Embed Size (px)
Citation preview

SSD Diabetologia ASL 1
Massa e Carrara
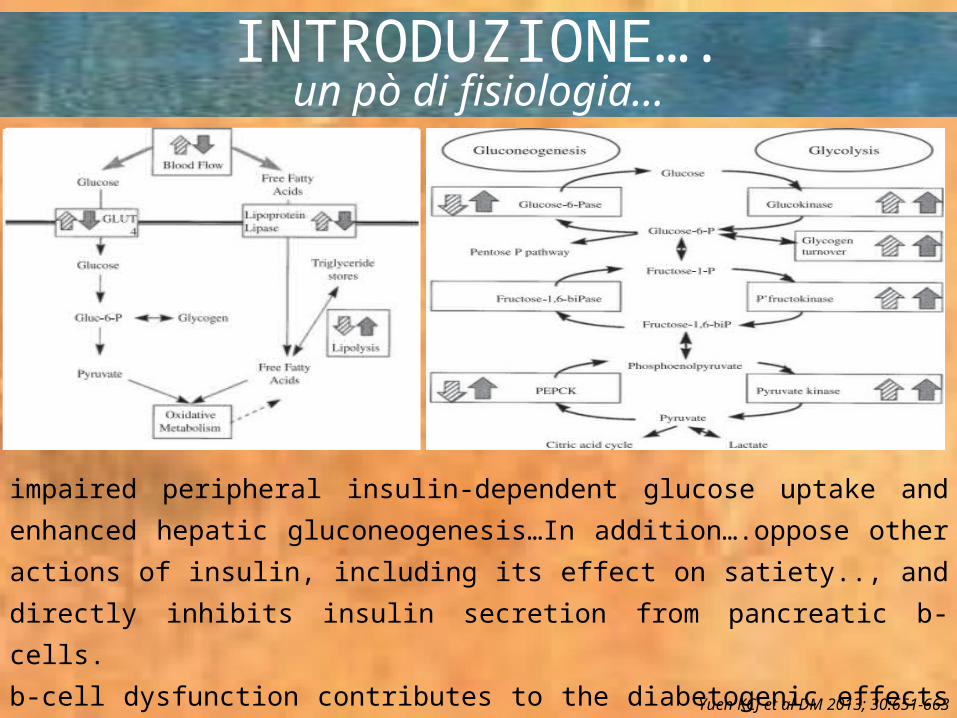
INTRODUZIONE….un pò di fisiologia…
Yuen KCJ et al DM 2013; 30:651-663
impaired peripheral insulin-dependent glucose uptake and enhanced hepatic
gluconeogenesis…In addition….oppose other actions of insulin, including its effect on
satiety.., and directly inhibits insulin secretion from pancreatic b-cells.
b-cell dysfunction contributes to the diabetogenic effects of GCs is less clear…
…may also affect pancreatic a-cell function and impair the insulinotrop- ic actions of
incretins

COSA DICONO LE LINEE GUIDA?
DC 2009; 32 (6):119
….Several approaches have been proposed for treatment of this condition, but no published protocols or studies have investigated the efficacy of these approaches. A reasonable approach is to institute glucose monitoring for at least 48 h in all patients receiving high-dose glucocorticoid therapy and to initiate insulin therapy as appropriate…. In patients who are already being treated for hyperglycemia, early adjustment of insulin doses is recommended... Importantly, during corticosteroid tapers, insulin dosing should be proactively adjusted to avoid hypoglycemia.

COSA DICONO LE LINEE GUIDA?
2012; 97 (1):16-38

COSA DICONO LE LINEE GUIDA?
Can J Diab 2014; 38:134-138
4. Patients treated with prednisolone once daily in the morning can receive concurrent NPH insulin subcutaneously, dosed as follows: 1 unit per 1 mg of prednisolone for the first 20 mg, then 0.5 unit per mg of prednisolone for the next 20 mg, then 0.25 unit per mg of prednisolone beyond 40 mg (33).5. Patients receiving dexamethasone or prednisone dosed every 8 to 12 hours should receive basal insulin (NPH twice daily or basal analogue insulin once daily), along with bolus insulin with meals plus a correction-dose insulin algorithm.6. Patients who are naive to insulin should be started on basal insulin at a dose of 0.3 units/kg/day and bolus insulin at 0.1 units/kg/meal (25).7. The correction-dose insulin algorithm is a critical component of management so as to avoid escalating hyperglycemia, and daily adjustments of the routine insulin doses are necessary.

COSA DICONO LE LINEE GUIDA?
prednisone e prednisolone hanno un picco d’azione a 4-6 ore e una durata di effetto sulle glicemie di circa 12 ore ovvero un profilo simile alla farmacocinetica dell’insulina NPH

COSA DICONO LE LINEE GUIDA?
Quando viene impiegato il desametasone, il cui effetto iperglicemizzante è più protratto, viene consigliato l’impiego dell’insulina glargine o detemir, la cui farmacocinetica risulterebbe la più idonea
In uno studio retrospettivo di confronto tra insulina NPH e insulina glargine come insuline basali in soggetti ospedalizzati e trattati con prednisone le due insuline hanno dimostrato uguale efficacia e uguale rischio ipoglicemico con necessità di un dosaggio insulinico minore nel gruppo in trattamento con NPH
E’ bene ricordare che i pazienti trattati con steroidi
che necessitano di uno schema insulinico basal
bolus presentano un maggior fabbisogno di insulina
prandiale rispetto all’insulina basale (in genere 70%
del fabbisogno insulinico totale come insulina
prandiale e 30% come insulina basale).

ma insomma che dobbiamo fare?
DC 2013; 36(7):1807-1814
Provocazione…….
basal bolus con premiscelata a
pranzo???




























![corticosteroid treatment or such treatment is not [Box I]](https://img.pdfslide.net/doc/110x75/616882e5d394e9041f701604/corticosteroid-treatment-or-such-treatment-is-not-box-i.jpg)
