Embed Size (px)
Citation preview
Terapeuticas hormonaissão ou não
Preventivas de DCV da mulher?
Manuel Neves-e-Castro(Sociedade Portuguesa de Menopausa)
Janeiro 2002
After all ...
“Only 20% of women who startHRT seem to continue treatmentafter 4 years”.
Pilon D, Castilloux A, Le Lorier J. Obstet Gynecol2001;97:97-100.
White woman’s risk of death betweenthe ages of 50 and 94 are:
31.0% from heart disease
2.8% from breast cancer
2.8% from hip fracture
Brinton LA, Schairer C. N Engl J Med.1997;336:1769-1775
Estrogens and LipidsFavorable effects through the liver:- inibition of lipoprotein lipase- stimulation of the production of HDL –C
- stimulation of the synthesis of Apo-A¹- stimulation of the uptake of LDL-C
- stimulation of the uptake of chylomicrons- increased secretion of VLDL
- increased secretion of bile acids
- increased triglycerides (slight)
Estrogens and Lipids
Female sex steroids prevent LDL oxidation in vivo and consequent arterial wall injury.
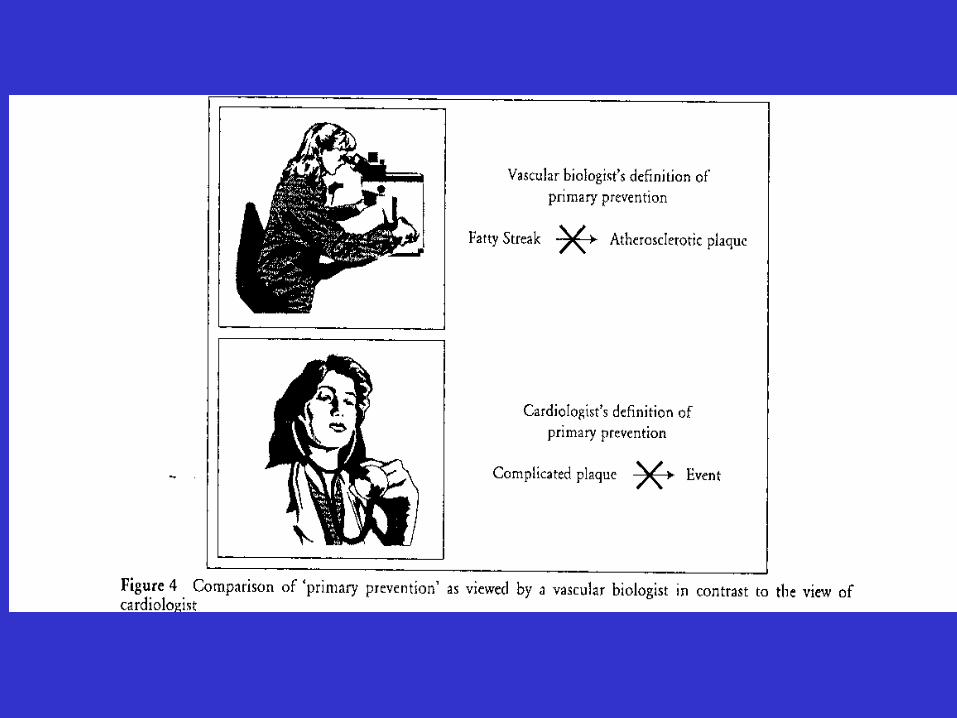
Lipid-lowering therapy promotes clinically stable plaque
- Prolonged intensive lipid-lowering therapy is associated with a markedly decreased lipid content in carotid atherosclerotic plaques
- The clinical implication of this is that the low plaque lipid composition would predict greater plaque stability, and would thus reduce clinical ischemic events such as myocardial infarction or stroke.
Zhao X-Q et al. Arterioscler Thromb Vasc Biol 2001;21:1623-1629,1563-1564 (October)
Estrogens, Lipids and Vascular System
The majority of the positive effects on the vascular system are non-lipid related
Estrogens and Vascular System
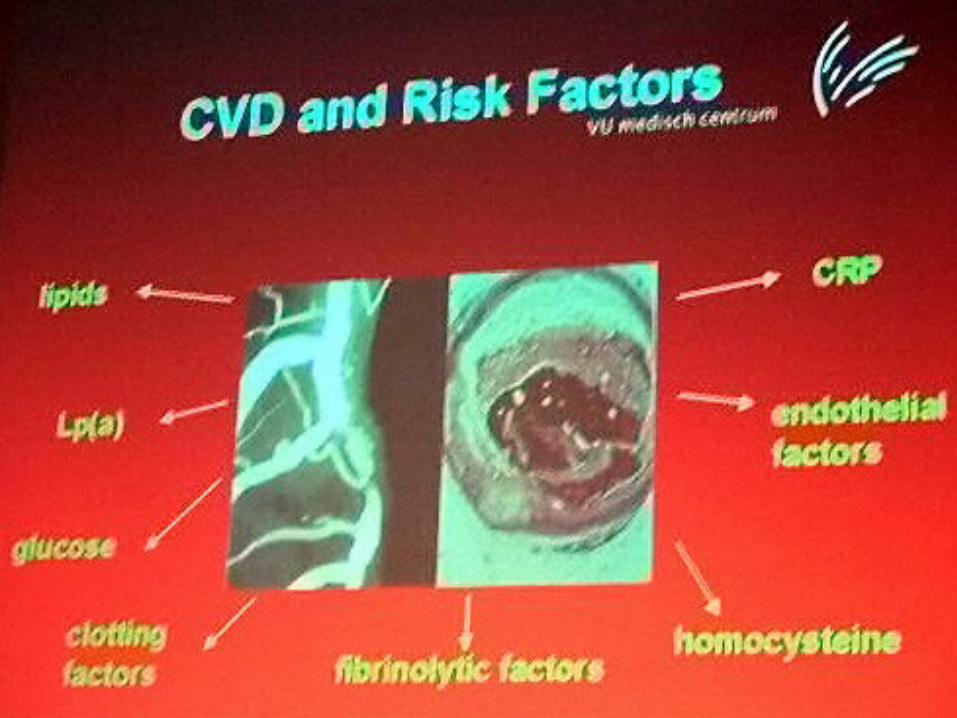
Estrogen may positively influence all the steps involved in the formation of the atherosclerotic plaque (accumulation of cholesterol in the arterial wall, arterial smooth muscle cell proliferation, platelet aggregation, collagen and elastin production)
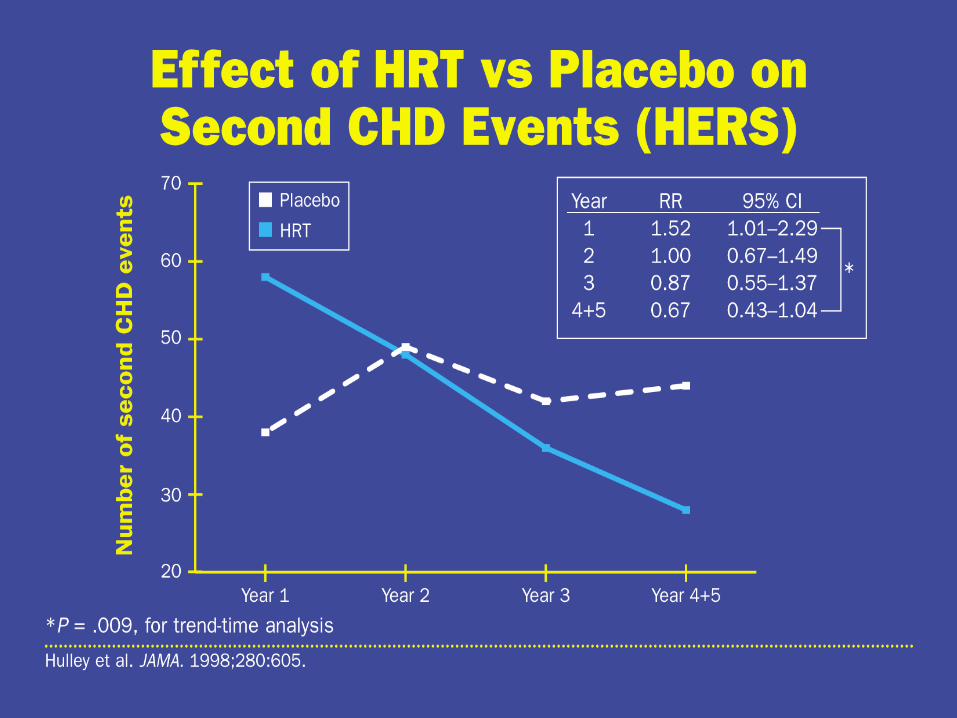
“The HERS trial”
Letter to the Editor
Neves-e-Castro M.Climacteric 1999;2:59
“On the basis of data from randomized clinical trials, hormone-replacement therapy does not appear to reduce the risk of cardiovascular events in women with established coronary heart disease”.Manson JA, Martin KA
N Engl J Med.2001;345:34-40
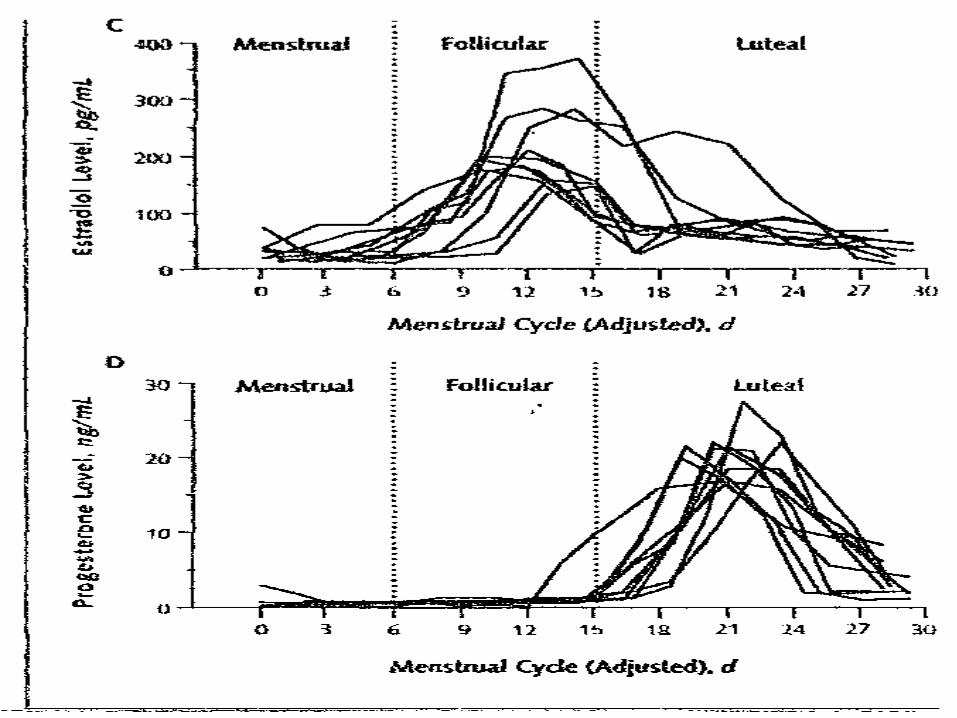
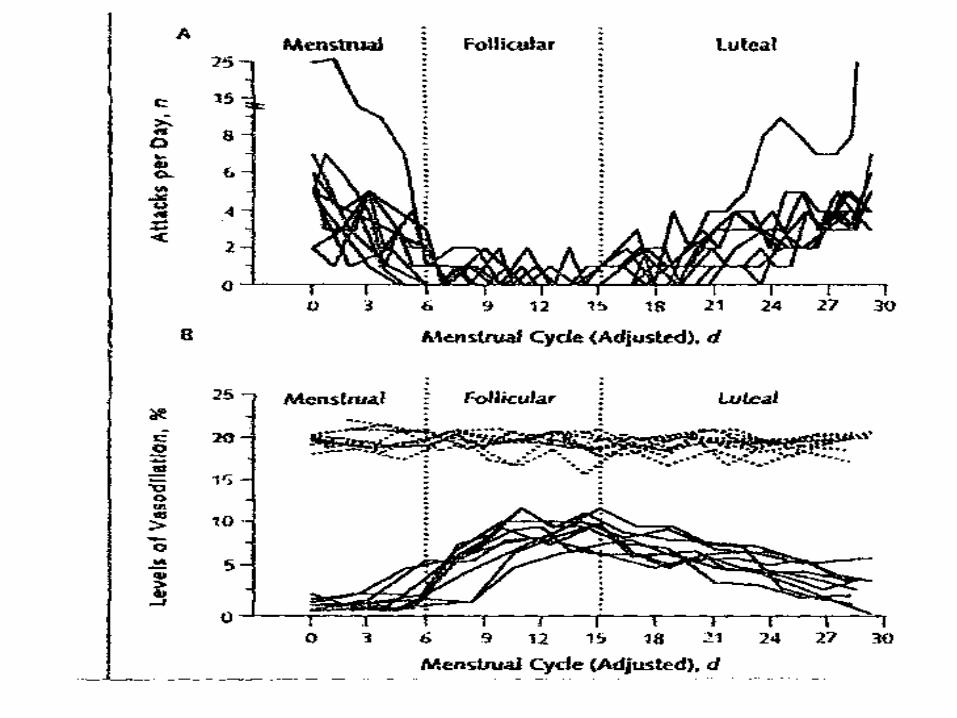
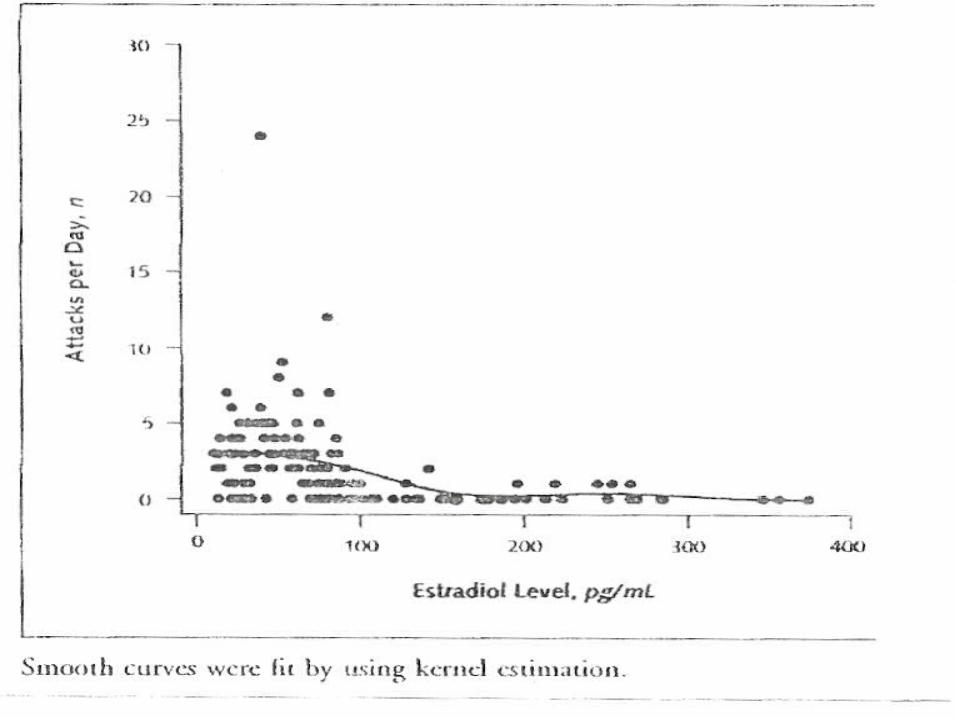
“The Effect of Treatment with Estradiol and Norethisterone Acetate on Exercise Tolerance and on the Frequency and Severity of Ischemic Attacks in Postmenopausal Women with Stable Angina Pectoris”.
Sanderson JE et al.J Cardiovasc Pharmacol 2001;38(3):372-383
Estrogens and Vascular System
“The total number of ischemic events/24 h during ambulatory electrocardiographic monitoring decreased by 0.82 events after treatment compared with an increase in the placebo group (0.94), a highly significant difference (p=0.006)”.
Sanderson JE et al.J Cardiovasc Pharmacol 2001;38(3):372-383
“This particular combined hormone replacement preparation may have a beneficial effect on myocardial ischemia in postmenopausal women with established coronary disease”.
Sanderson JE et al.J Cardiovasc Pharmacol 2001;38(3):372-383
“Reduced risk of cardiovascular events even within the first year of HRT in a retrospective case-control study of 1200 women with myocardial infarction compared with 5000 controls”.
Varas-Lorenzo C, Garcia-Rodriguez LA. Perez-Gutthann S, et al
Circulation 2000;101:2572-2578
“HRT is associated with a 35% reduction in mortality for women who suffered myocardial infarction”.
Shlipack MG, Angeja B, Go AS, et al
Circulation 2001;104:2300-2304
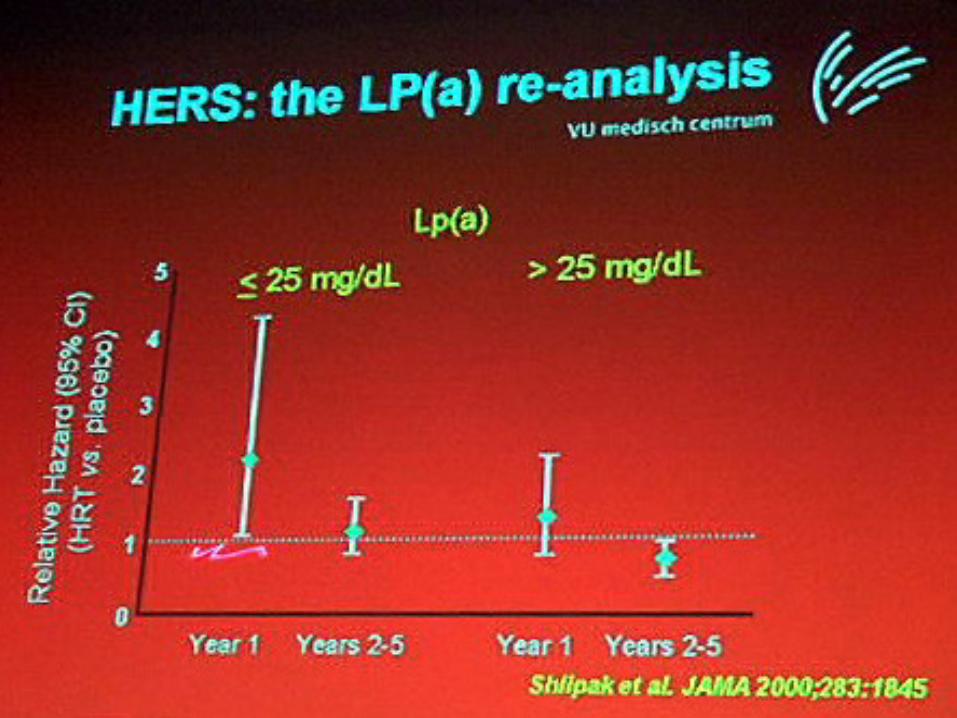
“CEE + MPA appeared to have a more favorable effect in women with high initial lipoprotein (a) levels than in women with low levels”.
Shlipack MG, Simon JA, Vittinghoff E, et al
JAMA 2000;283:1845-1852
“The Nurse’s Health Studyinvestigation of primary preventionindicates that hormone therapymay be associated with coronarybenefits”.
Grodstein F, Manson JE, Colditz GA, et al. Ann Intern Med2000;133:933-41
“Combined hormone replacement therapy improves endothelial function in healthy post-menopausal women”.
Gužič-Salobir B, Keber I, Seljeflot I, et al
J Intern Med 2001;250:508-515
“When are observational studies adequate evidence”?
Grady D. and Hulley SB. Ann Intern Med 2000;133:999-1001
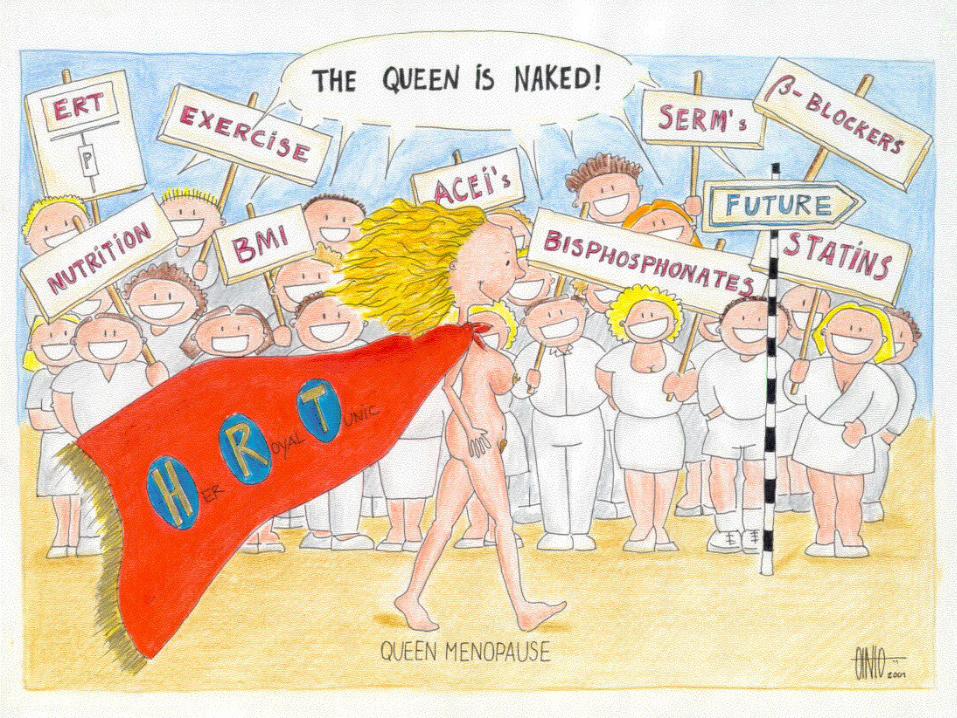
“The Queen ... is naked!”
Critical Comment
Neves-e-Castro M..Maturitas 2001;38:235-237
“The HERS Study, as interpreted by a practitioner, is nothing but a phase III Study of a particularproduct (0.625 mg of conjugated equine estrogens plus 2.5 mg of medroxyprogesterone acetate, in one tablet daily)”.
Neves-e-Castro M. Maturitas 2001;38(3):235-237
Grady D, Hulley SB. Ann Intern Med 2000;133:999-1001
“The protocol of the study does not reflect good clinical practice”.
Neves-e-Castro M. Maturitas 2001;38(3):235-237
“The higher rate (thromboticevents) is probably a consequence of the facts that women involved in HERS were older and had multiple risk factors”.
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“HRT decreased or increased atherothrombosis depending on the presence of factor V Leiden mutation”
Glueck CJ, Wang P, Fontaine RN, et al
Am J Cardiol 1999;84:549-554
“Primary CHD occurred only in172 of the 1380 women in thehormone group and in 176 of the1383 women in the placebogroup”.
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“For women who stopped taking HERS medication, the risk of primary CHD events was elevated in the first month after stopping use of the medication”?!
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“The RH comparing risk of theprimary CHD outcome in thehormone and placebo group wassimilar”.
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“Total mortality in the hormone group was not significantly different from that in the placebo group (131 vs. 123 women)”.
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“HERS did not evaluate the effect of estrogens plus progestin therapy, in women without CHD, and it is not known whether our findings applyto healthy women. It is also not known whether the use of different progestin or of estrogens alone would have been beneficial”. Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“The discrepancy between the finding of HERS and the observational studies may also reflect important differences between the study populations and treatments”.
Hulley S, Grady G, Bush T, et al. JAMA 1998;280:605-13
“Perhaps post-menopausal hormone therapy is beneficial in women who have not yet developed coronary disease but not in women who already have it”.
Grady D, Hulley SB. Ann Intern Med 2000;133:999-1001
“Numerous observational studies have reported lower CHD rates in postmenopausal women receiving estrogen than in those who did not”.
“The strongest association was in postmenopausal women with CHD; estrogen users had 35% to 80% fewer recurrent events than nonusers”.
LaRosa JC-Circulation 2001;104:1688-1692
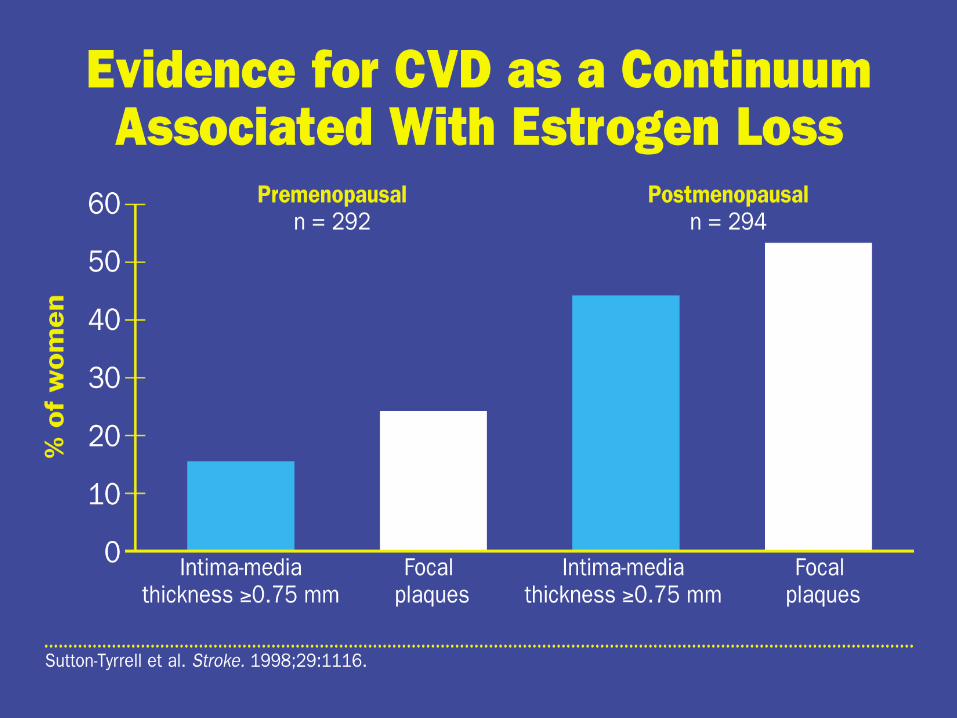
Vascular benefits of HRT limited to women without atherosclerosis
“Estrogen may be more effective for maintenance of vascular health than it is for treatment of established vascular disease”.
Herrington DM et al;Arterioscler Thromb Vasc Biol 2001;21:1867-1869,1955-1961
“Early intervention in the progression of atherosclerosis, especially at the start of menopause, may be the key to successful prevention of cardiovascular disease with HRT”.
Hodis HN, Mack WJ, Lobo RA, et al
Ann Intern Med. 2001;135:939-953
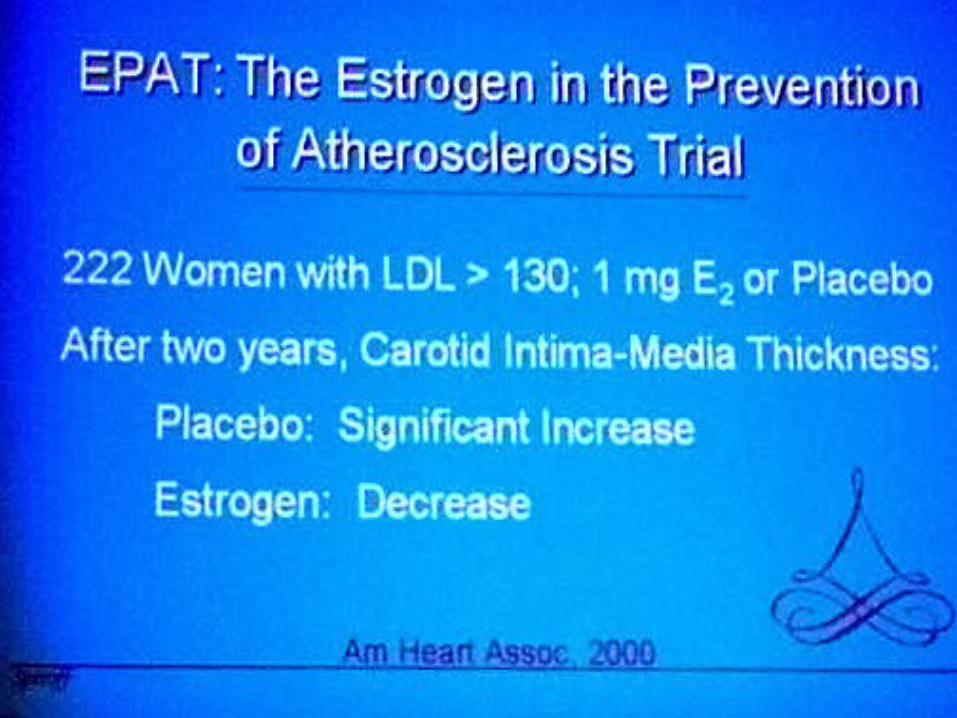
“The average rate of progression of subclinical atherosclerosis was slower in healthy postmenopausal women taking unopposed ERT with 17ß-estradiol than in women taking placebo”.
Hodis HN, Mack WJ, Lobo RA, et al
Ann Intern Med. 2001;135:939-953
“The risk for major coronary events was lower among current users of hormone therapy, including short-term users, compared with never users [(relative risk, 0.61 (95% CI, 0.52-0.71)]”.
Grodstein F. et al.Ann Intern Med 2000;133:933-41
CGHFBC. Lancet 1997; 350:1047-1059
“The findings of HERS should notdiscourage the use of hormonereplacement therapy in the primaryprevention of cardiovasculardisease”.
Tolbert T. and Oparil S. Circulation 2001;103:620-2
Editorial
The time has come to stop letting the HERS Tale Wag the Dogma
Michael E. Mendelson,; Richard H. Karas,
Circulation 2001;104:2256-2259
“We believe there has been enormous overinterpretation and misinterpretation of recent clinical data (the HERS tale) with regard to the efficacy of hormone replacement therapy (HRT) in preventing or diminishing the risk of heart disease (the dogma)”.
“Hormone Replacement Threrapy and Cardiovascular Disease”.
A Statement for Healthcare Professionals From the American Heart Association.
Mosca L et al;Circulation.2001;104:499-503
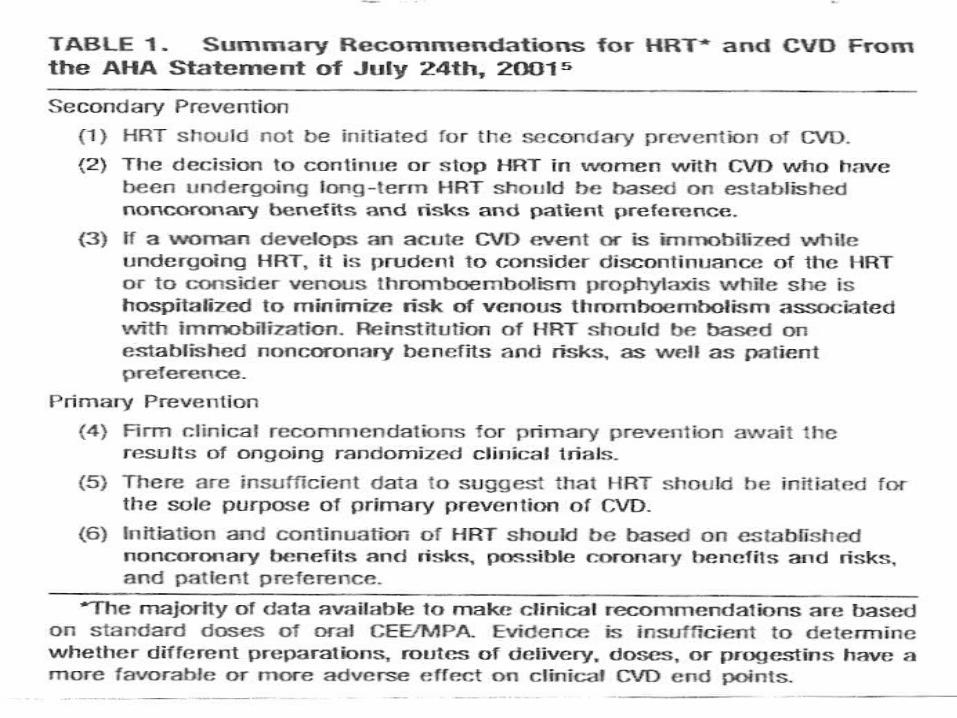
“Hormone Replacement Therapy and Cardiovascular Disease”.
“There are insufficient data to suggest that HRT should be initiated for the sole (?) purpose of primary prevention on CVD” (Circulation 2001)
“Hormone Replacement Therapy and
Cardiovascular Disease”. The majority of data available to make clinical
recommendations are based on standard doses of oral CEE/MPA. Evidence is insufficient to determine whether different perparations, routes of delivery, doses, or different progestins have a more favorable or more adverse effect on clinical CVD end points” (Circulation 2001)
“Hormone Replacement Therapy and
Cardiovascular Disease”.
“In conclusion, recommendations such as these of the AHA (Circulation 2001),writen as they are, may be less helpful than intended, both for clinicians and women”.
Neves-e-Castro M.The ImaginaryWoman, Maturitas 2001;40:8-9
“All medical interventionsshould be individualised to thespecific woman’s age,characteristics and needs”.
Genazzani AR, Gambacciani M. IMS Expert Workshop,Climacteric 2000;3:233-240
The important issue, after all, is not HRT.
What is important is the best possible approach to preventive medicine in a middle aged-woman.
Neves-e-Castro M.(2000)
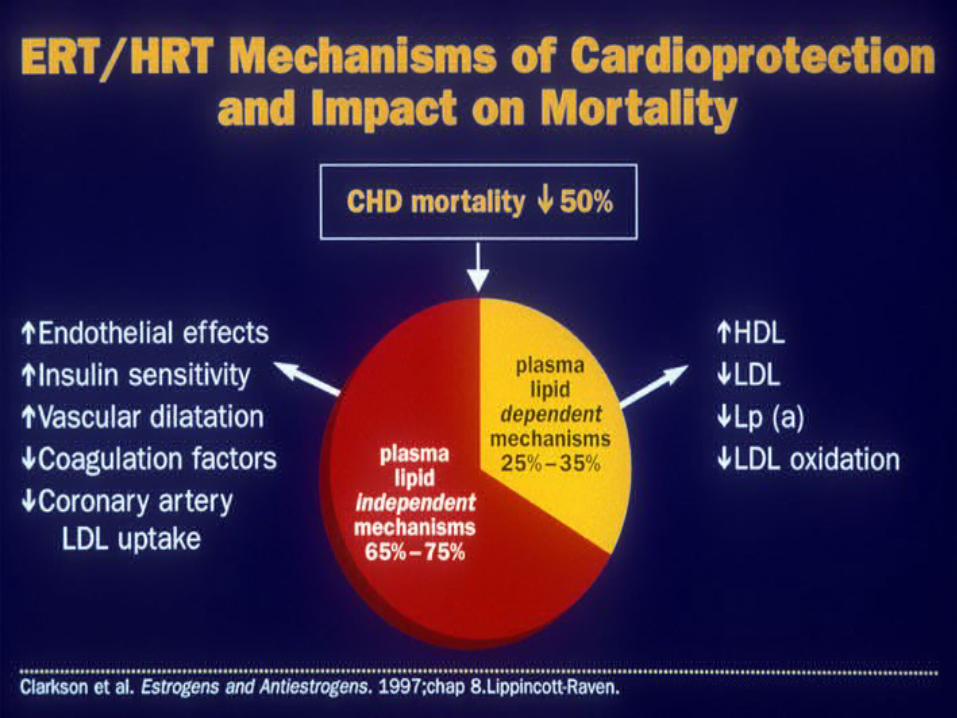
“It appears that half of thebenefits in the prevention ofcardiovascular diseases are nothormone related”!
Mosca L, Grundy SM, Judelson D, et al. Circulation1999;99:2480-4
Menopausal hormonal treatments are very good.
but
Treatments without hormones may also be very good for a woman’s health
“When hormone replacement therapy is not possible”
Neves-e-Castro M in “The Management of the Menopause” The Millennium Review 2000” Ed.John Studd; Parthenon, NY 2000
“Every discussion about the Menopause (the Queen...) seems to implicate that there is nothing but HRT!”
Neves-e-Castro M. Maturitas 2001;38(3):235-237
A RaínhaMenopausa
vai nua!...
The take home message
The prescription of long-term hormonal treatments must depend always on a benefit/risk analysis in comparison with other non-hormonal medications and strategies.
Preventing a woman from the
benefits of a sound postmenopausal hormone therapy because of the fear of rare side effects does not seem to be satisfactory Medicine...
MNC 3/01
Há
só
uma
Medicina!
A Woman
in the autumn of her life
deserves an indian summerrather than a winter of a discontent ...
Robert B Greenblatt





![Metodos contraceptivos hormonais[1]](https://img.pdfslide.net/doc/110x75/5571f1e949795947648bcbae/metodos-contraceptivos-hormonais1.jpg)