Embed Size (px)
Citation preview

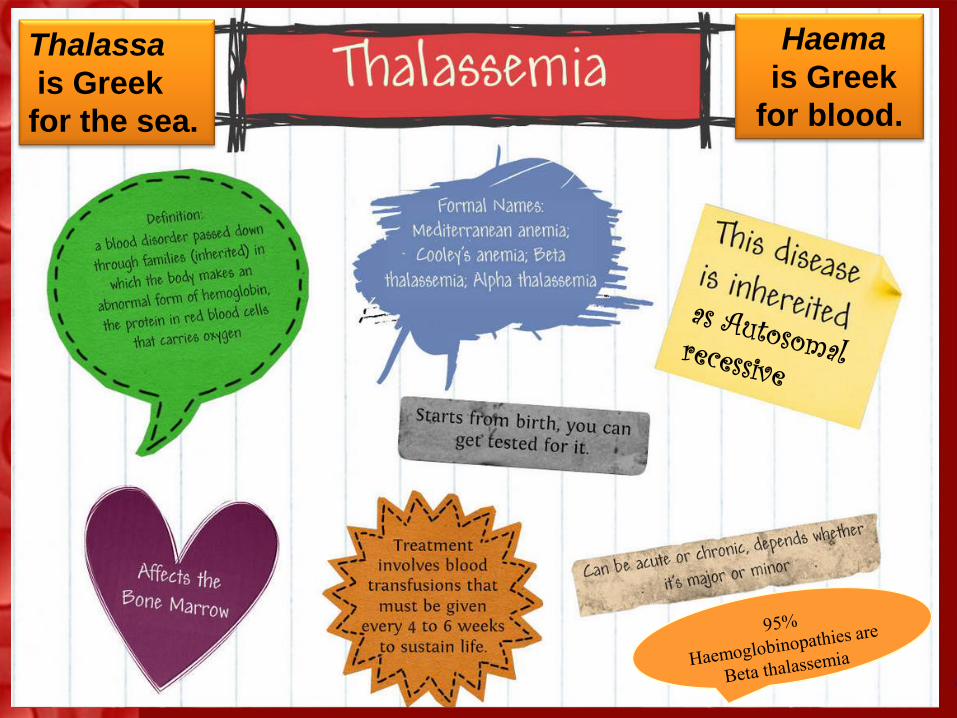
Haema
is Greek
for blood.
Thalassa
is Greek
for the sea.
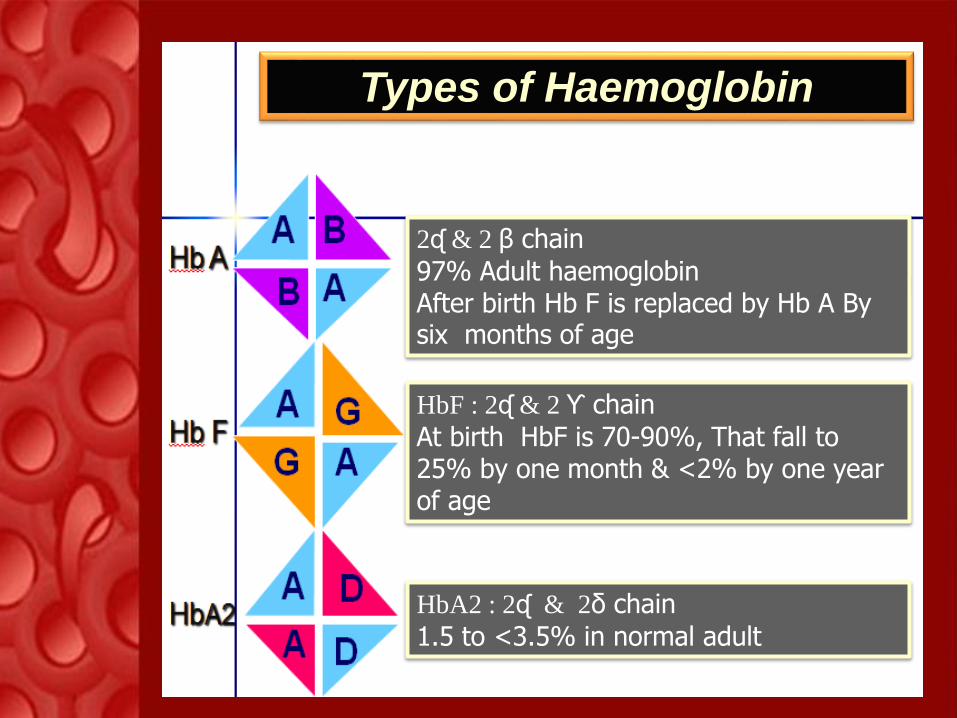
2ᶑ & 2 β chain
97% Adult haemoglobinAfter birth Hb F is replaced by Hb A By six months of age
HbF : 2ᶑ & 2 ϒ chain
At birth HbF is 70-90%, That fall to 25% by one month & <2% by one year of age
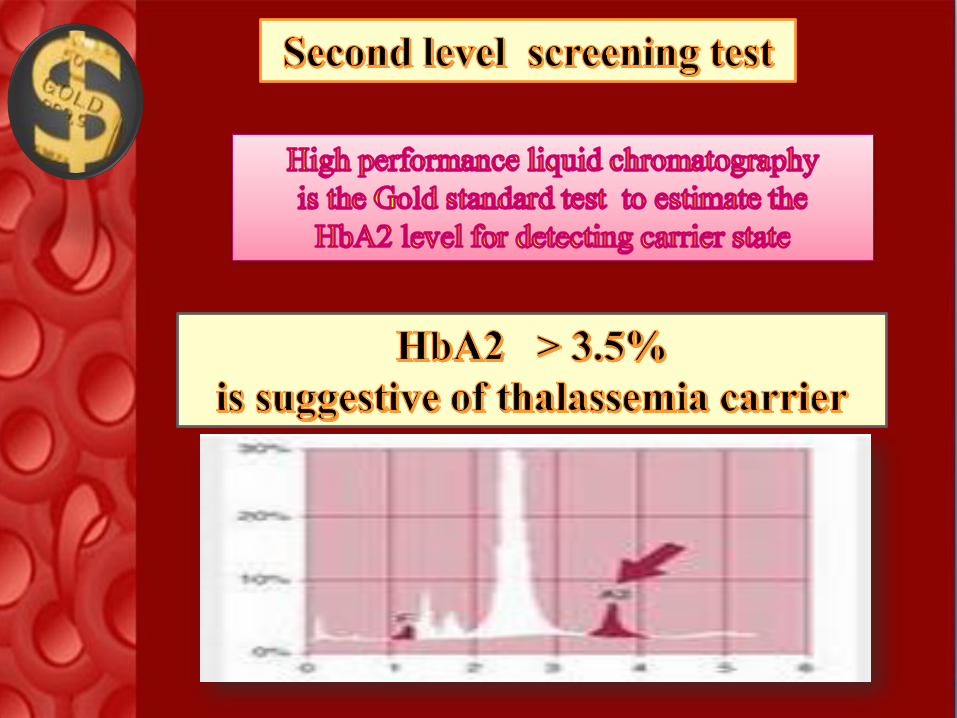
HbA2 : 2ᶑ & 2δ chain
1.5 to <3.5% in normal adult
Types of Haemoglobin
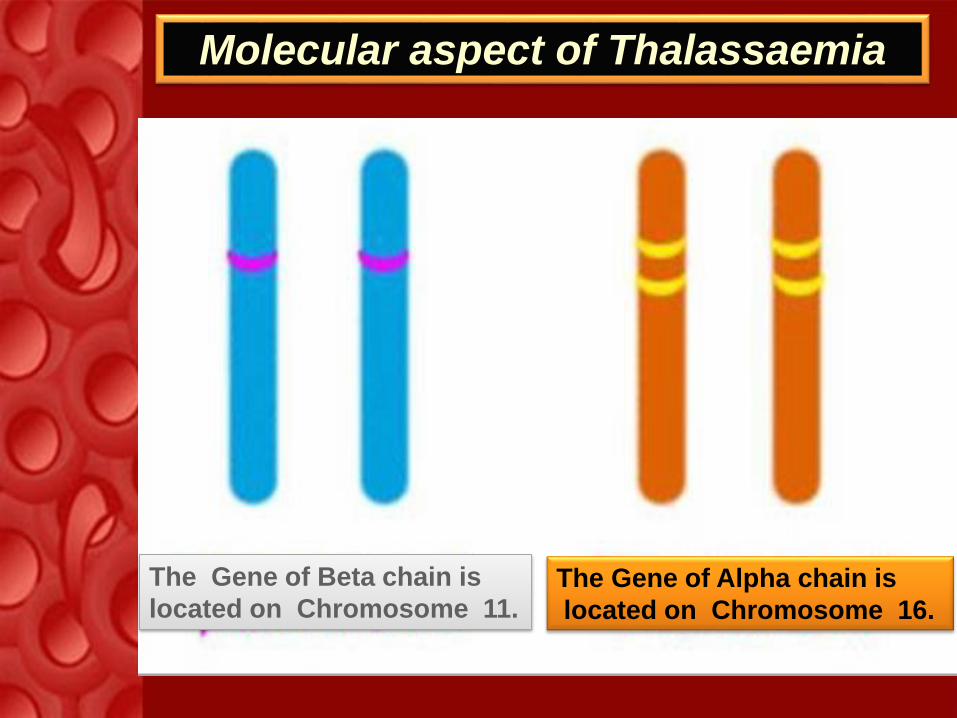
The Gene of Alpha chain is
located on Chromosome 16.
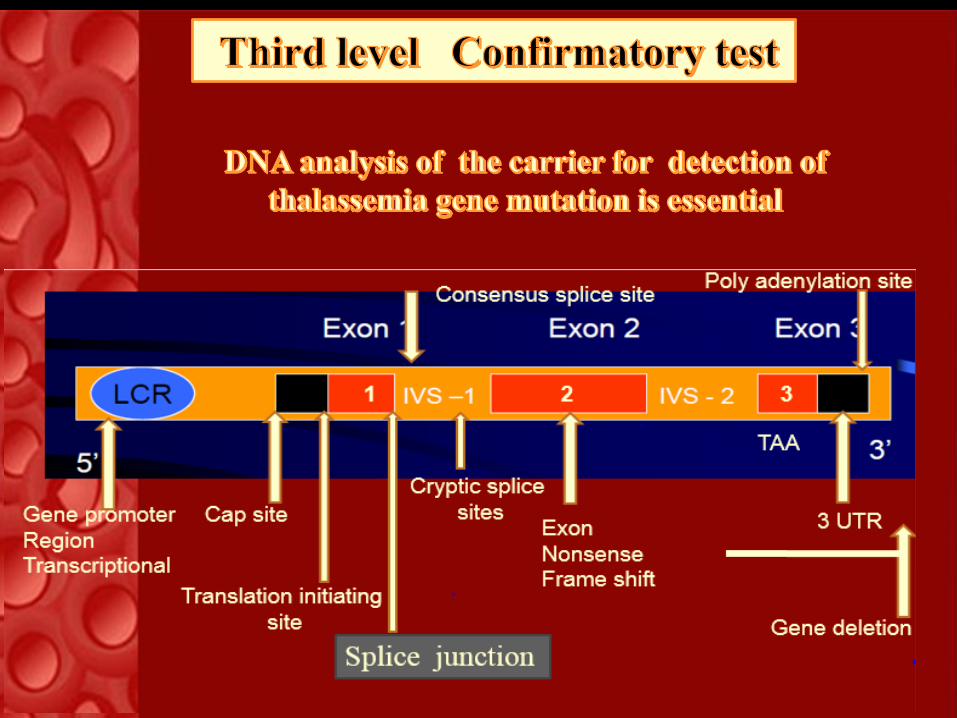
Molecular aspect of Thalassaemia
The Gene of Beta chain is
located on Chromosome 11.
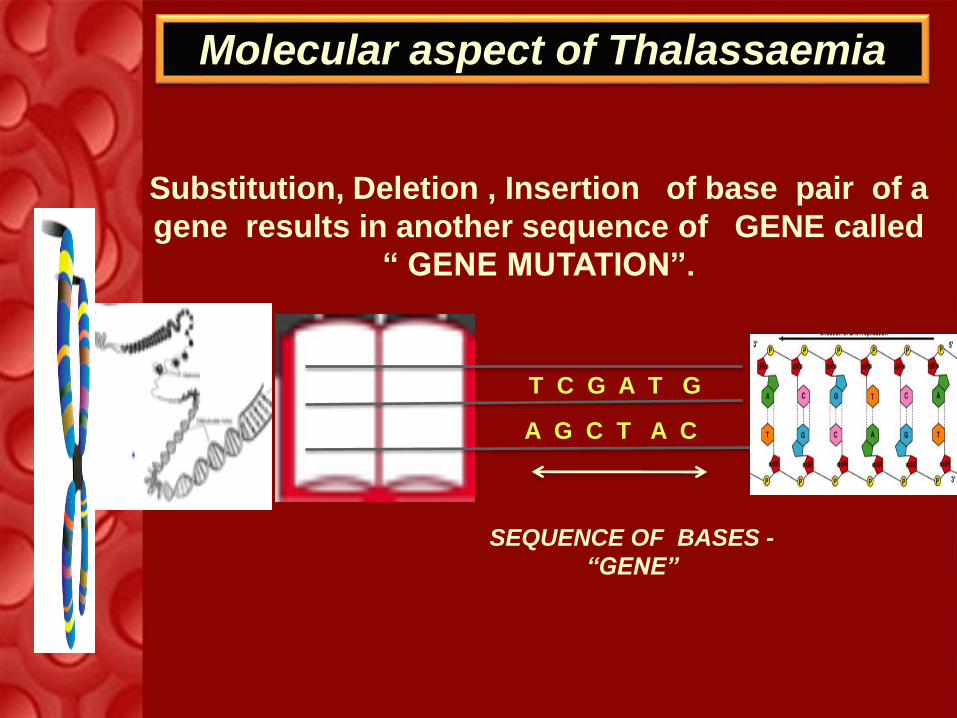
SEQUENCE OF BASES -
“GENE”
Molecular aspect of Thalassaemia
T C G A T G
A G C T A C
Substitution, Deletion , Insertion of base pair of a
gene results in another sequence of GENE called
“ GENE MUTATION”.
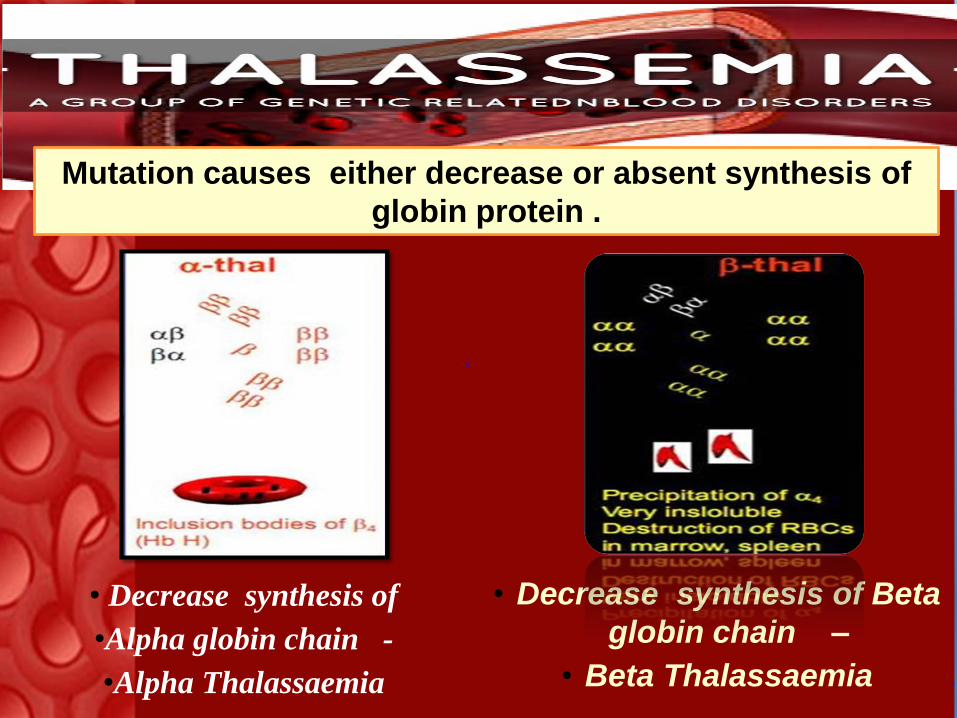
Mutation causes either decrease or absent synthesis of
globin protein .
• Decrease synthesis of Beta
globin chain –
• Beta Thalassaemia
• Decrease synthesis of
•Alpha globin chain -
•Alpha Thalassaemia
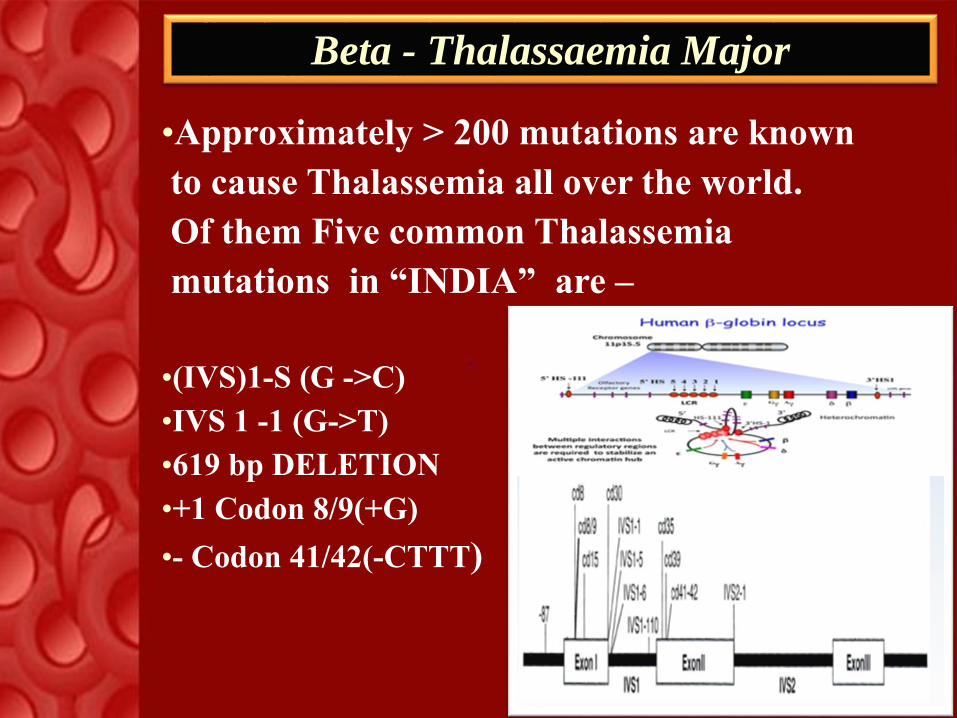
•Approximately > 200 mutations are known
to cause Thalassemia all over the world.
Of them Five common Thalassemia
mutations in “INDIA” are –
•(IVS)1-S (G ->C)
•IVS 1 -1 (G->T)
•619 bp DELETION
•+1 Codon 8/9(+G)
•- Codon 41/42(-CTTT)
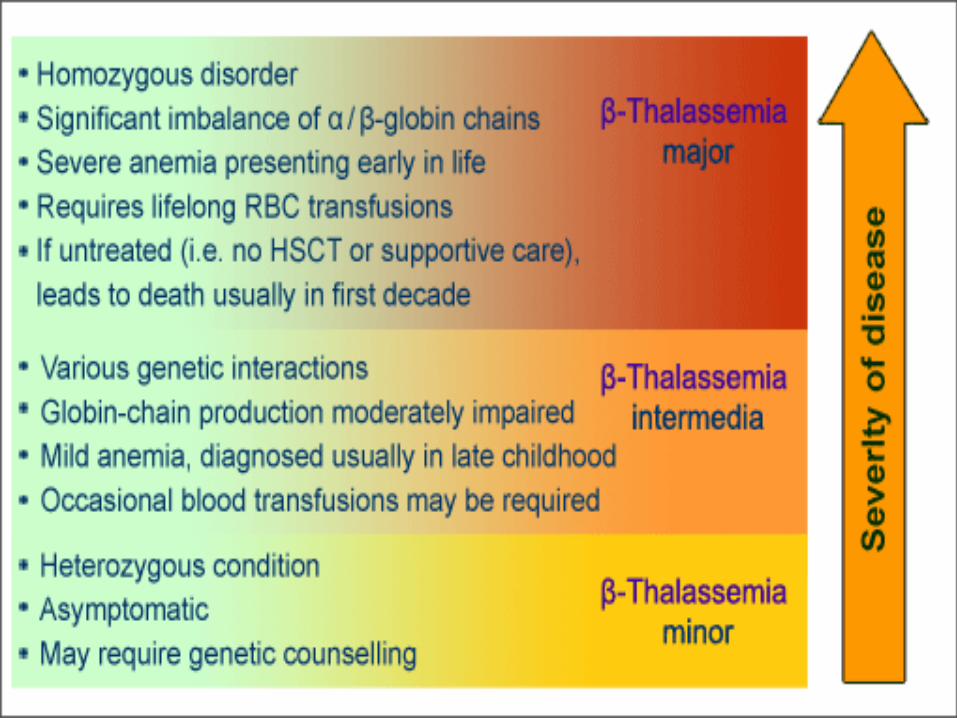
Beta - Thalassaemia Major
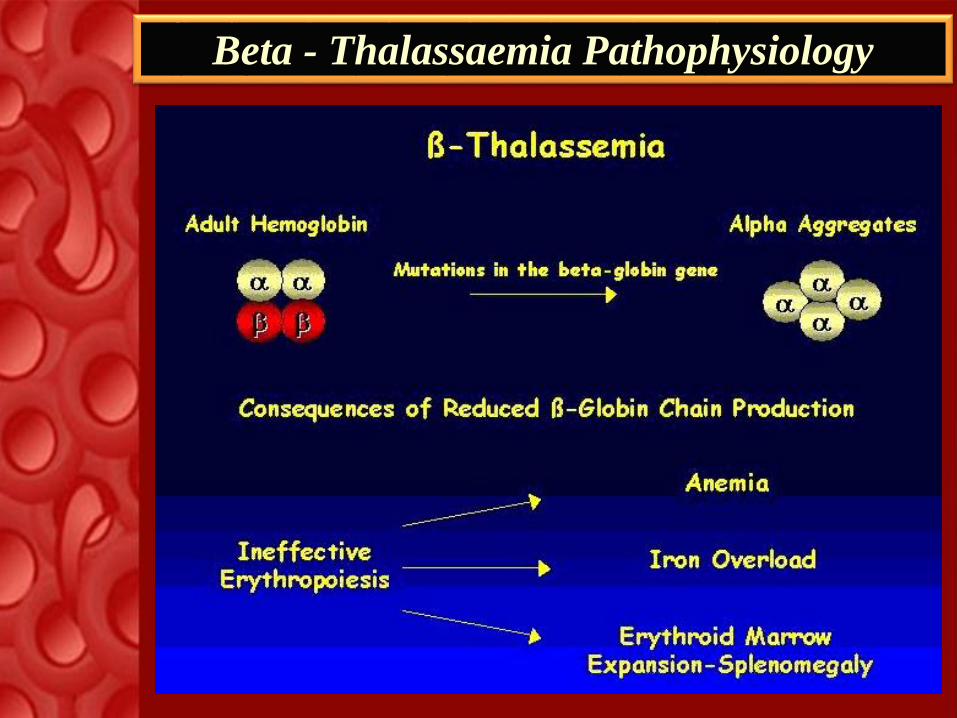
Beta - Thalassaemia Pathophysiology
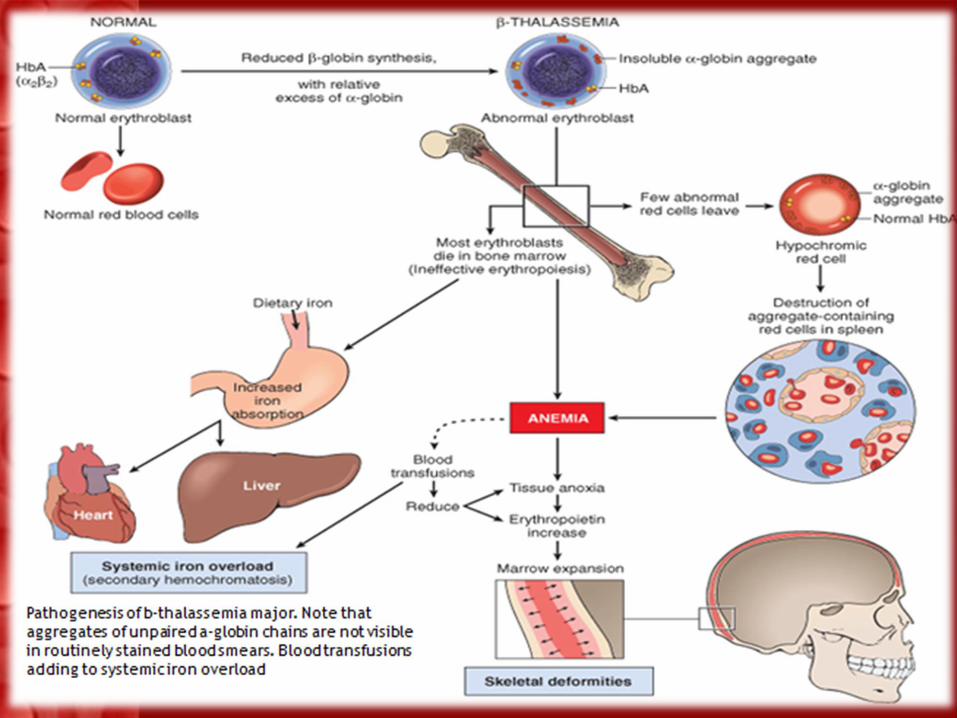
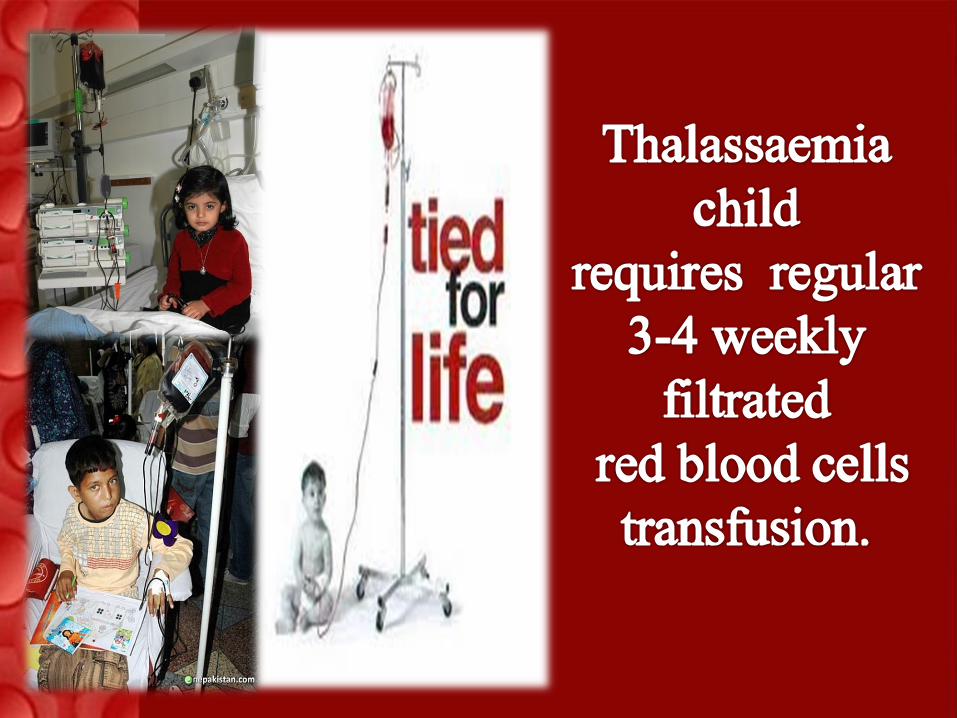

Repeated BT causes iron load.
Desferoxamine is Given S.C. for 8 hours
every day for 5-6 days a week so as to chelate
iron load.
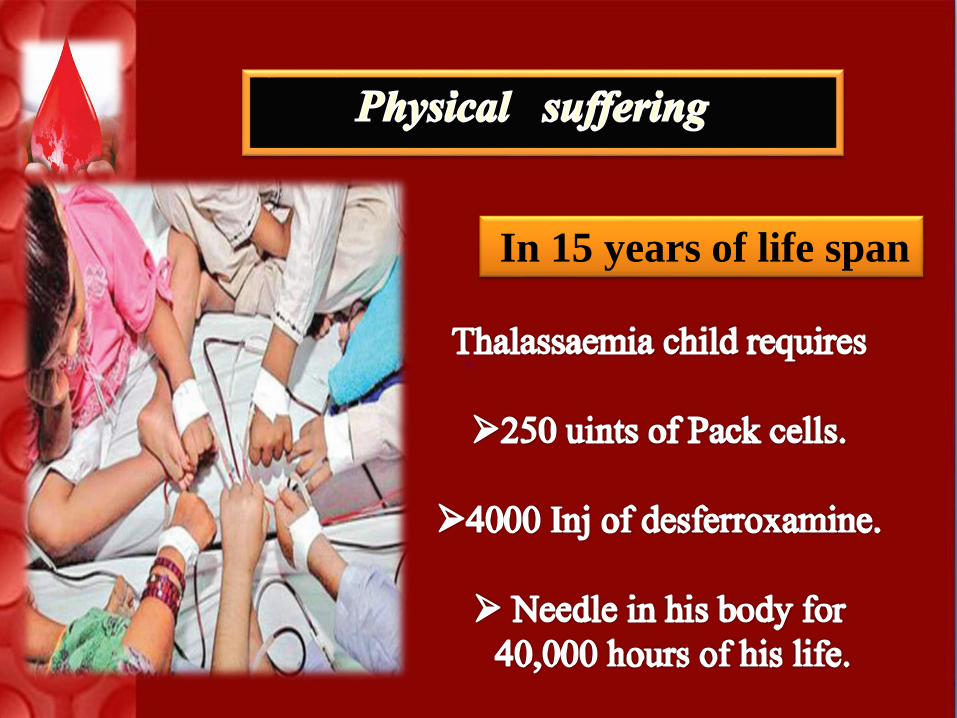
In 15 years of life span

Preventing the Birth of a
“Thalassaemia” child is the only
answer to this world wide problem
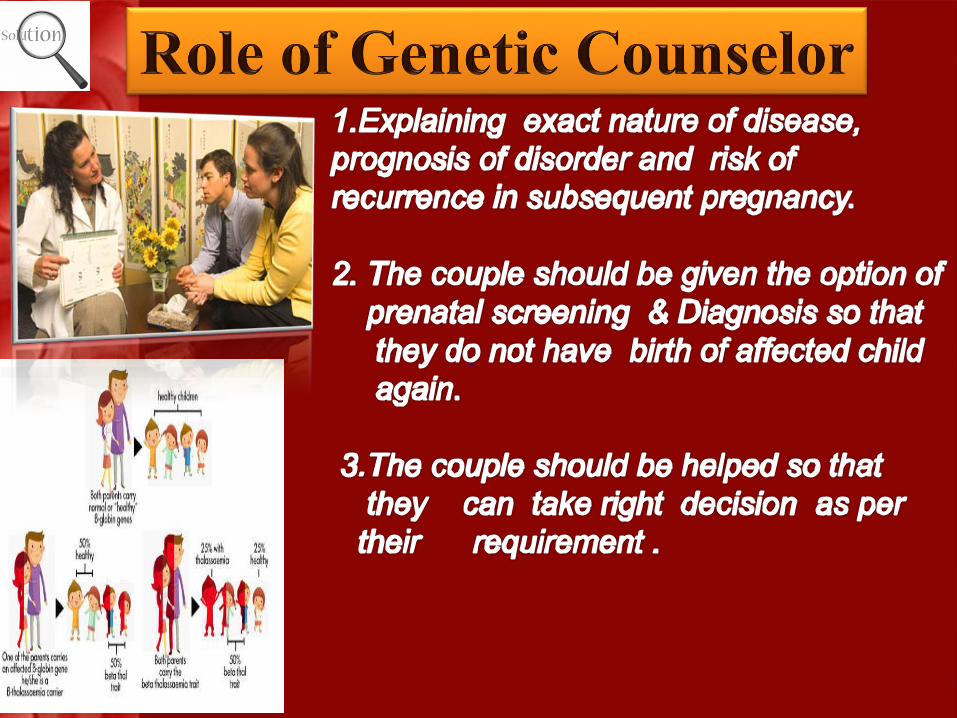
How does the birth of a thalassemia
child occur ?
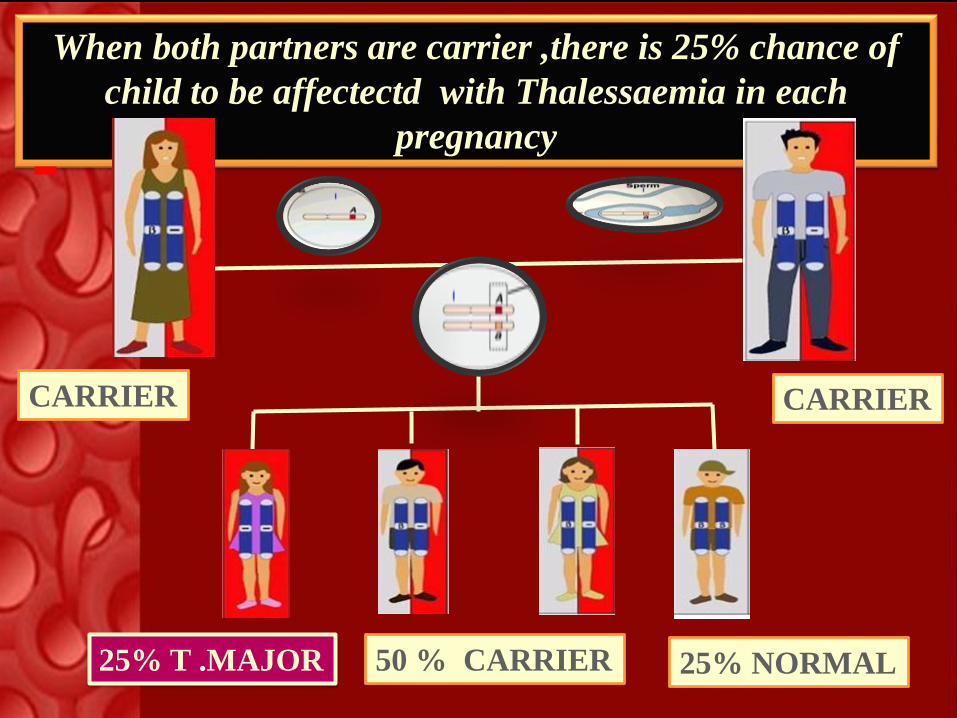
When both partners are carrier ,there is 25% chance of
child to be affectectd with Thalessaemia in each
pregnancy
CARRIER
50 % CARRIER 25% NORMAL25% T .MAJOR
CARRIER
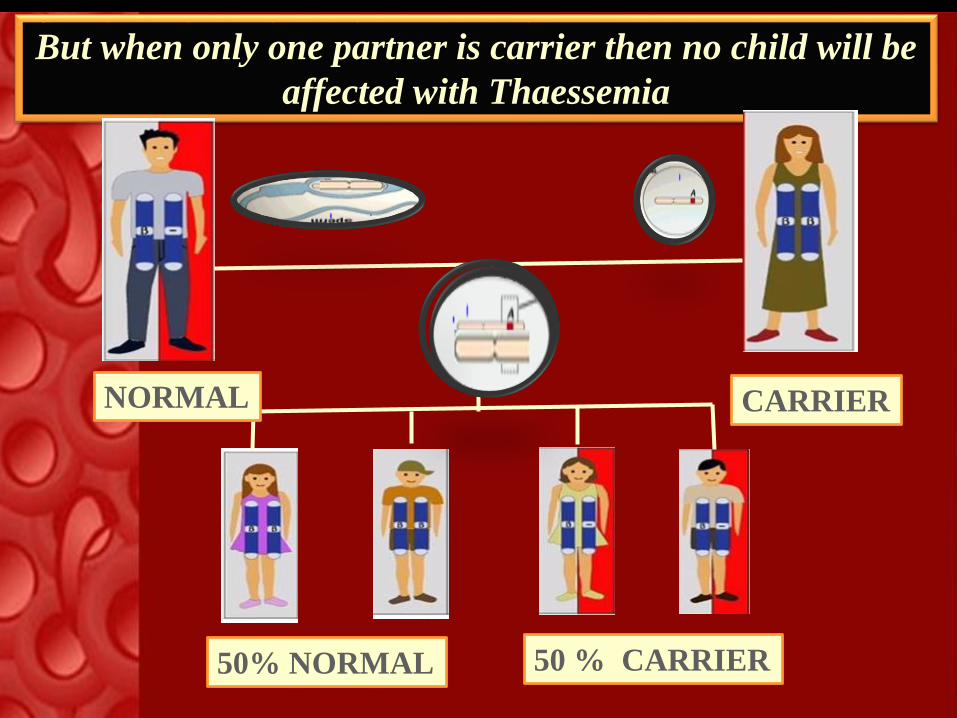
But when only one partner is carrier then no child will be
affected with Thaessemia
CARRIER
50 % CARRIER
NORMAL
50% NORMAL

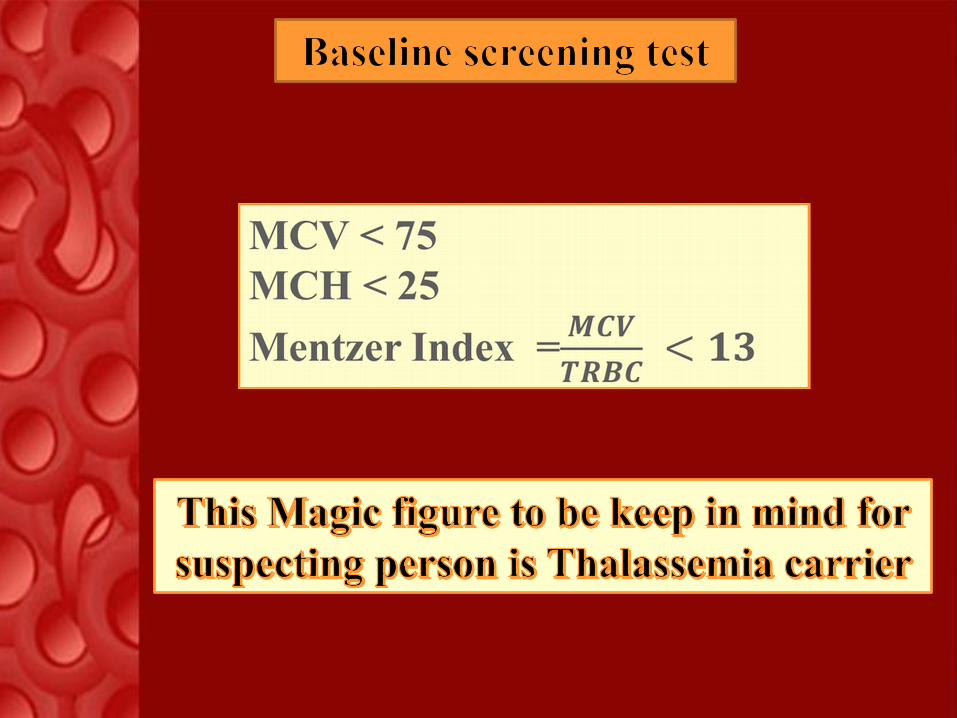
-Carriers are Asymptomatic
-They are silent culprit
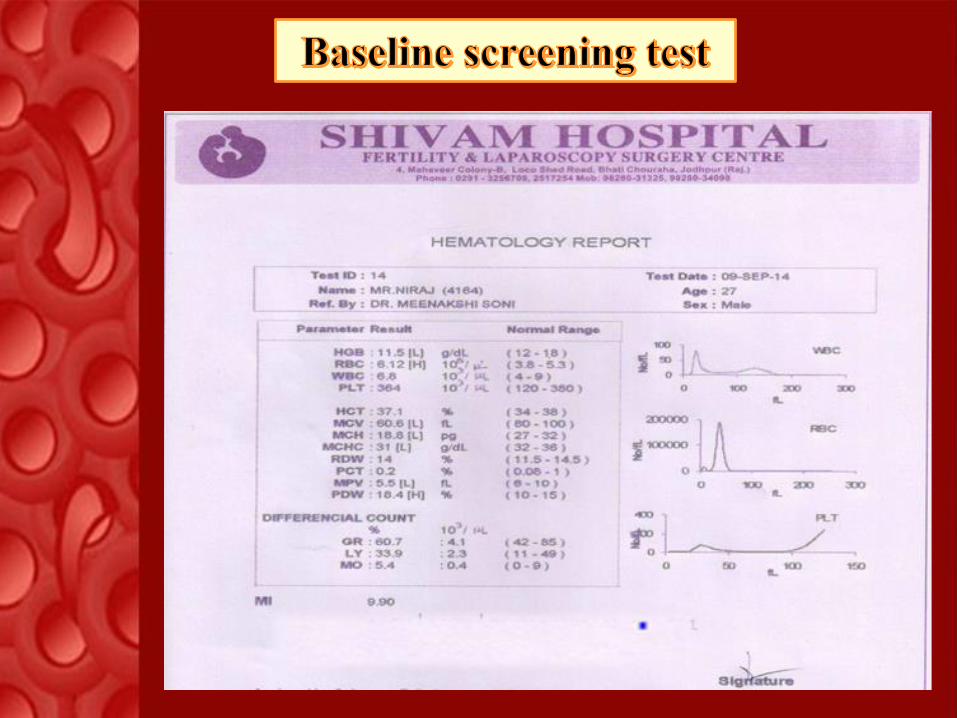
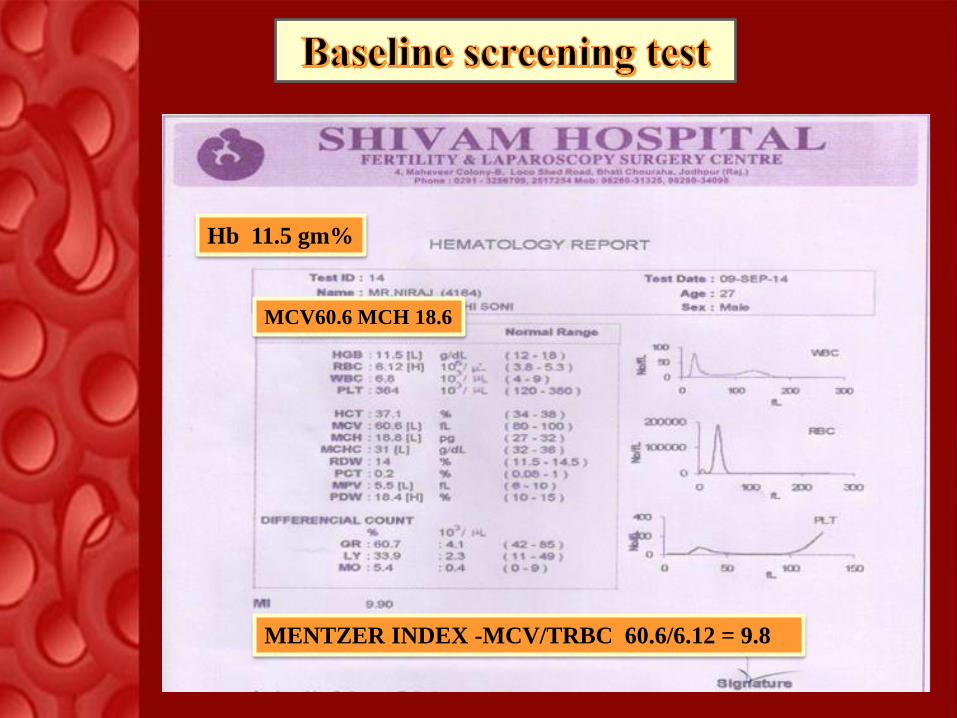
Hb 11.5 gm%
MCV60.6 MCH 18.6
MENTZER INDEX -MCV/TRBC 60.6/6.12 = 9.8

Genetic Counseling
If marriage is unavoidable due to cultural
& social reasons or diagnosed as carriers after
marriage or after conception
P
Then what is the option ?
PRENATAL DIAGNOSIS
G1P0A0
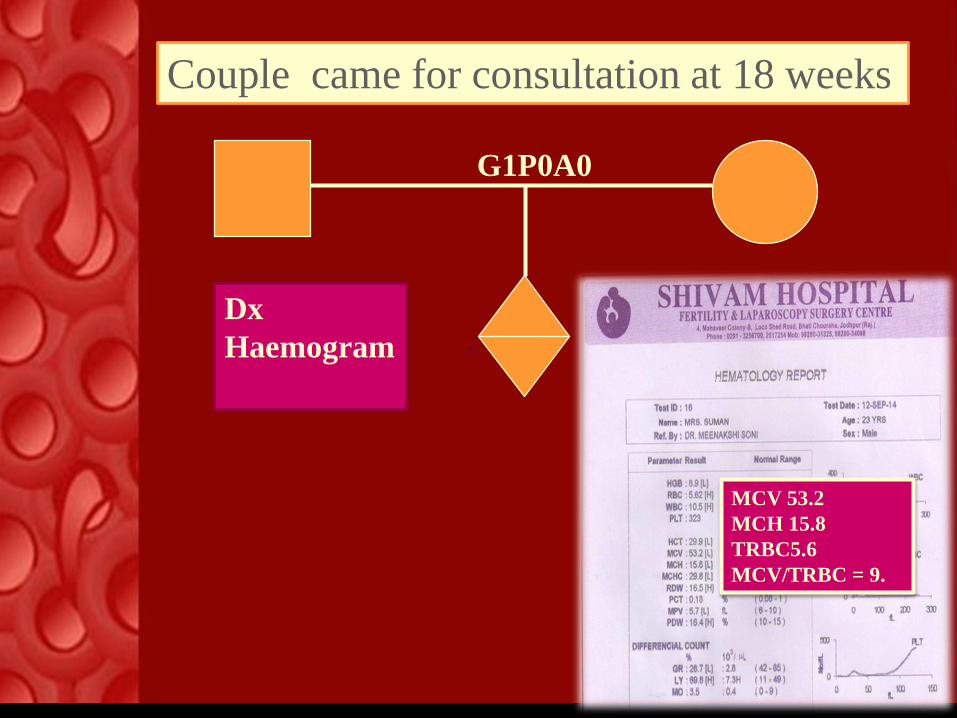
Dx
Haemogram
MCV 53.2
MCH 15.8
TRBC5.6
MCV/TRBC = 9.
Couple came for consultation at 18 weeks
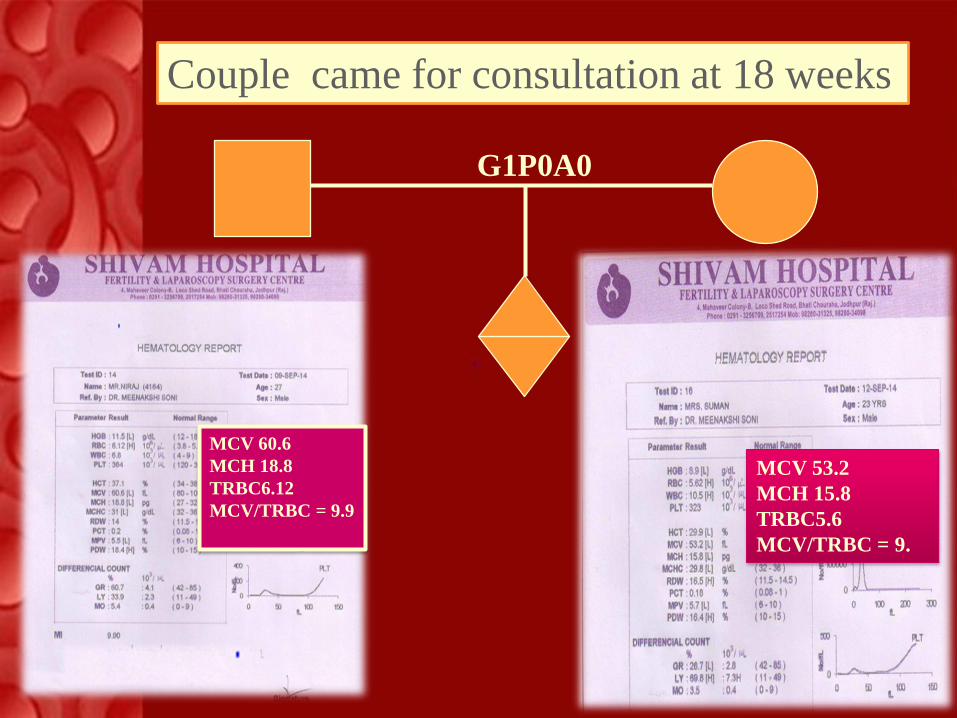
G1P0A0
MCV 60.6
MCH 18.8
TRBC6.12
MCV/TRBC = 9.9
MCV 53.2
MCH 15.8
TRBC5.6
MCV/TRBC = 9.
Couple came for consultation at 18 weeks
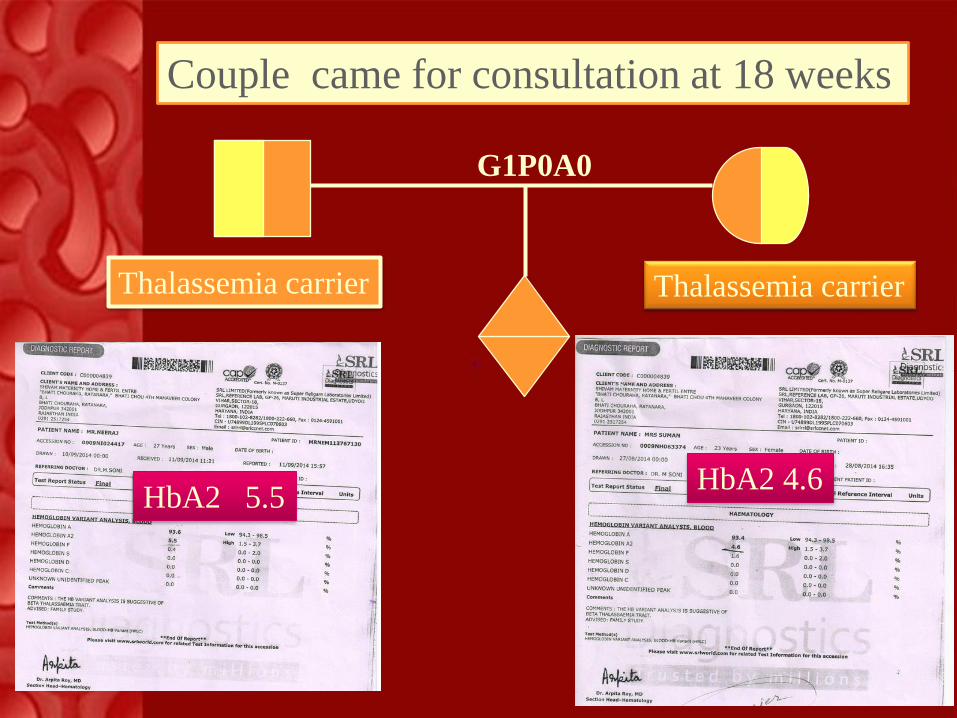
G1P0A0
Thalassemia carrier
HbA2 4.6HbA2 5.5
Couple came for consultation at 18 weeks
Thalassemia carrier
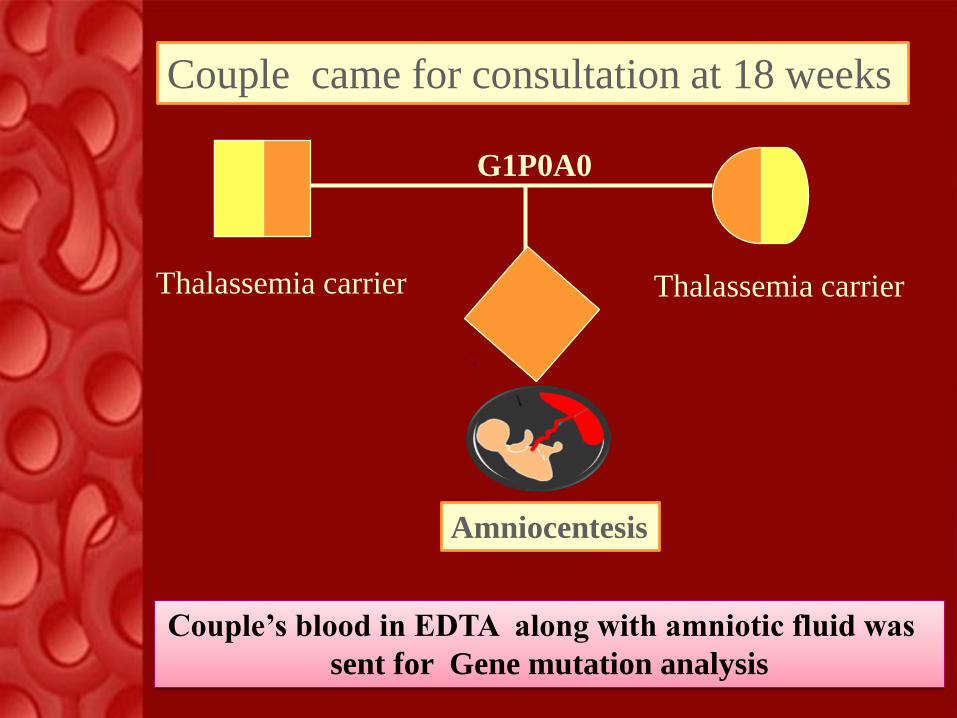
G1P0A0
Thalassemia carrier
Couple came for consultation at 18 weeks
Thalassemia carrier
Amniocentesis
Couple’s blood in EDTA along with amniotic fluid was
sent for Gene mutation analysis
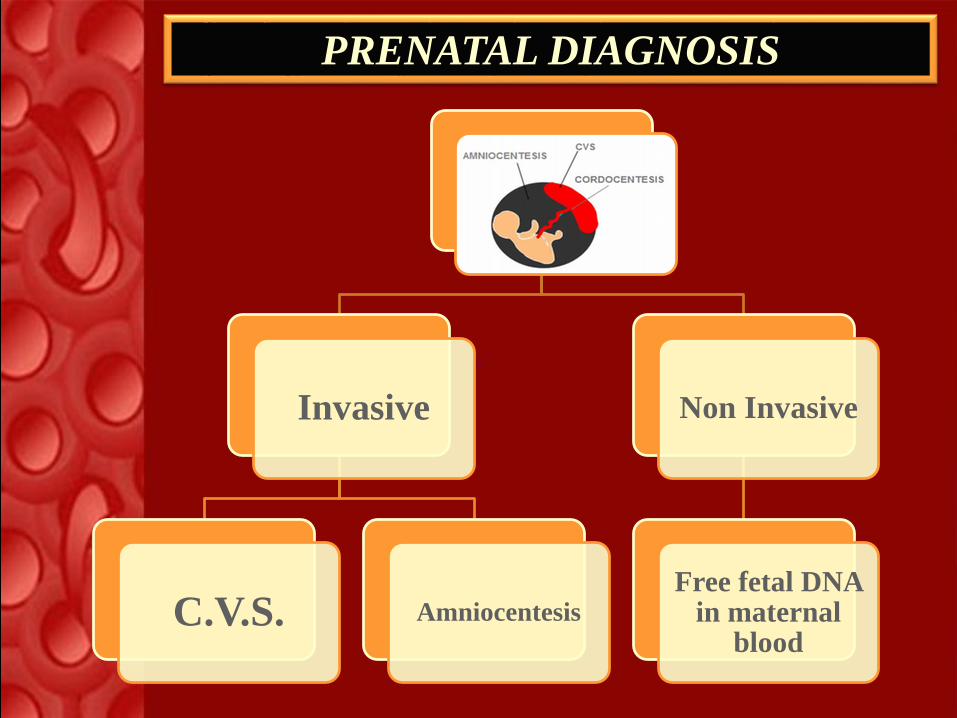
Invasive
C.V.S. Amniocentesis
Non Invasive
Free fetal DNA in maternal
blood
PRENATAL DIAGNOSIS
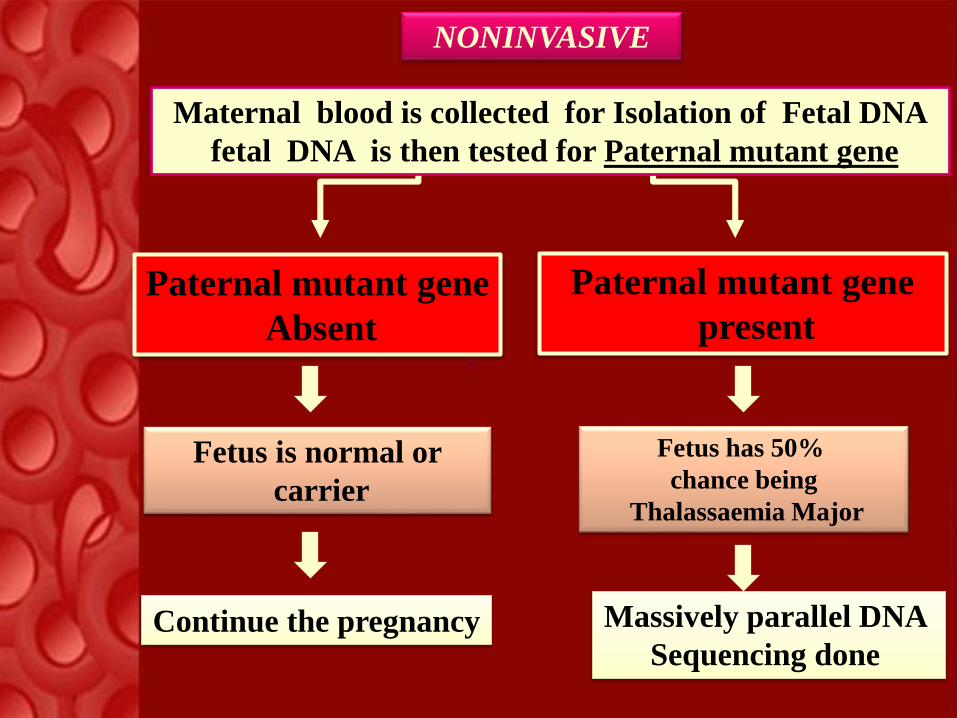
Paternal mutant gene
Absent
Fetus is normal or
carrier
Continue the pregnancy
Paternal mutant gene
present
Fetus has 50%
chance being
Thalassaemia Major
Massively parallel DNA
Sequencing done
Maternal blood is collected for Isolation of Fetal DNA
fetal DNA is then tested for Paternal mutant gene
NONINVASIVE
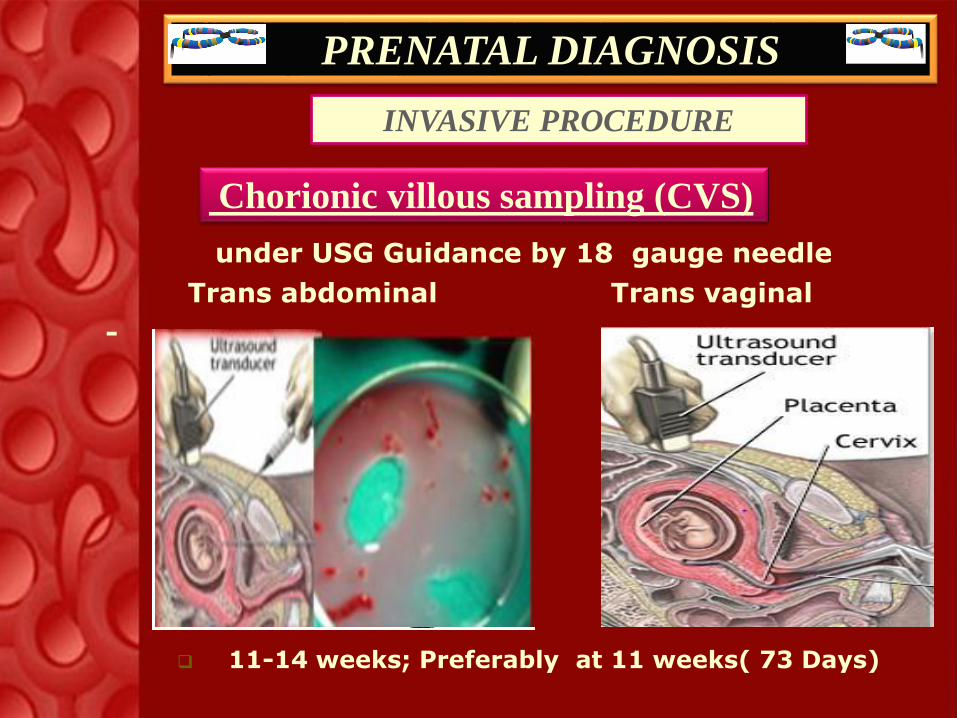
PRENATAL DIAGNOSIS
INVASIVE PROCEDURE
under USG Guidance by 18 gauge needle
Trans abdominal Trans vaginal
-
Chorionic villous sampling (CVS)
11-14 weeks; Preferably at 11 weeks( 73 Days)

PRENATAL DIAGNOSIS
Trans abdominal -Ultrasound guided after 16 weeks
22 g needle
Initial - 2-3 ml is discarded
Usually 20cc amniotic fluid
Results – 2 to 3 weeks
AMNIOCENTESIS
INVASIVE PROCEDURE
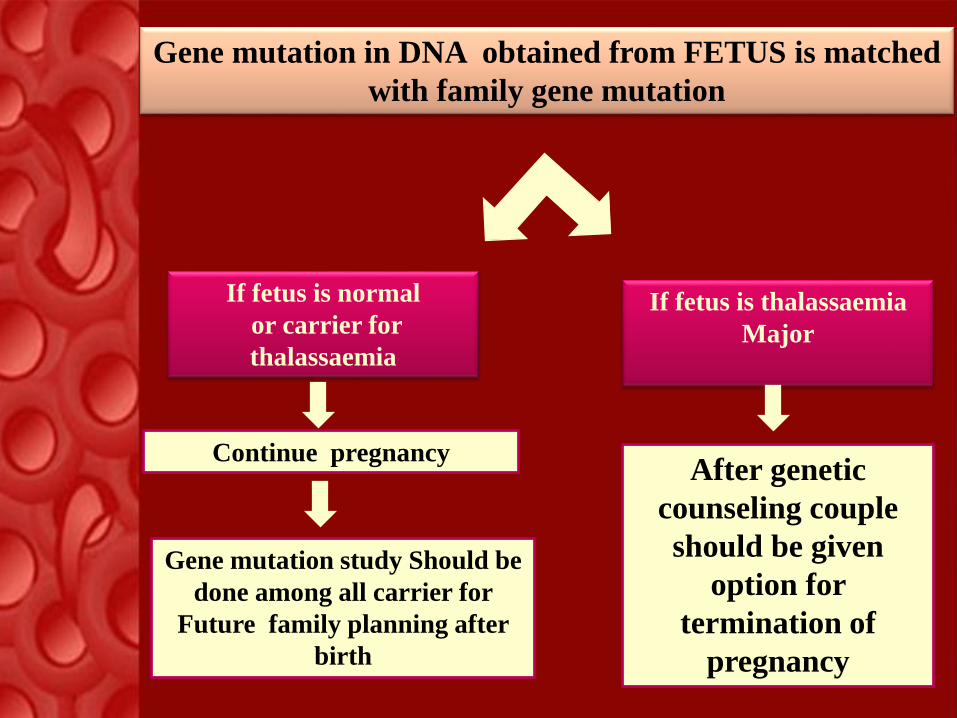
Gene mutation in DNA obtained from FETUS is matched
with family gene mutation
If fetus is normal
or carrier for
thalassaemia
If fetus is thalassaemia
Major
After genetic
counseling couple
should be given
option for
termination of
pregnancy
Continue pregnancy
Gene mutation study Should be
done among all carrier for
Future family planning after
birth
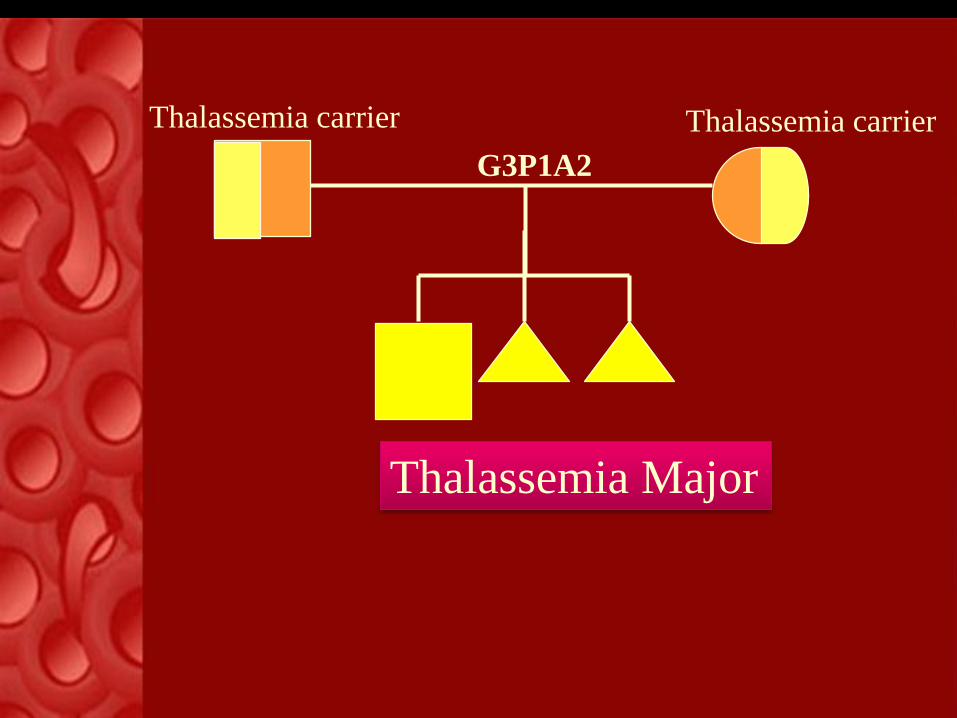
G3P1A2
Thalassemia carrier Thalassemia carrier
Thalassemia Major
Pre-implantation Genetic diagnosis
PGD is a state of the
ART procedure used in
in conjunction with
IVF. In which the
embryo is tested for
Genetic disorders
prior to being placed in
the womb of the
woman -
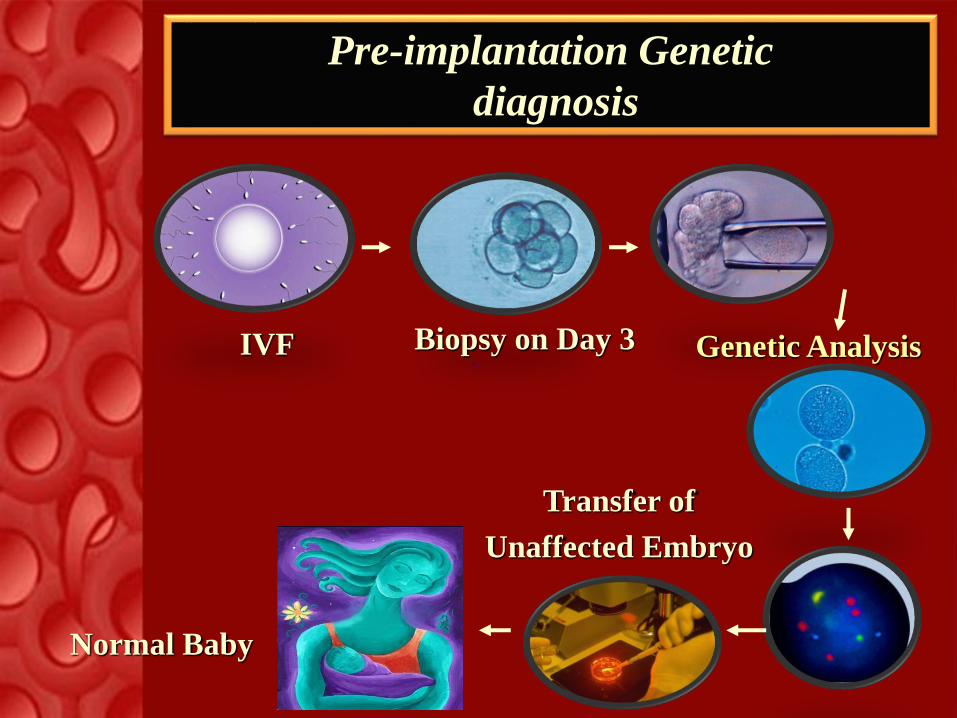
Pre-implantation Genetic
diagnosis
IVF Biopsy on Day 3 Genetic Analysis
Transfer of
Unaffected Embryo
Normal Baby
-
Benefits of Pre-implantation Genetic
diagnosis
For couples who have already an affected
child, PGD allows HLA matching for pre-
selection of potential donor progeny for the
affected sibling who require bone marrow
transplantation.
Psychological stress of termination of
pregnancy can be avoided

World wide 240 million people are
carriers of β-thalassemia i.e.
1.5% of total world population.
Approximately 15 million people are
estimated to suffer from
“Thalassemia Major”.
Every year One lac children are
born with thalassemia major
On an average 1 person in every 25
Indians is a thalassemia carrier i.e.
approximately 30 million people are
thalassaemia carrier .
Every hour “One” Thalassaemia major
child is born i.e. every year
approximately10,000 new Thalassaemia
patients are born in India.
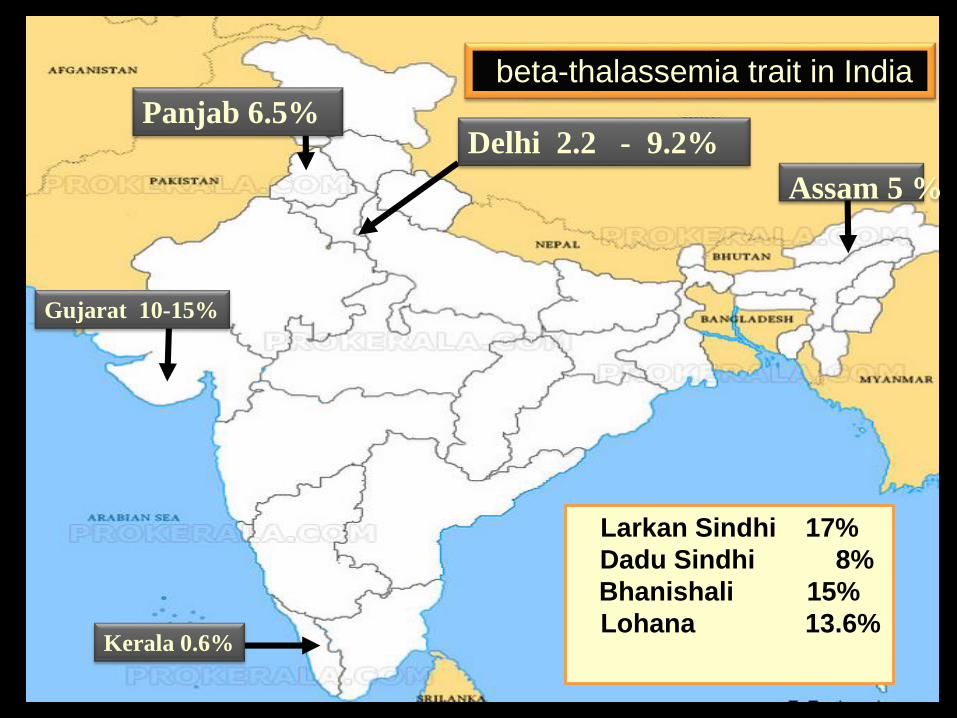
beta-thalassemia trait in India
Panjab 6.5%Delhi 2.2 - 9.2%
Larkan Sindhi 17%
Dadu Sindhi 8%
Bhanishali 15%
Lohana 13.6%Kerala 0.6%
Assam 5 %
Gujarat 10-15%

TO REDUCE
TO PREVENT
TO SET UP
TO DIAGNOSE


Lack of
Education
Lack of
experts
Social factorsLack of
National
policy
lack of
Fetal medicine
Centre Lack Genetic entre
lack of
Funds lack of
Screening

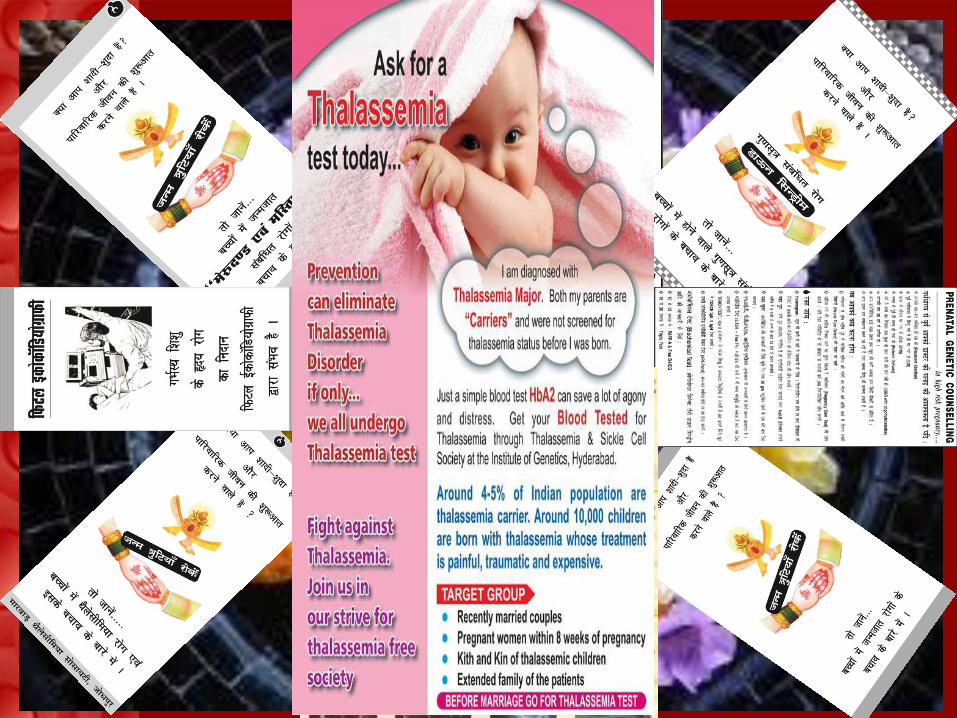
Lack of Education
Illiteracy is a big challenge for prevention of
Thalassaemia In India
Lack of Education lack of Pre marital screening
Detection of Carrier state
seems to be is a “stigma” to
their life and may
Affect their marriages
hence deprived of it.
Lack of Pre- conception counseling –Even When family is having
affected Child, Couple have
unplanned pregnancy due
lack of knowledge & fund for
Screening methods.
Lack of Education
They do not have early
antenatal Booking
Hence deprived of
prenatal screening
And
prenatal diagnostic
care for
Thalassaemia
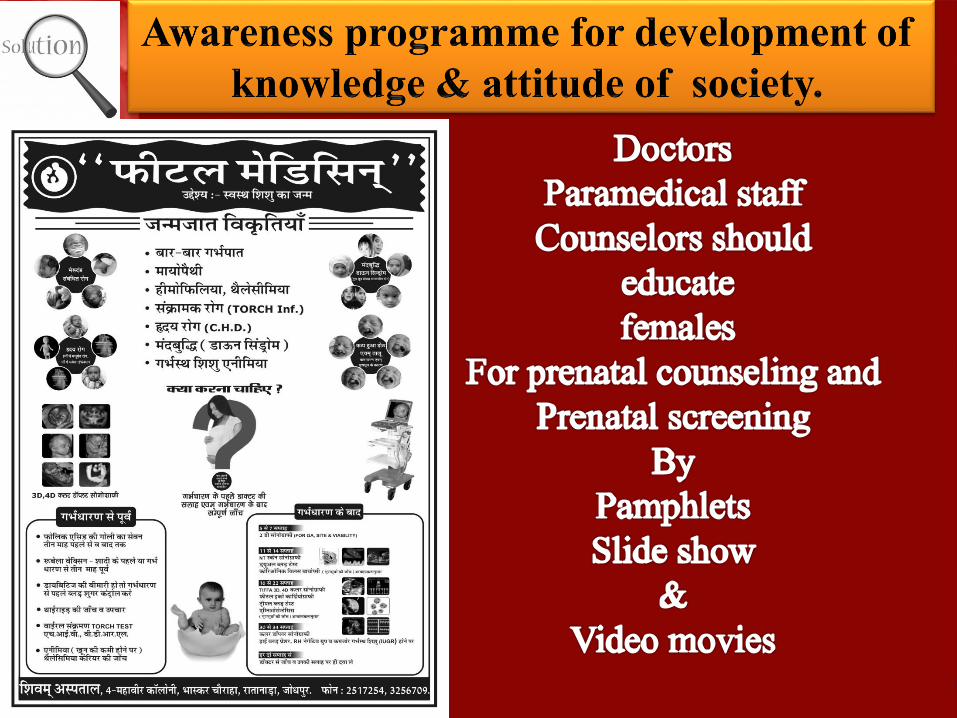
Lack of knowledge &
attitude
Of pregnant woman &
her family

Challenges of Social factors
Consanguineous Marriage
Marriage among Close blood relative is a big hurdle for
prevention of Thalassaemia.
Feticide is “SIN” Hence they avoid termination of
even when fetus is affected.
Lack of well equipped laboratory
Lack of genetic laboratory
Challenges of Economic burden Fund for
Education, Training and awareness
programmes
Fetal medicine Centre 50 -70 lacs
Lab - Cell counter 08-10 lacs
- HPLC 70-80 lacs
Genetic lab 25-75 lacs
Economic burden on patients



Mass screening :
Means screening of each individuals
for thalassemia in reproductive age
group (15 to 45 years)

P
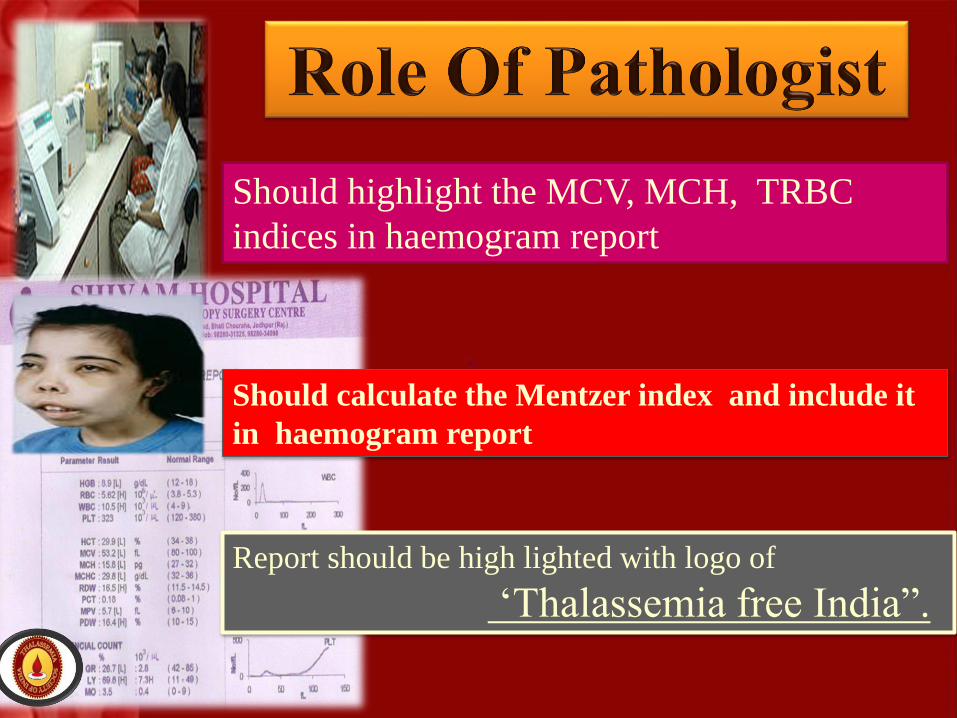
Report should be high lighted with logo of
‘Thalassemia free India”.
Should calculate the Mentzer index and include it
in haemogram report
Should highlight the MCV, MCH, TRBC
indices in haemogram report
3.Casscade screening :
Screening of relatives of index Thalassemia major

Government should formulate a policy for implementation of
universal Thalassaemia screening programme “FREE OF
COST” for infants, school and college going children,
And those attending preconceptional and antenatal clinics.
“Registration of marriage by the court should be done only
when Blood report of Thalassemia screening is produced”
Like “Janani surksha yojana” the government should formulate
the policy Of “ SWASTH SHISHU YOJANA” to prevent the
birth of child with “THALASSEMIA” by providing prenatal
diagnostic facility “FREE OF COST” at each and every corner of
our country.
Psychological and financial support should be given to the
pregnant women for safe termination of pregnancy if the fetus is
affected with Thalassemia major.


Join hands

I AM A SMALL AND PRETTY CREATURE
WILL SOON COME TO THIS WORLD IN FUTURE.
BUT WOULD LIKE TO SEE SMILING DAD AND MOM
WHEN I COME OUT OF THE WOMB
THIS IS POSSIBLE ONLY WHEN
I BORN HEALTHY ONLY THEN
SO I APPEAL TO MY DOCTOR FRIENDS
DO INVESTIGATE ON ME BEOFRE JOURNEY ENDS
START WITH GENETIC COUNSELLING WITH MOM
BEFORE I ARRIVE IN THE WOMB
DO MOM’S HAEMOGRAM BLOOD TEST
TAKE MCV &MCH CRITERIA IN SET
IF MCV LESS THAN 75 & MCH LESS THAN 25 INDICE
THEN GO FOR ESTIMATION OF HbA2 IN PRECISE
IF VALUE COMES TO BE MORE THAN 3.5 PERCENT
LABLE MY MOM AS THALASSAEMIA CARRIER INSTANT
ADVISE FOR MY DAD’S CARRIER SCREEN TEST
IF COMES POSITIVE , GO FOR MY PRENATAL TEST
DO CVS AT 12 WEEKS OF MY GESTATIONAL LIFE
TAKE OUT VILLOUS TISSUE BY SMALL NEEDLE PIPE
SENT CVS TO GENETIC LAB FOR GENE MUTATION ANALYSIS
ALONG WITH REPORT OF MY PARENT’S BLOOD ANALYSIS
IF I STOOD THALASSAEMIA CARRIER OR NORMAL
CONTINUE MY JOURNEY IN THE WOMB AS USUAL
IF MY REPORT SHOW MUTATION FOR THALASSAEMIA DISORDER
TAKE ME OUT OF WOMB TO PREVENT THIS GENETIC DISOREDR
THIS WILL BE VERY PAINFUL TO MY MOM & DAD
FOR ME ALSO, NOT TO GET ENTERY IN THIS WORLD
HENCE I APPEAL TO YOU ALL MY DEAR
GO FOR PREMARITAL SCREENING WITHOUT FEAR
SO THAT MY LIFE NEVER COMES IN DANGER ZONE
AND I COMLPETE MY JOURNEY HAPPILY IN THE WOMB
I WOULD LIKE TO SEE ALL PARENTS WITH HAPPY & SMILLING FACE
AND MY NATION WILL SHINE AS THALASSAEMIA FREE IN WORLD RACE
.


“INVITATION”13TH BIENNIAL CONFERENCE OF
“ISPAT”
JODHPUR
SUN CITY OF INDIA
13TH BIENNIAL CONFERENCE OF
“ISPAT”
JODHPUR
SUN CITY OF INDIA
“INVITATION”