Embed Size (px)
DESCRIPTION
this is a case of very rare disease
Citation preview
Salman Saleem
FCPS-II trainee
Name: aaa
Age: 22 years
Gender: female
Marital Status: Unmarried
Resident of lahore
Date of presentation: 22nd May 2014
Presented with chief complaint of
Left upper limb pain-----------1month
My patient had pain in left upper arm, most
sever in left forearm and hand which was
Aching in nature, present most of the time
and aggravated by doing any kind of work.
There was associated numbness and
coldness of the left hand.
There is no history of any color changes
on exposure to cold. There is no H/O skin
rash or fever
There is H/O generalized body aches and pains, sometimes left shoulder pains but no systemic joint pains, stiffness, redness or swelling.
There is no HO lower limb pain or claudication. No Chest pain or SOB
No HO vertigo, dizziness, blackouts or headache
No HO cough sputum, hemoptysis, burning micturtion, hematuria, pyuria
No GIT disturbanceNormal periods.
She had Hx of fever 07 months back. The fever continued for 01 month. It was mostly low
grade, intermittent. fever was associated body aches and join pains involving both small and large joints. There was no joint swelling or stiffness
There was also dry cough and exercise intolerance. There was no HO hematuria or burning. No GIT symptoms.
No hx Skin rash She remained under treatment from various physicians
and got worked up to find out the cause of fever but no conclusive diagnosis could be made. The fever finally subsided after 01 month
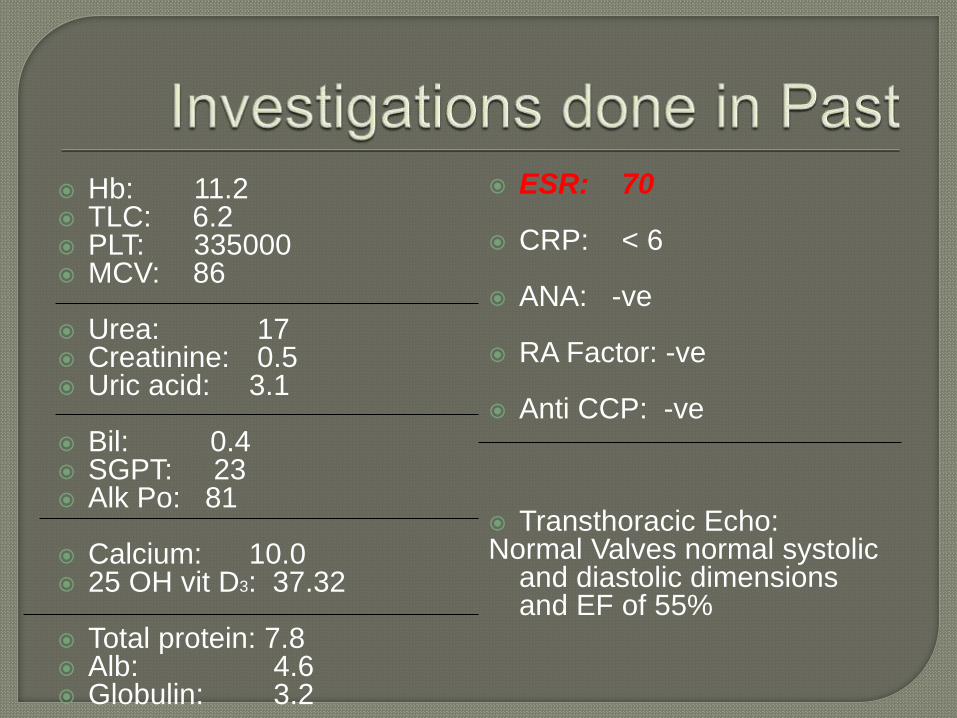
Hb: 11.2 TLC: 6.2 PLT: 335000 MCV: 86
Urea: 17 Creatinine: 0.5 Uric acid: 3.1
Bil: 0.4 SGPT: 23 Alk Po: 81
Calcium: 10.0 25 OH vit D3: 37.32
Total protein: 7.8 Alb: 4.6 Globulin: 3.2
ESR: 70
CRP: < 6
ANA: -ve
RA Factor: -ve
Anti CCP: -ve
Transthoracic Echo:Normal Valves normal systolic
and diastolic dimensions and EF of 55%
Family history: no history IHD,DM or
dyslipidemia any similar illness in family
Personal Hx: She is staff nurse by
profession
There is no HO, smoking, addiction or drug
dependance
Menstrual History: noramal
Young female of average height and built looks anxious
BP: 110/70 in rt arm and was not recordable in left arm
PULSE: 90 b/min
ABSENT LEFT RADIAL. Left brachial but ulnar artery was very feeble. There was no change in pulse with change of position of left UL or neck
All other pulses were normal. no radiofemoral delay
R/rate: 18/min Temp: 98.6F
There was no clubbing, cyanosis or edema
Chest: Normal vesicular breathing
Abd: Soft non tender no palpable visceromegaly
CVS: S1 and S2 audible with no murmur
CNS: Normal examination
1)Vasculitis: Large vessel:Takayasu’s arteritis , Giant cell arteritis,
2)Atherosclerosis
3)Buerger’s disease
4)Thoracic outlet syndrome
5)Coarctation of Aorta
(Medium vessel vasulitis: Polyarterititis nodosa, kawasaki’s disease
Small vessel: wegner’s granulomatosis , rheumatoid arthritis,) were also in differentials
Giant cell arteritis occurs in elderly with headache and jaw claudication
Thoracic outlet syndrome: its pain is aggravated with movement in vascular type thoracic outlet syndrom
Coarctation of Aorta: Pt has no radiofemoral delay and hypertention
Athersclerosis: donot involve subclavian artery as individual . No family history of dyslipidemia
Buerger’s disease ocuurs in middle aged smoker male and effects lower limb
PAN associated with abdominal pain, rashes, hematuria and peripheral neuropathy
Kawasaki disease occurs in childhood pts have eye symptoms, lymphadenopathy and cutaneous lesions
Wegner’s Granulomatosis: is associted with upper respiratory symptoms and hemoptysis
Rheumatoid arthritis: ho morning stiffness and multi organ involvement
CBC,ESR,ANA, RA factor, ENA, C-
ANCA,P-ANCA,
LFTS,RFTs,Lipid porfile
ECG
CXR
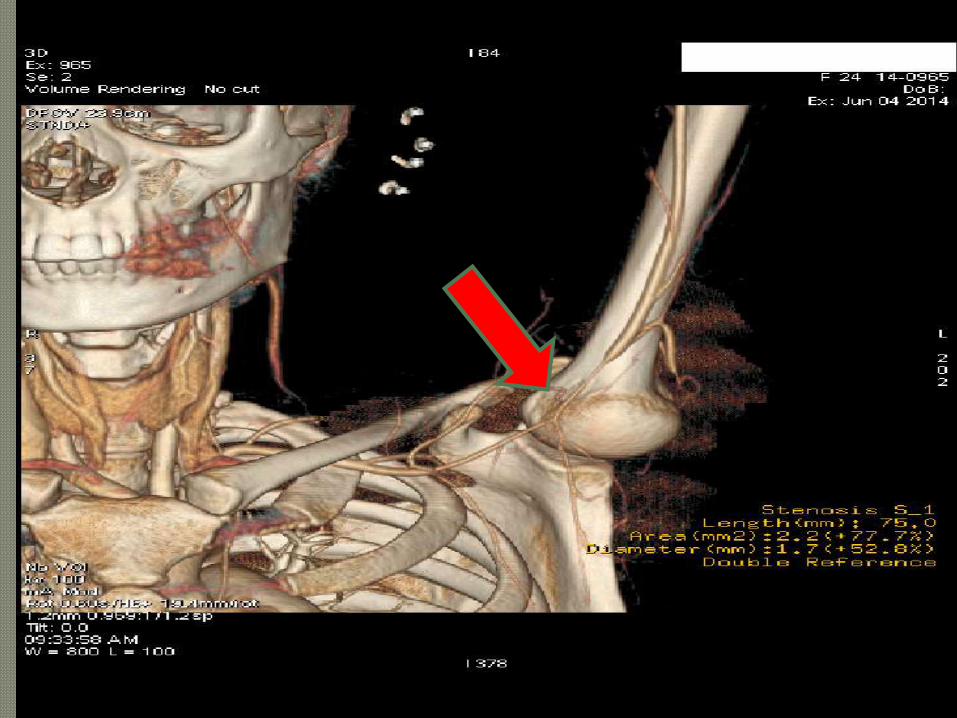
Arterail Doppler
CT Peripheral Angiogram was planned
Hb: 10.2
Plt: 453000
Tlc: 7800
Mcv: 80.6
ESR: 58
CRP: <6
Urea: 17
Creatinine: 0.5
S. Bil: 0.4
SGPT: 23
ALT: 32
Alk Phosp:81
Calcium: 8.9
Phosph: 3.9
Vit D3 : 37
Albumin: 4.6
Globulin: 3.2
ANA: -ve
RA Factor:-ve
Anti CCP:-ve
HBsAg:-ve
Anti HCV:-ve
Arterial doppler of left
upper Limb Shows
stenosis of the left
subclavian artery with
diminished flow
beyond
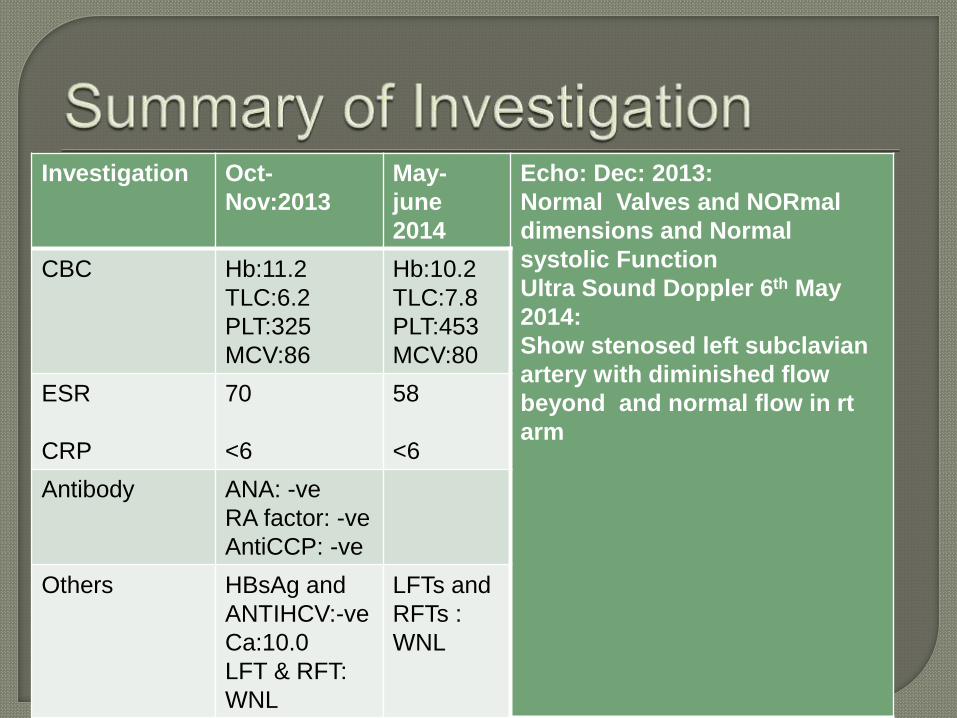
Investigation Oct-
Nov:2013
May-
june
2014
Echo: Dec: 2013:
Normal Valves and NORmal
dimensions and Normal
systolic Function
Ultra Sound Doppler 6th May
2014:
Show stenosed left subclavian
artery with diminished flow
beyond and normal flow in rt
arm
CBC Hb:11.2
TLC:6.2
PLT:325
MCV:86
Hb:10.2
TLC:7.8
PLT:453
MCV:80
ESR
CRP
70
<6
58
<6
Antibody ANA: -ve
RA factor: -ve
AntiCCP: -ve
Others HBsAg and
ANTIHCV:-ve
Ca:10.0
LFT & RFT:
WNL
LFTs and
RFTs :
WNL

Takayasu’s Arteritis
1) Age younger than 40yrs at disease onset2) Claudication of the extremities3) Decreased pulsation of one or both brachial arteries4) Difference of at least 10 mm Hg in systolic blood
pressure between arms5) Bruit over 1 or both subclavian arteries or the
abdominal aorta6) Arteriographic narrowing or occlusion of the entire
aorta, its primary branches, or large arteries in the upper or lower extremities that is not due to arteriosclerosis, fibromuscular dysplasia, or other causes
The presence of any 3 or more criteria yields a sensitivity of 90.5% and a specificity of 97.8%.[20]
First to treat as medically as shown by ESR & symptoms pt was in active stage and then to do intervention of left subclavian artery
So Pt was prescribed deltaacortil 30 mg per along with Methotrexate 10 mg weakly
Pts symptoms improved ESR dec: 70 08Methotrexate was stopped due to
hepatotoxicityAnd finally stenting of left subclavian artery
was done
Diagnosis
Is inflammatory arteritis of unknown origin involving medium and large size arteries.
Granulamtous inflammation of large arteries and medium sized arteies
Circulating antibodies plays important role
There may be stenosis (75%), occlusion or aneurysm of the arteries causing ischemic symptoms
May involve single branch of aorta or all arteries arising from aorta
Incidence of 2.6 cases per 1 million
It is more prevalent in japan and other Asian countries
More prevalent in female (8:1 ratio)
Remitting and relapsing very prolonged course that extend over years
Three stages:1) Active inflammatory phase (non constitutional
symptom)2) Vascular inflammatory stage( vascular stage)3) Burnt out stage: (vessels become fibrosed )
Type I - Branches of the aortic archType IIa - Ascending aorta, aortic arch, and its
branchesType IIb –Ascending, Arch plus thoracic
descending aortaType III - Thoracic descending aorta,
abdominal aorta, renal arteries, or a combination
Type IV - Abdominal aorta, renal arteries, or both
Type V - Entire aorta and its branches
Signs
Non specific like fever, rash, joint pain,weightloss
Limb claudication
Headache
Visual disturbance
Reynaud’s phenomenon
Symptoms
Hypertension
Pressure difference b/w two arms
Bruit
Signs of Aortic regurgitation
Signs of Bi ventricular failure
1) Age of 40 years or younger at disease onset2) Claudication of the extremities3) Decreased pulsation of 1 or both brachial arteries4) Difference of at least 10 mm Hg in systolic blood
pressure between arms5) Bruit over 1 or both subclavian arteries or the
abdominal aorta6) Arteriographic narrowing or occlusion of the entire
aorta, its primary branches, or large arteries in the upper or lower extremities that is not due to arteriosclerosis, fibromuscular dysplasia, or other causes
The presence of any 3 or more criteria yields a sensitivity of 90.5% and a specificity of 97.8%.[20]
Increase in Acute phase reactant like ESR
& CRP
Increased APR may show active disease
but may be normal
Patient may shows normocytic anemia and
thrombocytosis
All antibodies like ANA,ANCA, CCP will be
negative
Echocardiogram:may show valvular
abnormality ( AR) or bi ventricular failure due to myocarditits
CT angiogram: it is non invasive and detects early
disease MR angiogram:
detects early disease provide detailed information
Angiography :of affected artery is gold standard
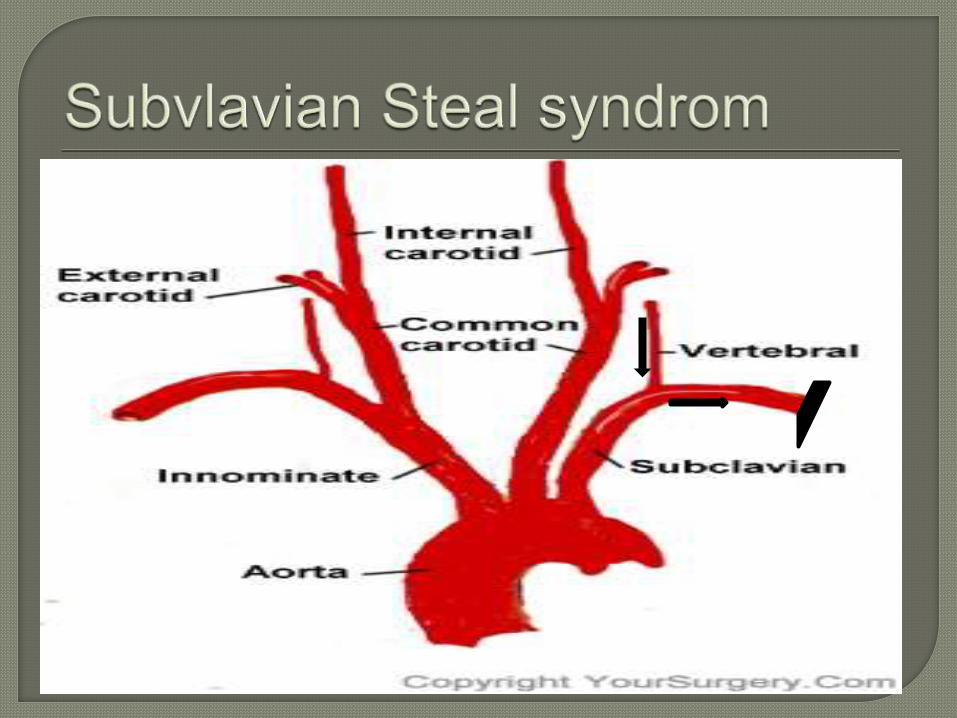
LIMB ISCHEMIASUBCLAVIAN STEAL SYNDROMECVARenovascular Hypertension when involve
renal arteryThromboembolic phenomenonRetinpathyBi-ventricular failure Valvular abnormality most common is Aortic
regurgitationComplication related to prolonged steroids
use
Assessing disease activity may be beneficial as it respond to steroid. presence of any of the following 2 out of 4 suggest active disease
1)Sytsemic features like fever and arthralgias
2)inc: ESR3)Features of ischemia like claudication
4)Typical angiographic features
Steroids like predisnolone 1mg/kgSteroids usually benefits patients with active
disease donot effect burnt out fibrosedvessels
½ of all pts on steroids do relapses after stoping
Adding immunosuppressive to non responders
Cyclophosphamide daily & Methotrexateweekly can be used to reduce dose of steroids
Anti TNF therapy
Literature had showed better outcome with
PTA because it can be reperformed
There can be restenosis of stented vessel
which is usually greater than PTA
performed in the Atherosclerosis lesions
However surgical grafting can achieve
better outcome with greater risk