislocation

POSITION:True lateral with affected limb above
LANDMARK:GTINCISION: 10-15cm curved centered on posterior aspect of GT Begin proximally 6-8cms posterosuperior to posterior
aspect of GT Continue to GT Curve the incision in line with fibers of GT Continue along shaft of femurINTERNERVOUS PLANE: No true plane

SUPERFICIAL DISSECTION:Cut the fascia lata to expose the V.lat.Superiorly split the fibers of GM(very important) gently.DEEP DISSECTION: Retract GL.maximus & deep fascia to expose
posterolateral aspect of hip. Cover by short ext.rotators. Internally rotate the hip to move sciaticN. away from
the field. Detach piriform & obt.internus retract them posteriorly. Incise the hip jt, capsule , to expose the head & neck of
femur. Internally rotate femur for hip dislocation.

DANGERS:Sciatic N &Inf GL.A (both may be damaged
while splitting GL. Max.ENLARGING THE APPROACH:LOCALLYBy extending the skin / fascial incisionBy detaching upper ½ of Q.femoris 1cm from
insertion.By detaching the origin of GL.max for femoral
neck & shaft.

MEDIAL APPROACH(LUDOLFFS APPROACH)
INDICATIONS: Open reduction of congenital dislocation of hip. Biopsy & RX of tumors of the inf.portion of femoral neck &
medial aspect of proximal shaft. Psoas release Obturator neurectomy. By making short transverse/longitudinal incision-used for
adductor release

POSITION:Supine with affected hipflexed , abducted & externally rotated.Sole of foot lies along the medial side of opp. Knee.LANDMARKS:Adductor longus traced to its originPubic tubercleGTINCISION:Longitudinal incision on the medial thigh starting 3cm below pubic tubercle
that runs down over adductor longusLength depends on amount of femur to be exposedINTERNERVOUS PLaNE:Superficial dissection b/w adductor.longus & gracialisDoesn’t involve int.N.plane

SUPERFICIAL DISSECTION:B/w adductor longus & gracialisDEEP DISSECTION:B/w adductor brevis & magnus till lesser
trochanterProtect post.division of obt.N. to preserve
innervation of adductor portion of Ad.magnus.
Place a bone spike above & below the lesser trochanter to isolate psoas tendon.

DANGERS:NERVES:Ant,div of obt.N which lies at the top of the
obt.externus running b/w add.longus & brevis.Post.div of obt.N. lies with in the obt,externus
which it supplies before it leaves the pelvis.Runs down thw thigh on adductor magnus under
the brevis,it also supplies adductor portion of adductor magnus.
These nerves are transected if approach is meant for adductor spasm or else protect them.
VESSELS:Medial femoral circum flex A.-may be injured at
distal part of psoas.

ENLARGING THE APPROACH: Locally can be extended by detaching psoas
& iliacus at L. T can expose 5 more cm of femoral shaft.
EXTENSILE MEASURE:Can never be enlarged