Embed Size (px)
Citation preview

Difficult AirwayI
Alexander S. Nivena and Kevin C. Doerschugb
Copyright . 2013 Wolters Kluwer Health | Lippincott Williams & Wilkins
BAGIAN ILMU ANESTESI, PERAWATAN INTENSIF, DAN MANAJEMEN NYERI
FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
2014
Department of Medicine, Madigan Healthcare System and Uniformed Services
Department of Internal Medicine, University of Iowa Carver College of Medicine
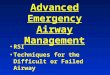
Techniques for the
Current opinion in critical care (Impact Factor: 2.67). 12/2012;
Oleh :
Faradhillah A Suryadi c11108340
Pembimbing :
dr. Maya P Suyata
Supervisor
dr. Fransiscus J.Manibuy, Sp.An-KIC

Introduction
Management of the difficult airway is associated with
significant morbidity and mortality in critically ill
patients.
An increasing array of advanced airway tools are
available, but appropriate selection and application
in the ICU remains poorly defined.
Difficult airway incidence during emergent intubation
is 10%, but complications of ICU airway
management remain common
the importance of interdisciplinary critical care team
preparation, training, and teamwork, and the
application of various advanced airway adjunct to
maximize intubation success and minimize com
plications in this environment

The Difficult Airway
ASA : difficult airway as the existence of clinical
factors that complicate ventilation by facemask or
intubation by experienced and skilled clinicians [5]
Jaber et al. [4] : complications in 50% of 253 ICU
intubations, 28% including severe complications
(serious hypoxemia, hemodynamic instability,
cardiac arrest or death)
Martin et al. [6] : Although 44% of these
complications occurred in the ICU, the proportional
rate of complications was significantly less than that
associated with intubations performed on a ward
(P<0.001).4. Jaber S, Amraoui J, Lefrant JY, et al. Clinical practice and risk factors for immediate complications of endotracheal intubation
in the intensive care unit: a prospective, multiple-center study. Crit Care Med 2006; 34:2355–2361.
5. American Society of Anesthesiologists. Practice guidelines for management of the difficult airway: an updated report by the
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003; 98:1269–1277.
6. Martin LD,Mhyre JM, Shanks AM, et al. 3,423 Emergency tracheal intuba at a University Hospital. Airway outcomes and
complications. Anesthesio 2011; 114:42–48.

Anatomy

Anatomy

Difficult Airway Management
Prediction Preparation Practice

Common risk factors associated with
a difficult airway
History Previous noted difficulties Large Tongue
Male Receding Jaw
Age 40–59 High Arched Palate
Diabetes Prominent uppers
incisors
Acromegaly Short thick neck
Rheumatoid arthritis Fixed or ‘high’ larynx
Obstructive sleep apnea Mouth opening <4 cm
Head and neck surgery, radiation Mallampati class 3 or 4
Physical exam Obesity
Upper airway trauma, burn, or swelling Reduced head/neck
mobility

Prediction
MALLAMPATI CLASSIFICATION
Class I: Soft and hard palate, tonsillar pillars, and uvula are well seen.
Class II: Tonsillar pillars and tip of the uvula are hidden.
Class III: Only soft and hard palates are visible.
Class IV: Only the hard palate is visible

Evaluating DMV
• Mask SealM
• Obesity/ ObstructionO
• No teethN
A
• StiffnessS
• Age

Evaluating DMV
• Over weight (body mass index > 26 kg/m2O
• BeardB
• Elderly (> 55 y.o)E
S
• EdentulousE
Snoring
a snoring (OBESE) Santa

Evaluating Difficult Intubation
LEMON or MELON scale
LM MAP
4 D
Wilson Risk Scale
Magboul 4M

LEMON Scale

Grading the Airway (Cormack-Lehane)
Grade I - Full view of the glottic opening
Grade II - Posterior portion of glottic opening visible
Grade III - Only tip of epiglottis is visible
Grade IV - Only soft palate is visible

Evaluating Difficult Intubation
• Look for external face deformitiesL
• MallampatiM
• Measure 3-3-2-1 fingersM
A
• Pathological obstructive conditionsP
Atlanto-occipital extension

4D
Dentition
Distortion
Disproportion
Dysmobility
4D

Wilson Risk Score
0 1 2
Weight <90 kg 90 – 110
kg
>110 kg
Head and
neck
movement
>90o 90o <90o
Jaw
movement
IG >5 cm
SL >0
IG <5 cm
SL = 0
IG <5 cm
SL < 0
Receding
mandible
Normal Moderate severe
Buck teeth Normal Moderate severe

4 M
M allampati
M easurement
M ovement
M alformation of STOPSkull,Teeth,Obstruction,Pathology
(kraniofacial abnormal & Syndromes: Treacher Collins, Goldenhar’s, Pierre
Robin, Waardenburg syndromes)


Preparation
Decide whether the basic problem is :
- Difficult ventilation
- Difficult intubation
- Uncooperative patient
Try more active to manage difficult airway
Consider the purpose of the management
- awake intubation vs intubation after induction
- Invasive or non-invasive intubation approach
- Decide the main strategy and always think about plan B

Practice
Stylets, Intubasi Guides and Bougies

Practice
Airway Exchange Catheter

Practice
Specialized Forceps

Practice
Direct Laryngoscopy

Practice
Laryngeal Mask Airway

Practice
Intubating Laryngeal Mask Airway


Practice
Video Laryngoscopy

Practice
Video Laryngoscopy

Practice
Advanced management in difficult airway
Retrograde intubation
Transtracheal Jet Ventilation
Cricothyroidotomy
Thoracostomy

Difficult airway management in the ICU
The Royal College of Anesthetists fourth National
Audit Project (NAP4) [7] : 20% airway incidents
occurred in the ICU, and 61% these episodes
resulted in death or significant neurologic injury.
the contributing factors to ICU airway management
complications: patient, staffing, training, equipment,
and environmental considerations.
Flavin K, Hornsby J, Fawcett J, et al. Structured airway intervention improves
safety of endotracheal intubation in an intensive care unit. Br J Hosp Med
2012; 73:341–344.

Equipments in drawers :
1st : Kateter suction Yankauer; Handle Laringoskop(besar dan kecil); Bilah laringoskop (Mac 3, 4, Miller,@, 3); Plester; Klem tube; Forsep Magill.
2nd : Drugs; syringe; ctistaloid; lubricant gel
3rd : Swivel adapters; stylets; dll
4th : Laringoscope fiber optic rigid.
5th : Oxygen Mask; guide wires (0,035); endotrachealtube (2-9); Cricothyrotomi set; retrograde intubation
6th : LMA ( ukuran 1-5); Disposable ambu bag; Oralairways; nasal trumpets; oral airways for fiberopticintubation; gum elastic bougie.
Flavin K, Hornsby J, Fawcett J, et al. Structured airway intervention improves
safety of endotracheal intubation in an intensive care unit. Br J Hosp Med
2012; 73:341–344.
Difficult Airway Cart



Conclusion
A systematic approach to intubation management
that emphasizes planning, preparation, and team-
work can significantly reduce intubation
complications.
Management of Difficult airway must apply the
general principles available from current medical
evidence
American Society of Anesthesiologists. Practice guidelines for management of the difficult airway: an updated
report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway.
Anesthesiology 2003; 98:1269–1277.

You
BAGIAN ILMU ANESTESI, PERAWATAN INTENSIF, DAN MANAJEMEN NYERI
FAKULTAS KEDOKTERAN UNIVERSITAS HASANUDDIN
2014
Thank