Embed Size (px)
Citation preview

Dr W J Rennie MSc,FRCR
Musculoskeletal Radiologist
Honorary Senior Lecturer
Leicester Royal Infirmary
The role of Cement
Augmentation in the
Prevention of Spinal
Insufficiency Fractures
–Albert Einstein
“Not all questions that can be answered are
worth asking and not all questions that are
worth asking can be answered
Acknowledge
Dr B Georgy- San Diego
Prof P Munk- Vancouver
Mr A Qureshi- PhD Orthopaedics
Dr R Botchu Msk Rad
Layout
• Thoughts
• Current Literature
• Review Spinal Biomechanics- Fracture
• My Experience
• Cases
• Summary
Surgical Procedures with No treatment
Effect Vs Conservative Management
Level 1 Evidence
• Scaphoid waist fracture fixation
• Surgical repair - Achilles Tendon ruptures
• Major limb Fracture fixation
Literature
Search
NEJM
Prevention
Insufficiency Fractures
Hip fractures NEJM 1992
Literature Search
• ‘Osteoporosis’, ‘Prophylactic’, ‘cement’, ‘fracture
prevention’
• Recent articles 2009- 2014
• 7 relevant articles Pubmed
• Only 3 on Spine
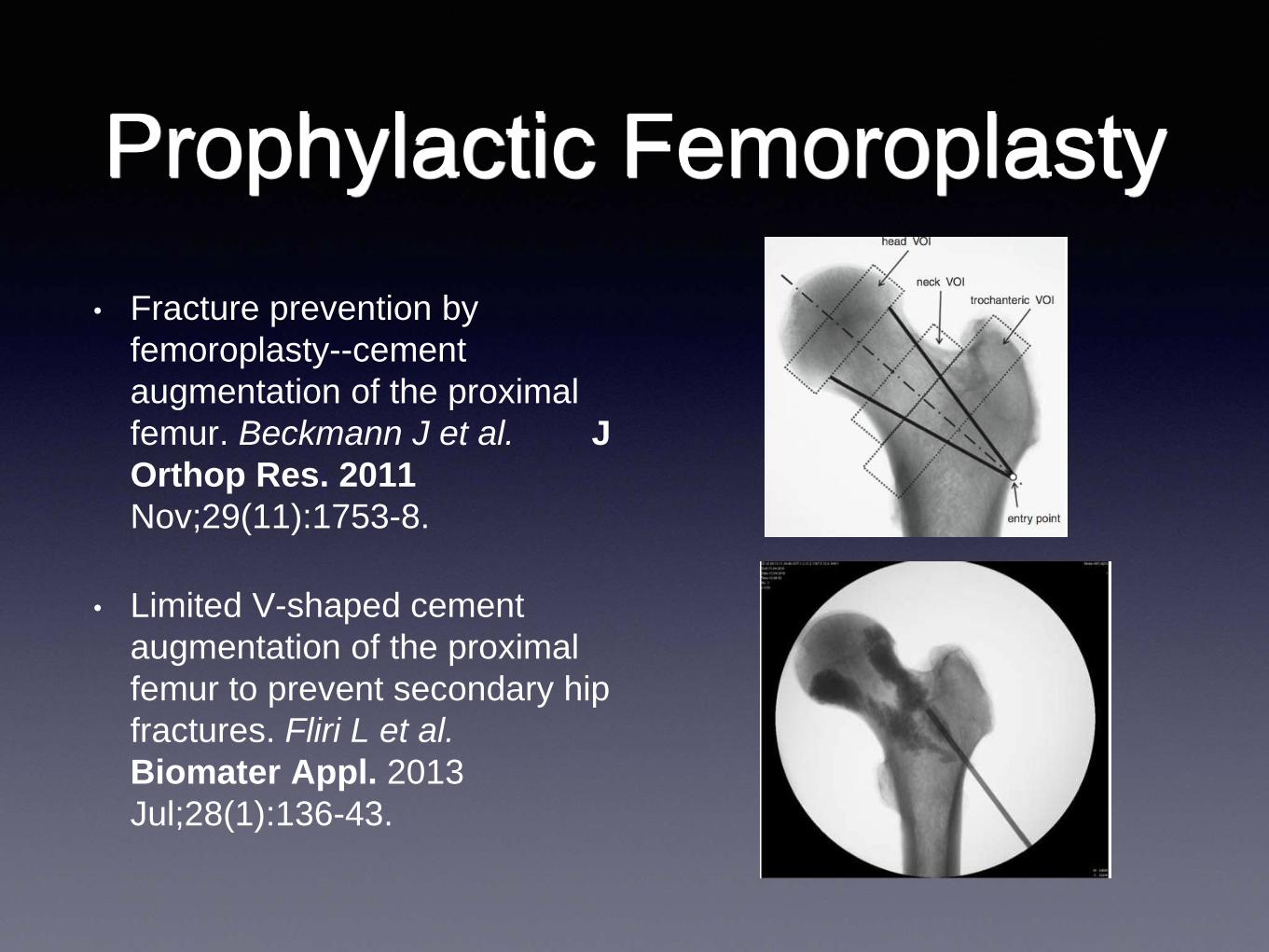
Prophylactic Femoroplasty
• Fracture prevention by
femoroplasty--cement
augmentation of the proximal
femur. Beckmann J et al. J
Orthop Res. 2011
Nov;29(11):1753-8.
• Limited V-shaped cement
augmentation of the proximal
femur to prevent secondary hip
fractures. Fliri L et al.
Biomater Appl. 2013
Jul;28(1):136-43.
Literature Against
• The effect of cement augmentation on the load
transfer in an osteoporotic functional spinal unit: finite-
element analysis.Polikeit A, Nolte LP, Ferguson SJ.
Spine (Phila Pa 1976). 2003 May 15;28(10):991-6.
• Material changes in osteoporotic human cancellous
bone following infiltration with acrylic bone cement for
a vertebral cement augmentation. Baroud G, Nemes
J, Ferguson SJ, Steffen T. Comput Methods
Biomech Biomed Engin. 2003 Apr;6(2):133-9.
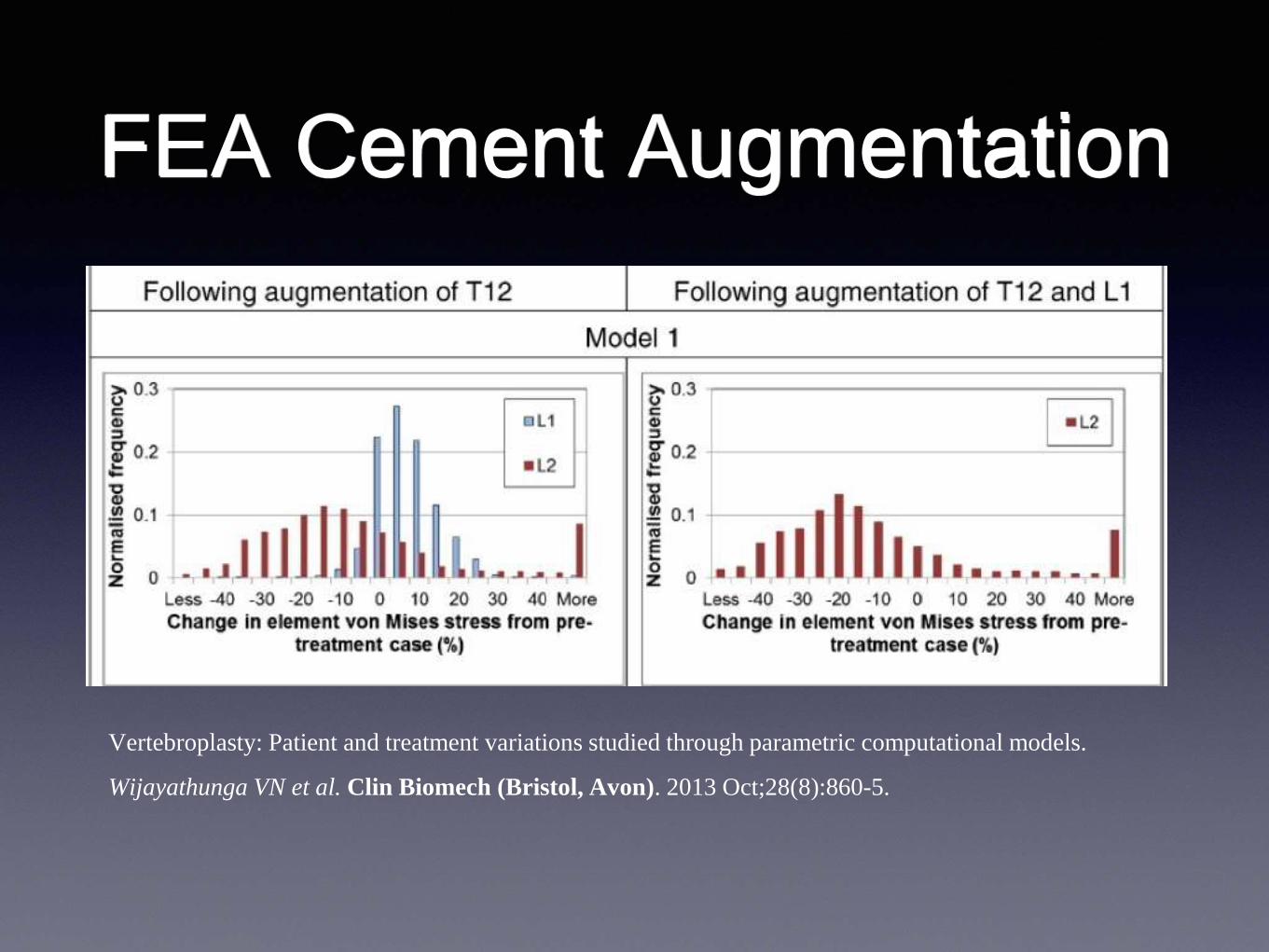
FEA Cement Augmentation
Vertebroplasty: Patient and treatment variations studied through parametric computational models.
Wijayathunga VN et al. Clin Biomech (Bristol, Avon). 2013 Oct;28(8):860-5.
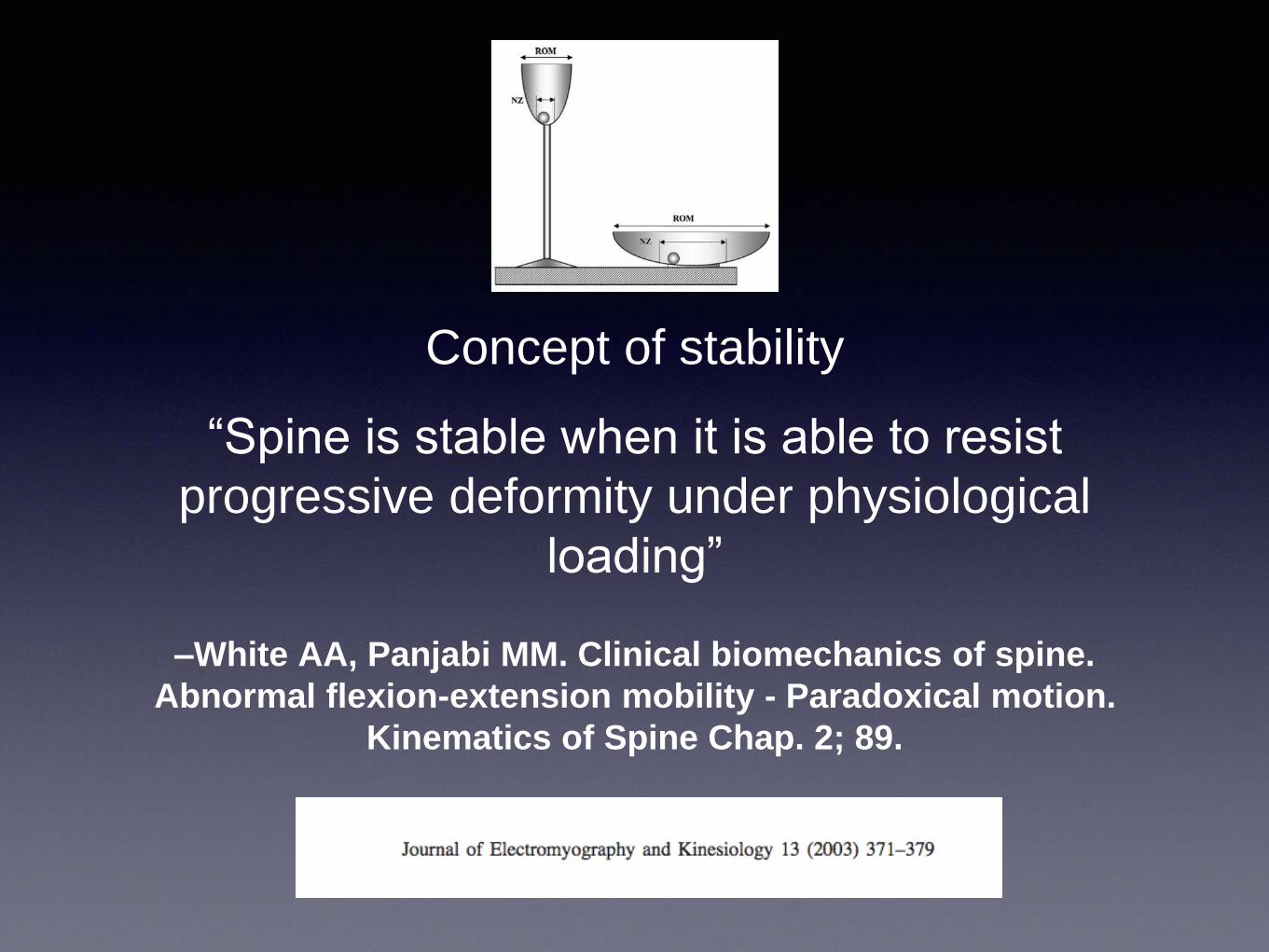
–White AA, Panjabi MM. Clinical biomechanics of spine.
Abnormal flexion-extension mobility - Paradoxical motion.
Kinematics of Spine Chap. 2; 89.
Concept of stability
“Spine is stable when it is able to resist
progressive deformity under physiological
loading”
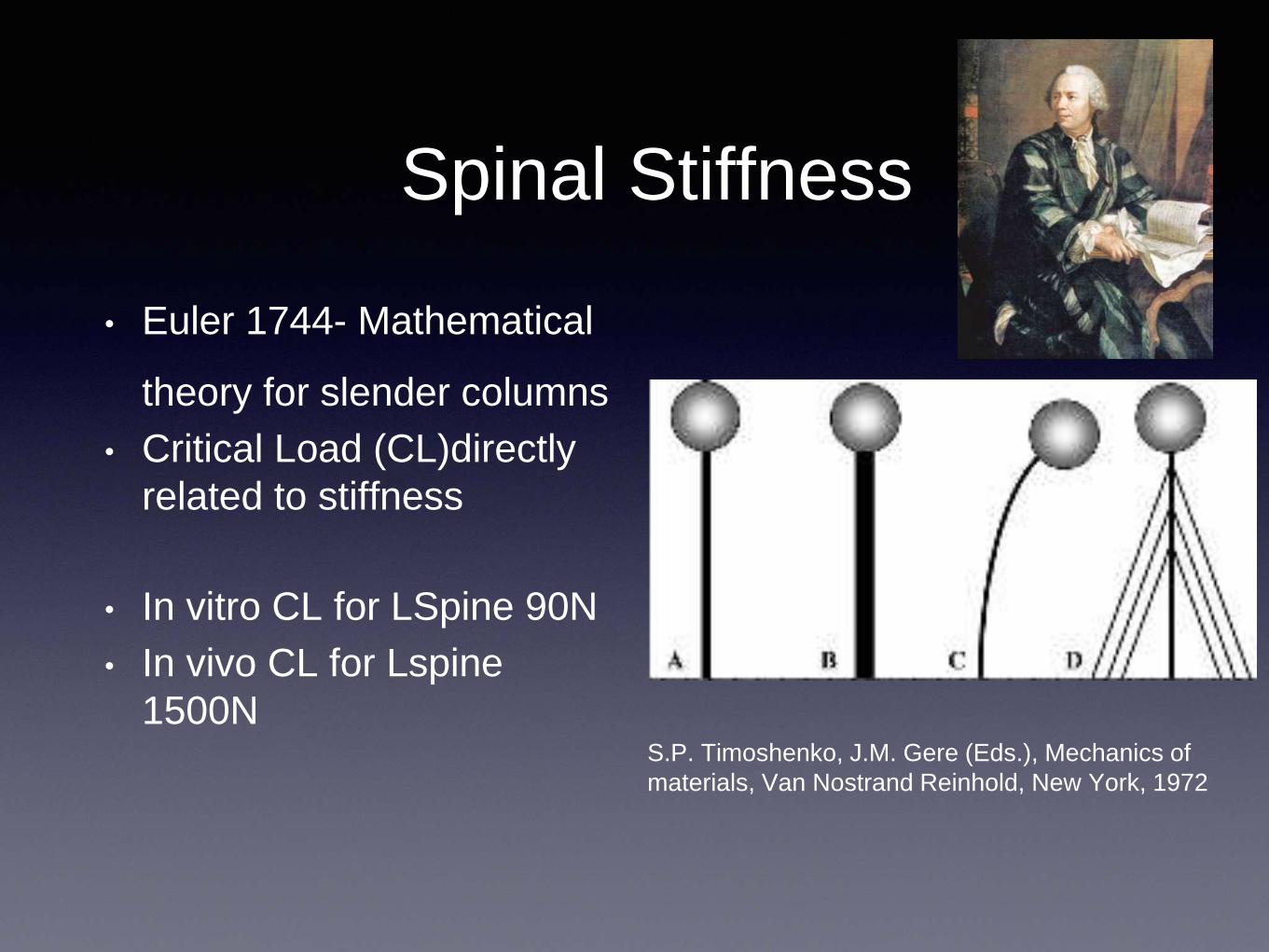
Spinal Stiffness
• Euler 1744- Mathematical
theory for slender columns
• Critical Load (CL)directly
related to stiffness
• In vitro CL for LSpine 90N
• In vivo CL for Lspine
1500NS.P. Timoshenko, J.M. Gere (Eds.), Mechanics of
materials, Van Nostrand Reinhold, New York, 1972
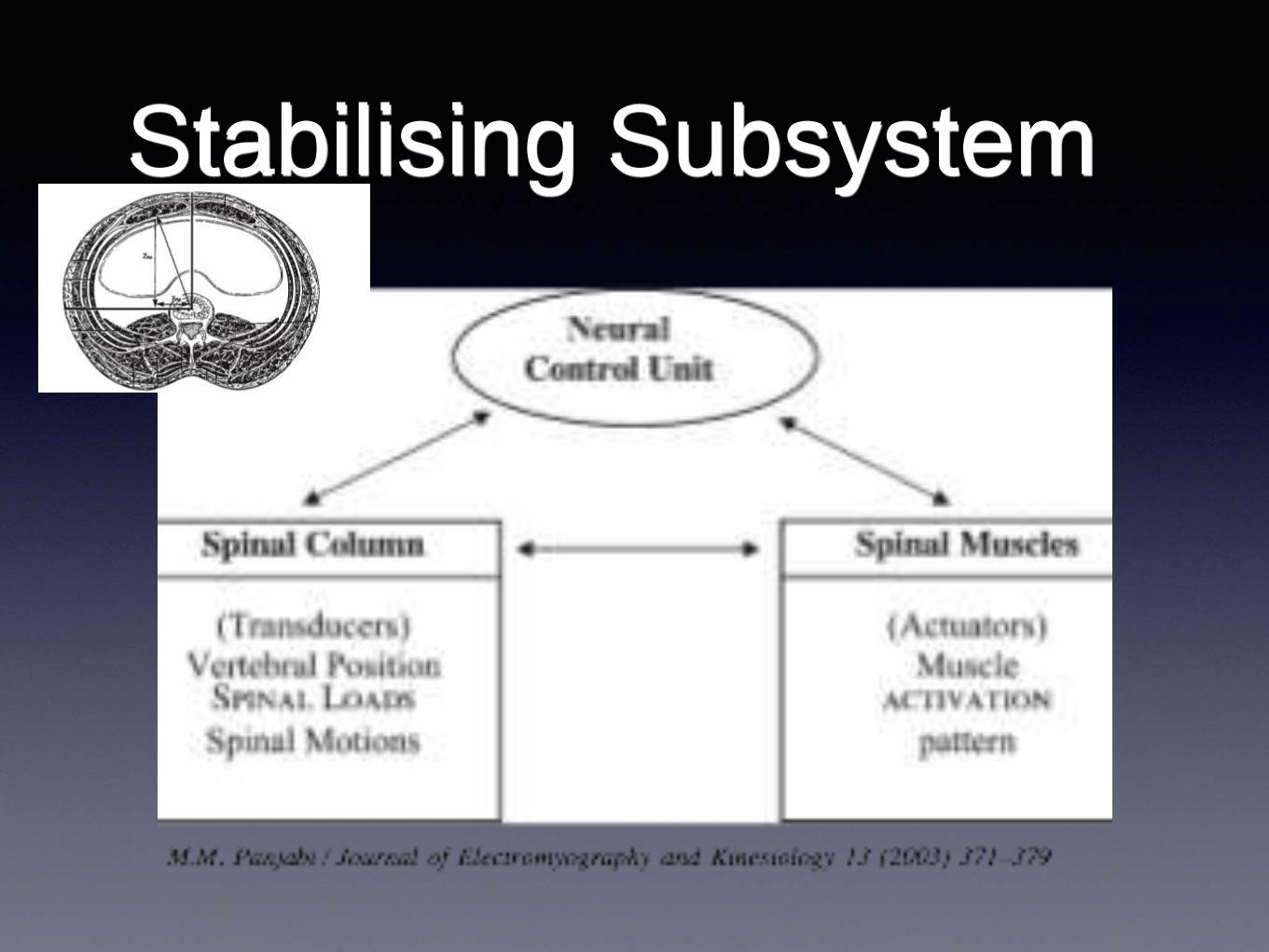
Stabilising Subsystem
Insufficiency Fracture?
• Fracture -Break in the cortex
• Multidirectional
• Significant Force- Trauma
• Single event
• Insufficiency Spine- Failure of
Bone
• Compression
• Gravity- Atraumatic
• Cannot be attributed to a single
event
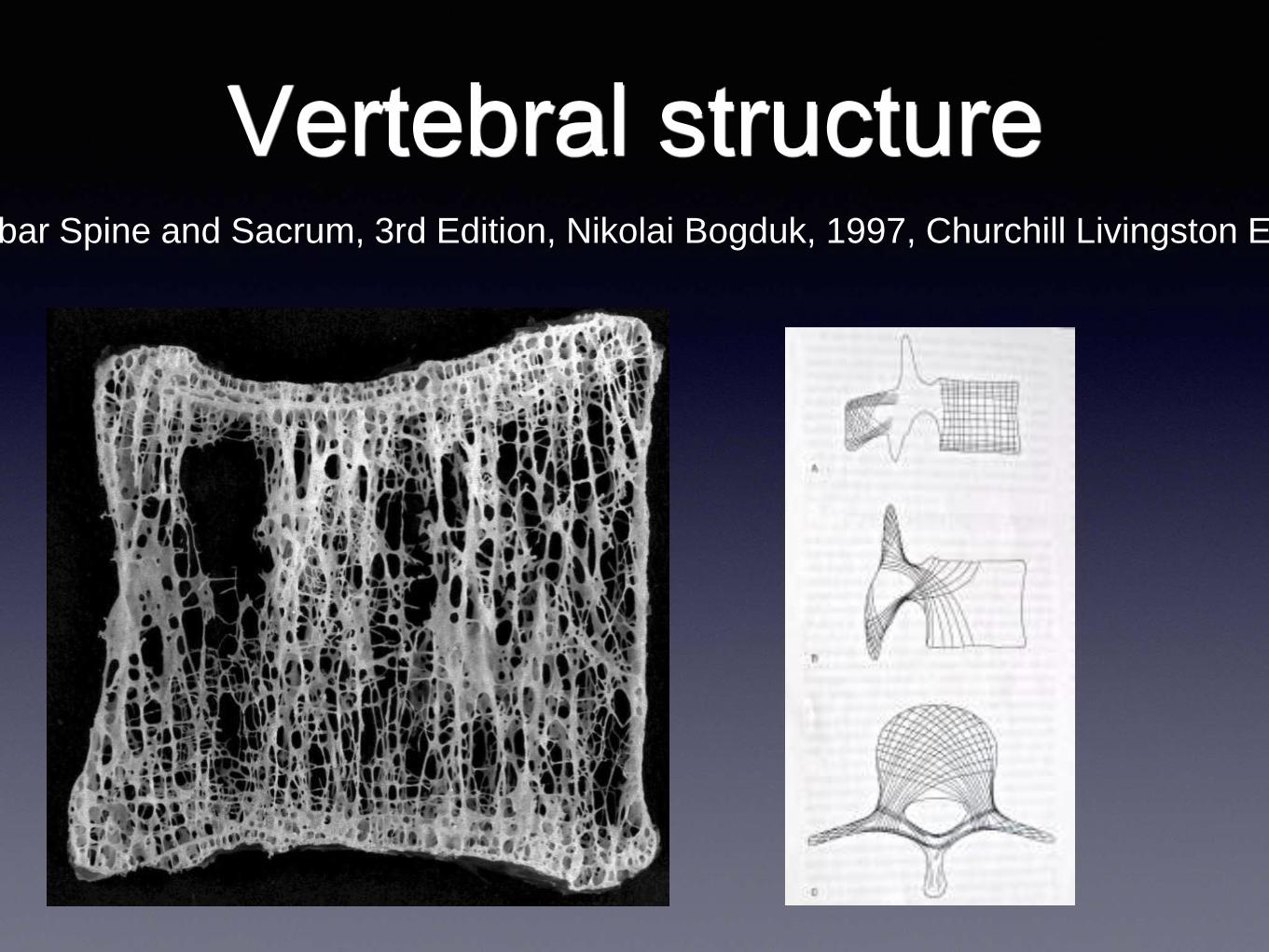
Vertebral structureClinical Anatomy of the Lumbar Spine and Sacrum, 3rd Edition, Nikolai Bogduk, 1997, Churchill Livingston Elsevier, ISBN 0 443
18
Vertebral
cortex/trabecular ratio
A P
Stable Arch
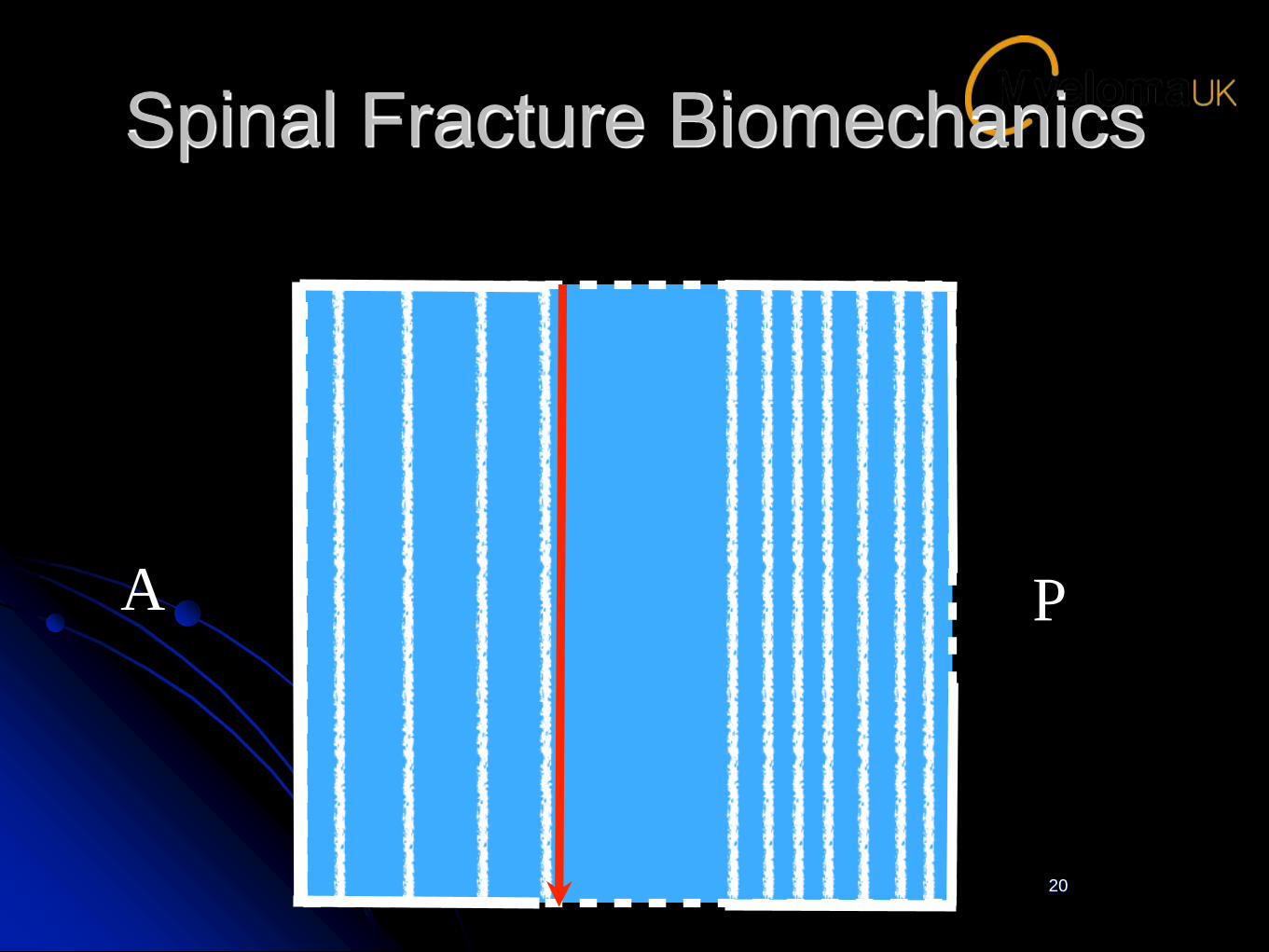
Spinal Fracture Biomechanics
20
A P
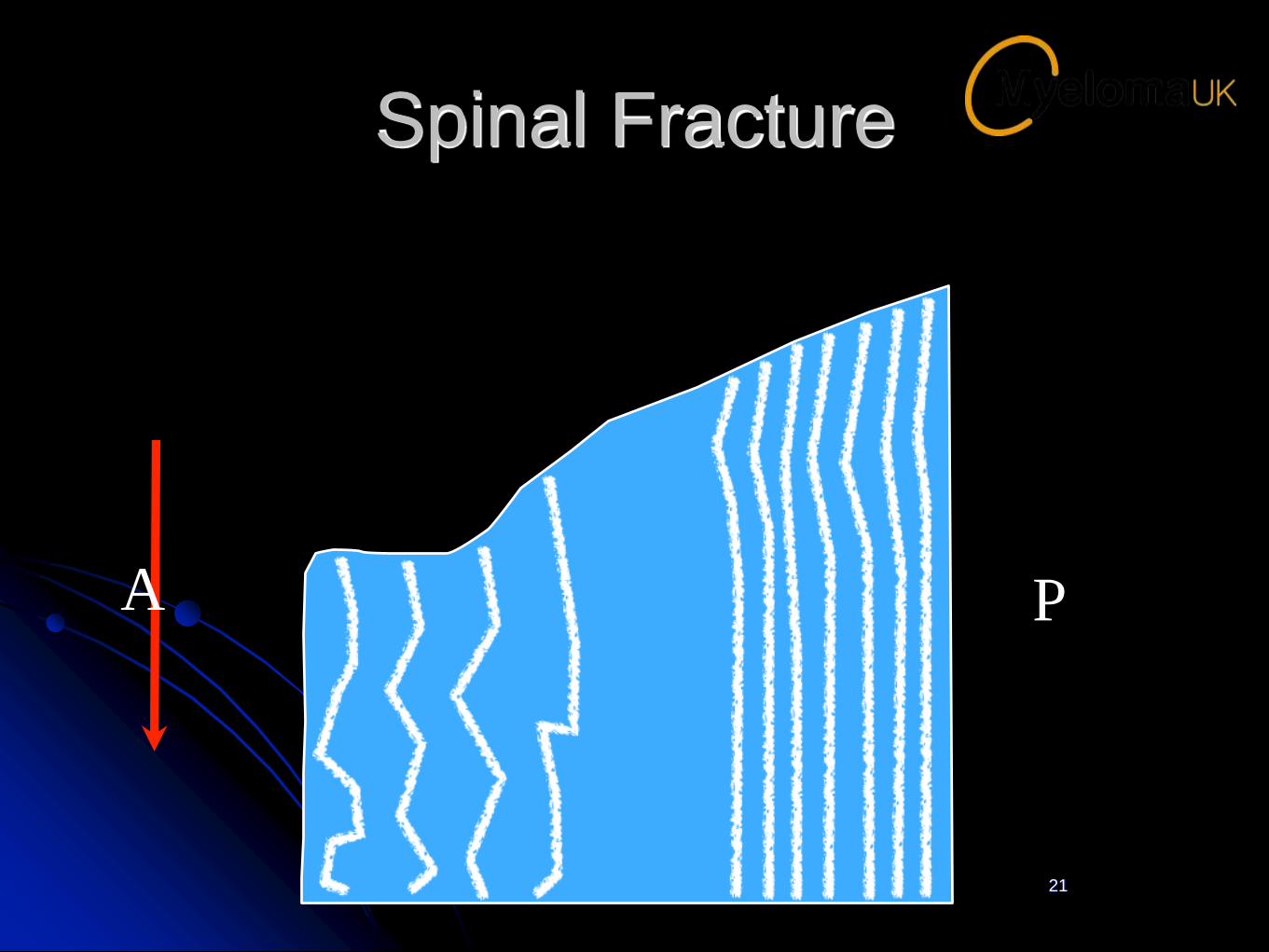
Spinal Fracture
21
PA
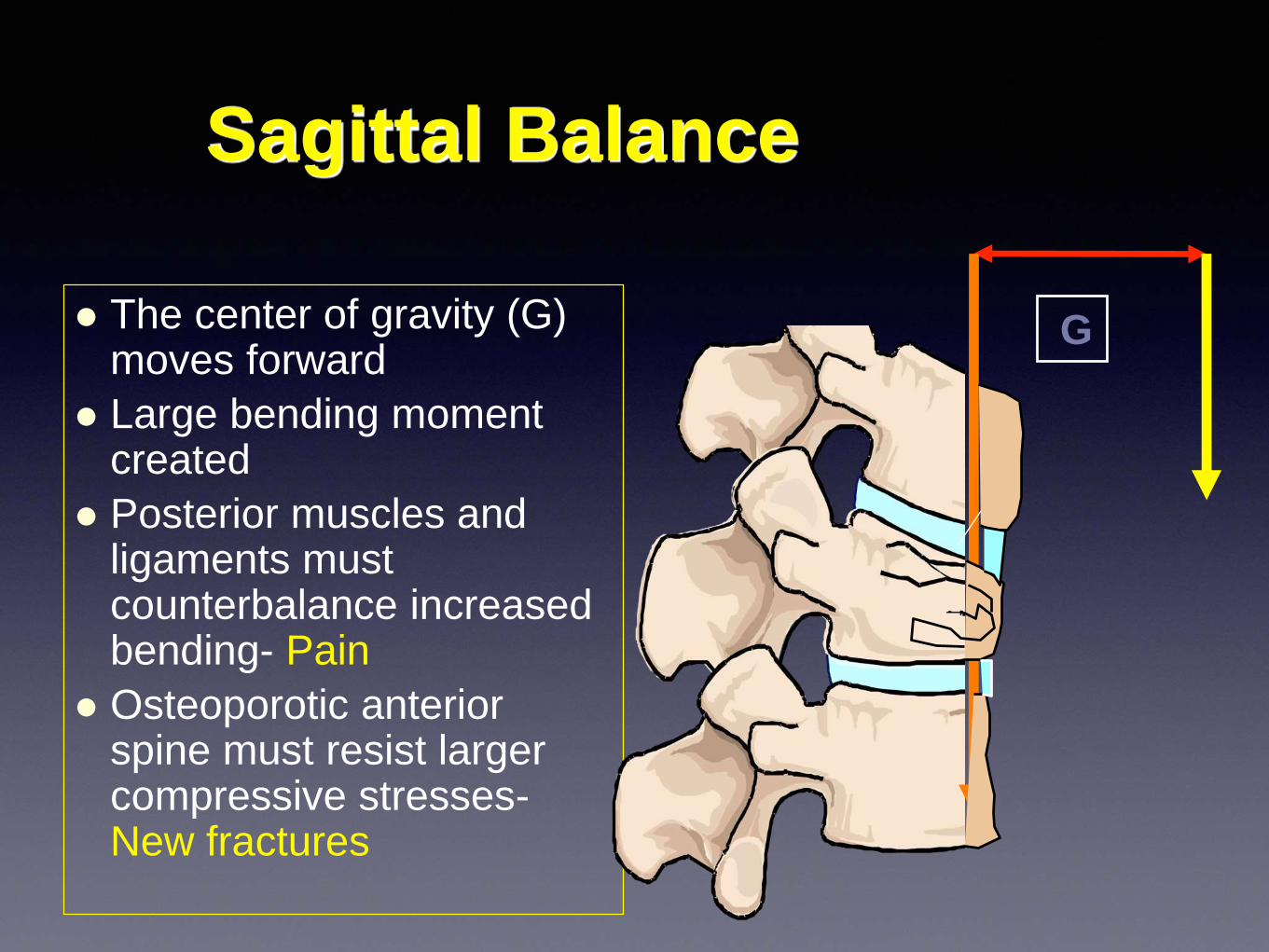
Sagittal Balance
The center of gravity (G) moves forward
Large bending moment created
Posterior muscles and ligaments must counterbalance increased bending- Pain
Osteoporotic anterior spine must resist larger compressive stresses-New fractures
G
Vertebral fracture healing
• Osteoporosis- Delayed bone healing?
• Lack of Callus formation in vertebrae
• Creeping Substitution
• Bone Grafts in spine
• Vertebral clefts- Pseudoarthrosis= Non Union
Hagasewa K et al Spine, 1988;23(20) 2201-06
Giannoudis P et al. Injury, Mar 2007;38(1),S90-99
Literature -1
• Biomechanical effectiveness of prophylactic vertebroplasty
• J Neurosurg Spine 8:442–449, 2008
• 12, 3 segment functional units- T12-L2
• Incremental loads up to 3.5x body weight
• Qct pre and post L1 augmentation
• Fractures occurred only after loads >2-3 times body weight
Literature 2
Prophylactic Vertebroplasty May Reduce the Risk of Adjacent Intact Vertebra From
Fatigue Injury
SPINE Volume 34, Number 4, pp 356 –364
• Biomechanical study on 14, 5 level thoracic spinal segments
• Divided prophylactic & standard groups
• Central vertebra augmented
• Compressive fatigue loading
• Strain Compliance -cortical shell and height
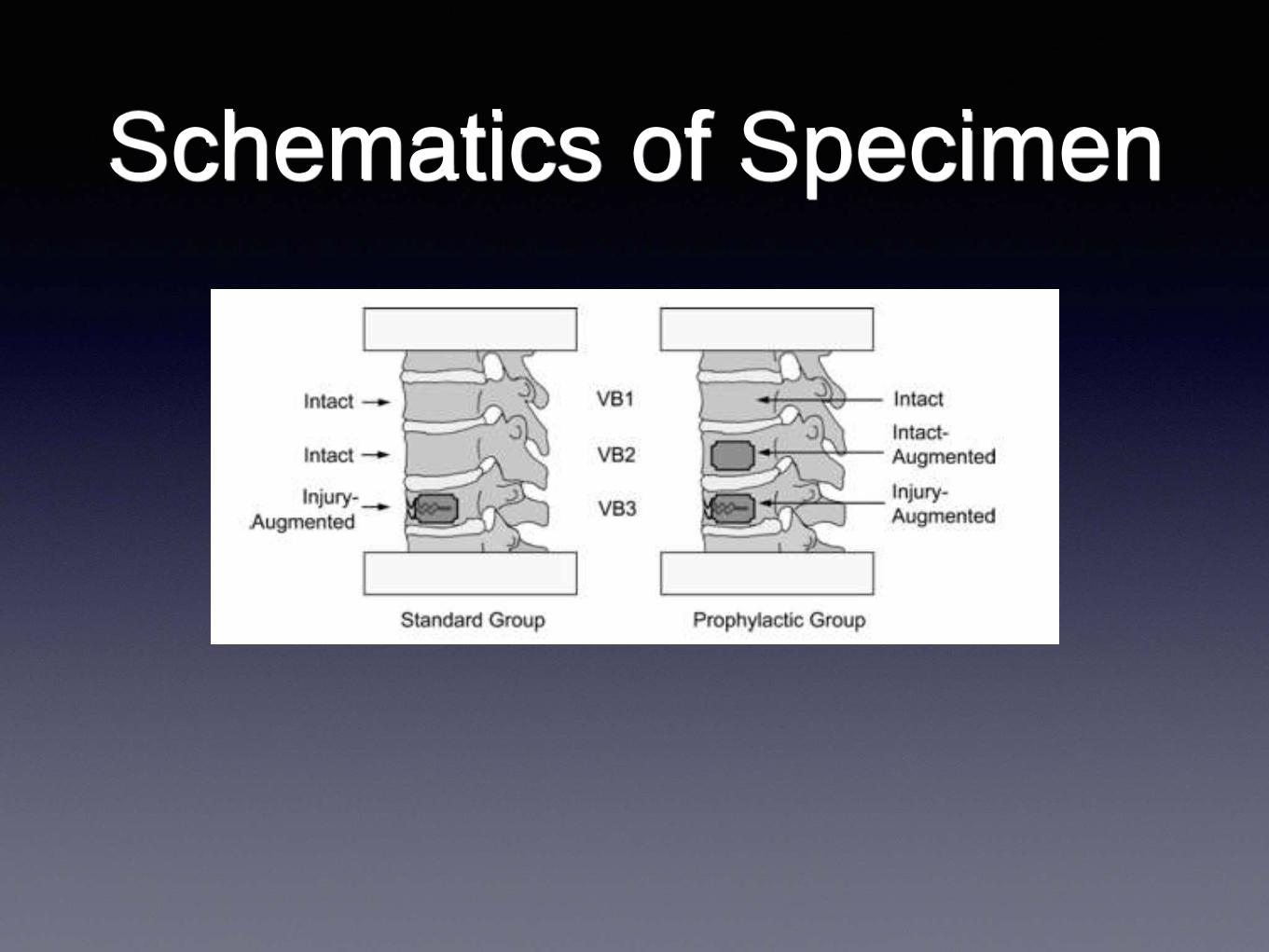
Schematics of Specimen
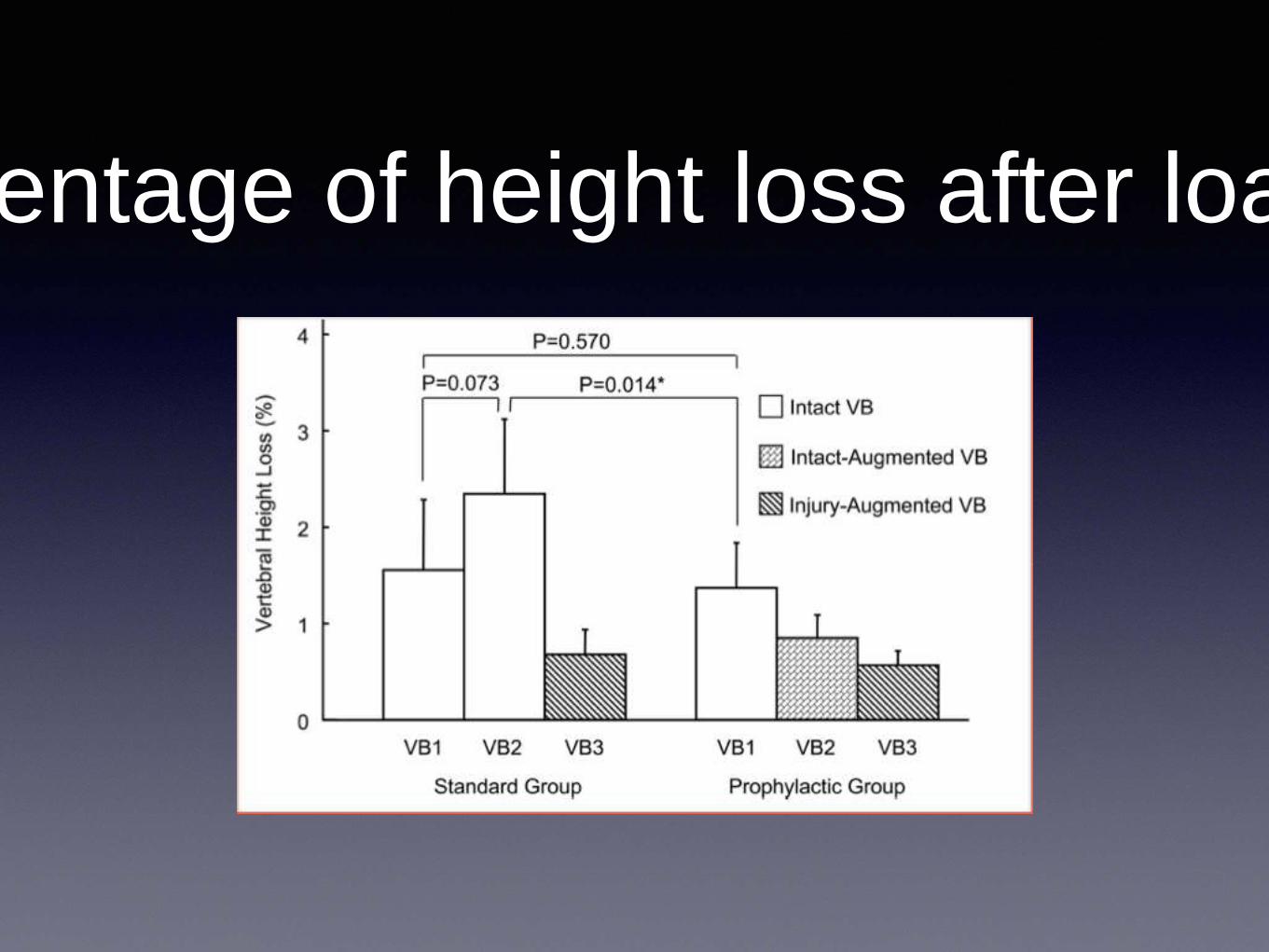
Percentage of height loss after loading
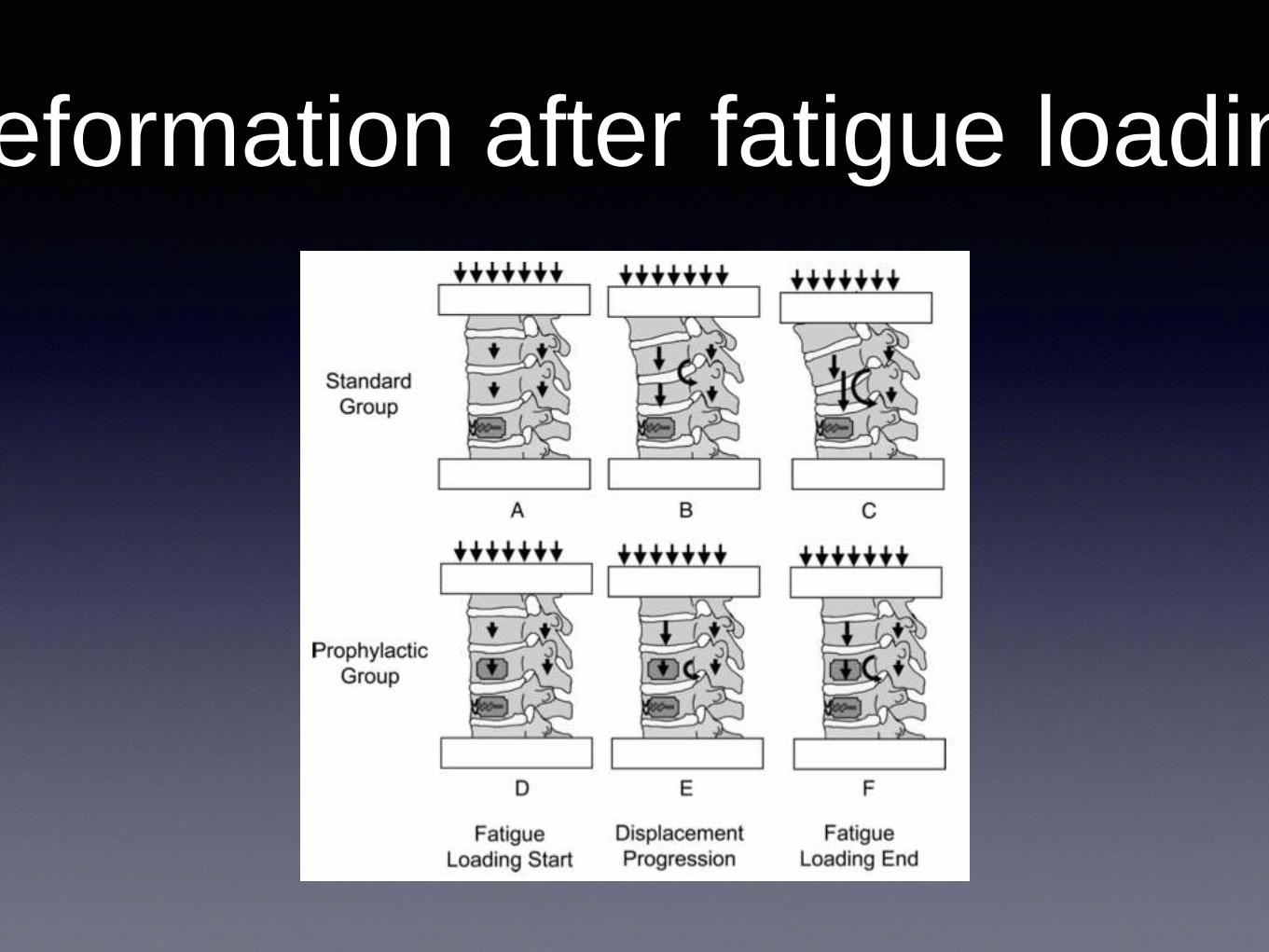
Deformation after fatigue loading
Prophylactic Augmentation
• Prophylactic augmentation strengthens osteoporotic vertebrae,
decreases the progression of vertebral height loss, reduces the
anterior body shift, and hence protects the adjacent intact
vertebra from elevated flexion bending.
• Vertebra is osteoporotic and adjacent level is located at pivot or
lordotic level of spinal column
• Prophylactic augmentation may be an option to prevent the
AVF.
• Spine (Phila Pa 1976). 2009 Feb 15;34(4):356-64.
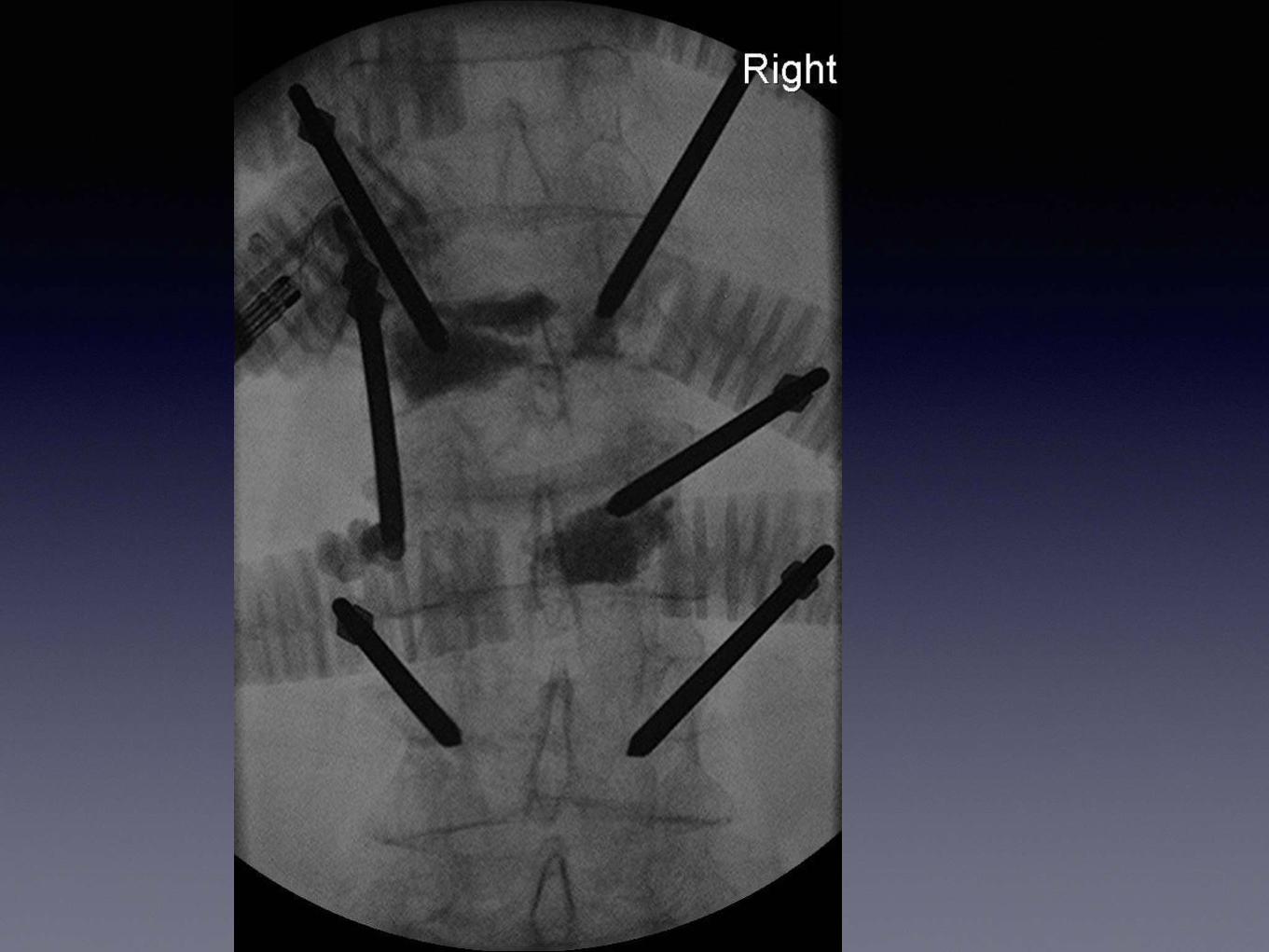
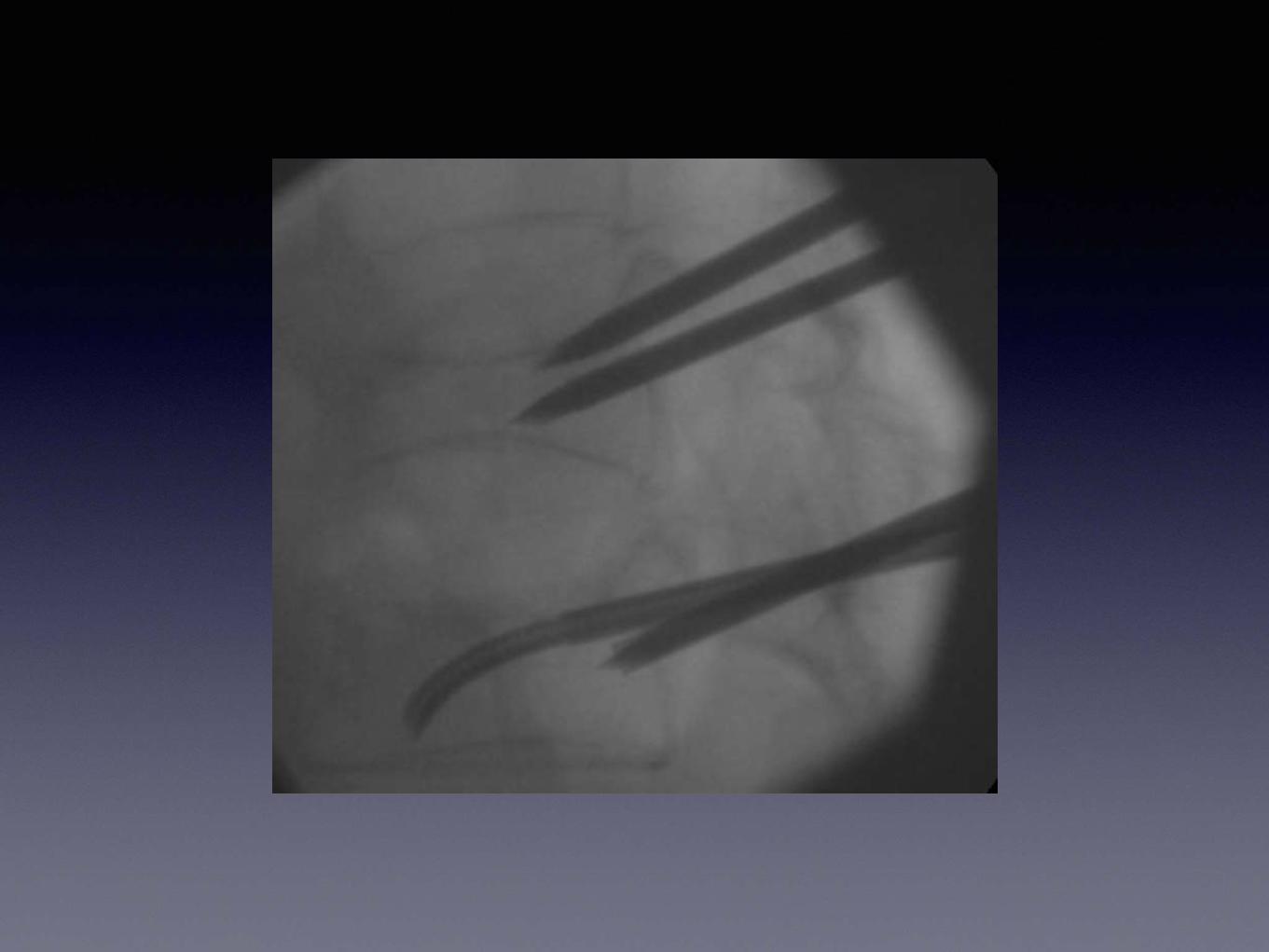
Uni or
Bipedicular?
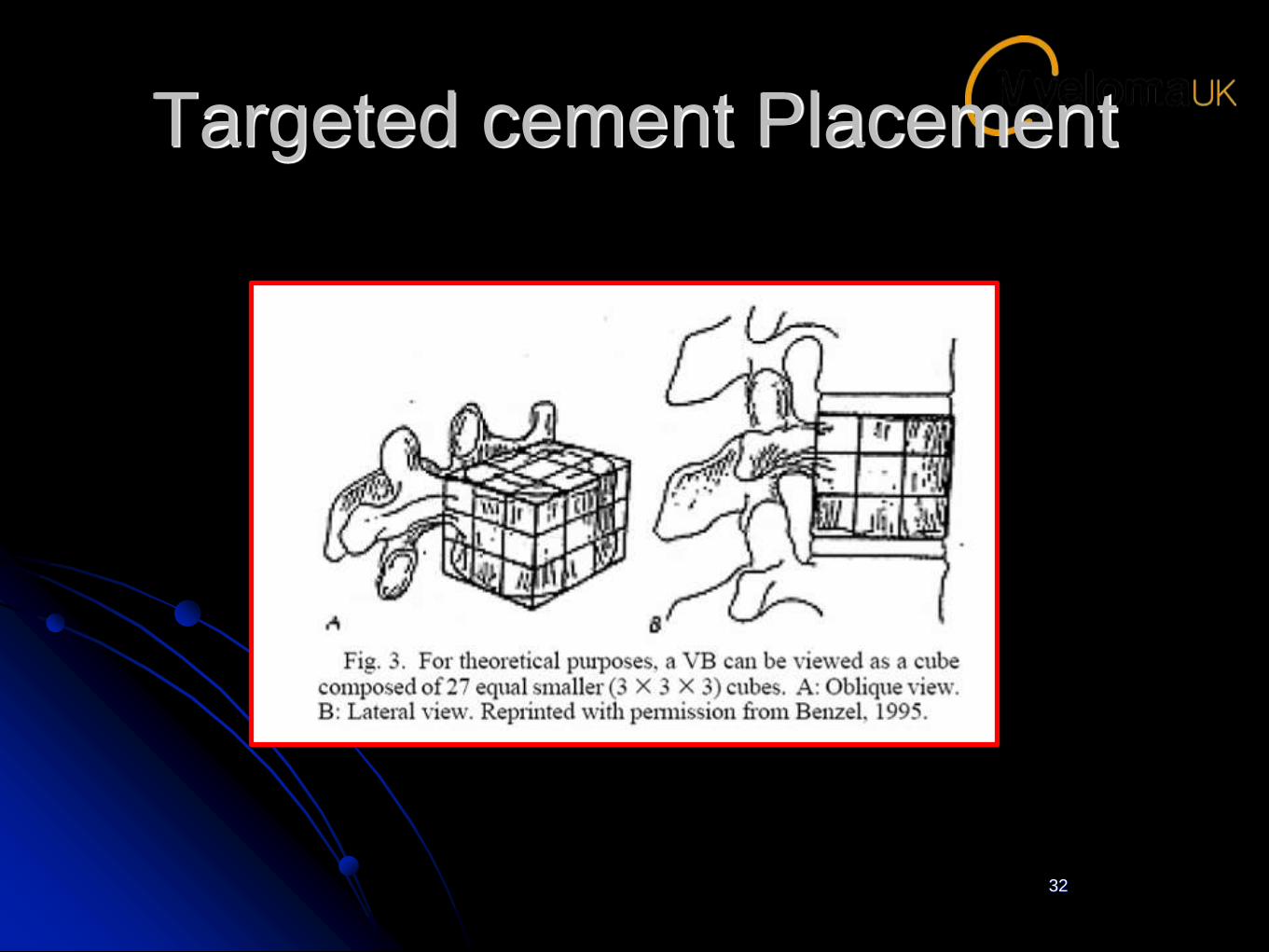
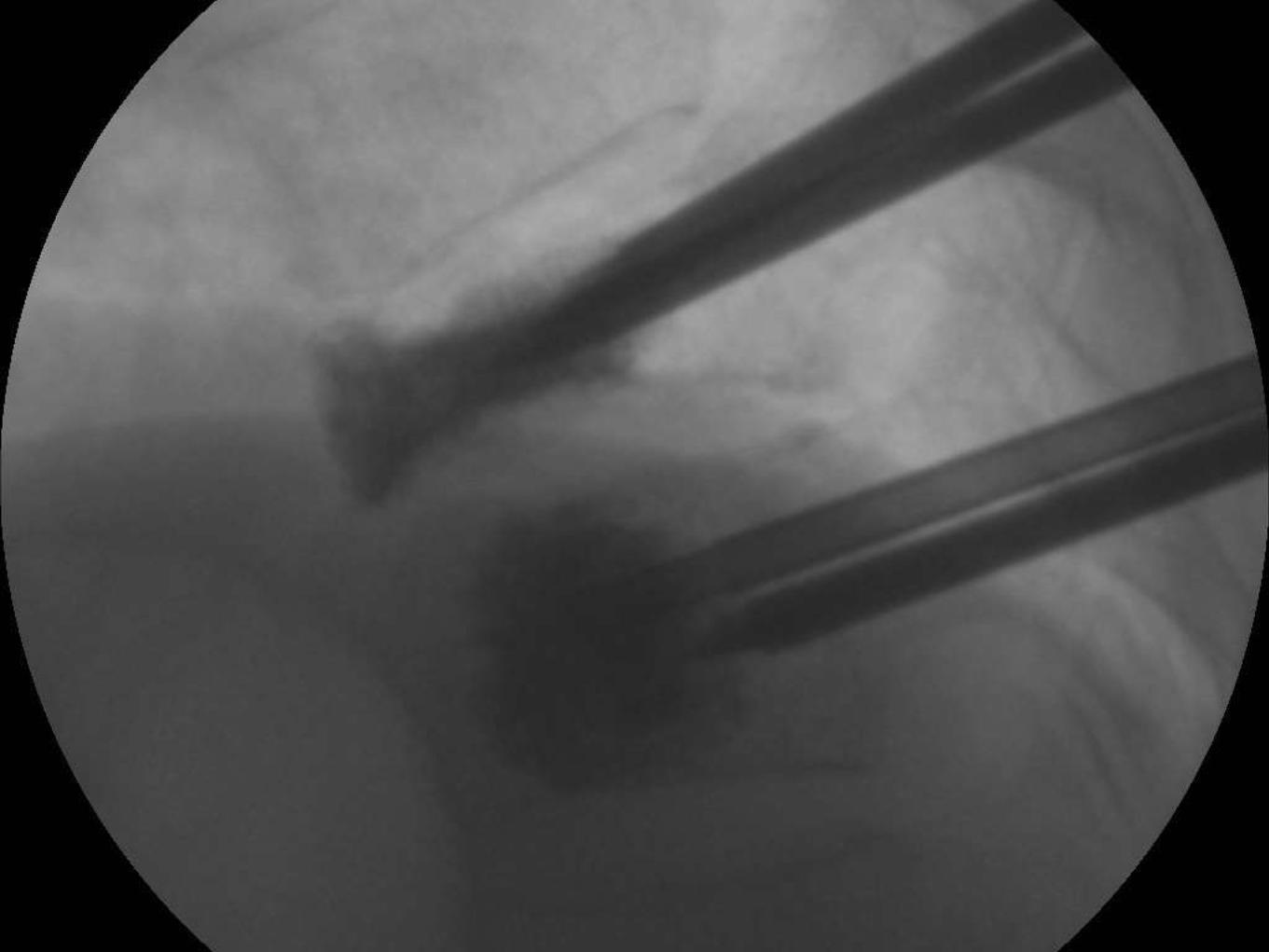
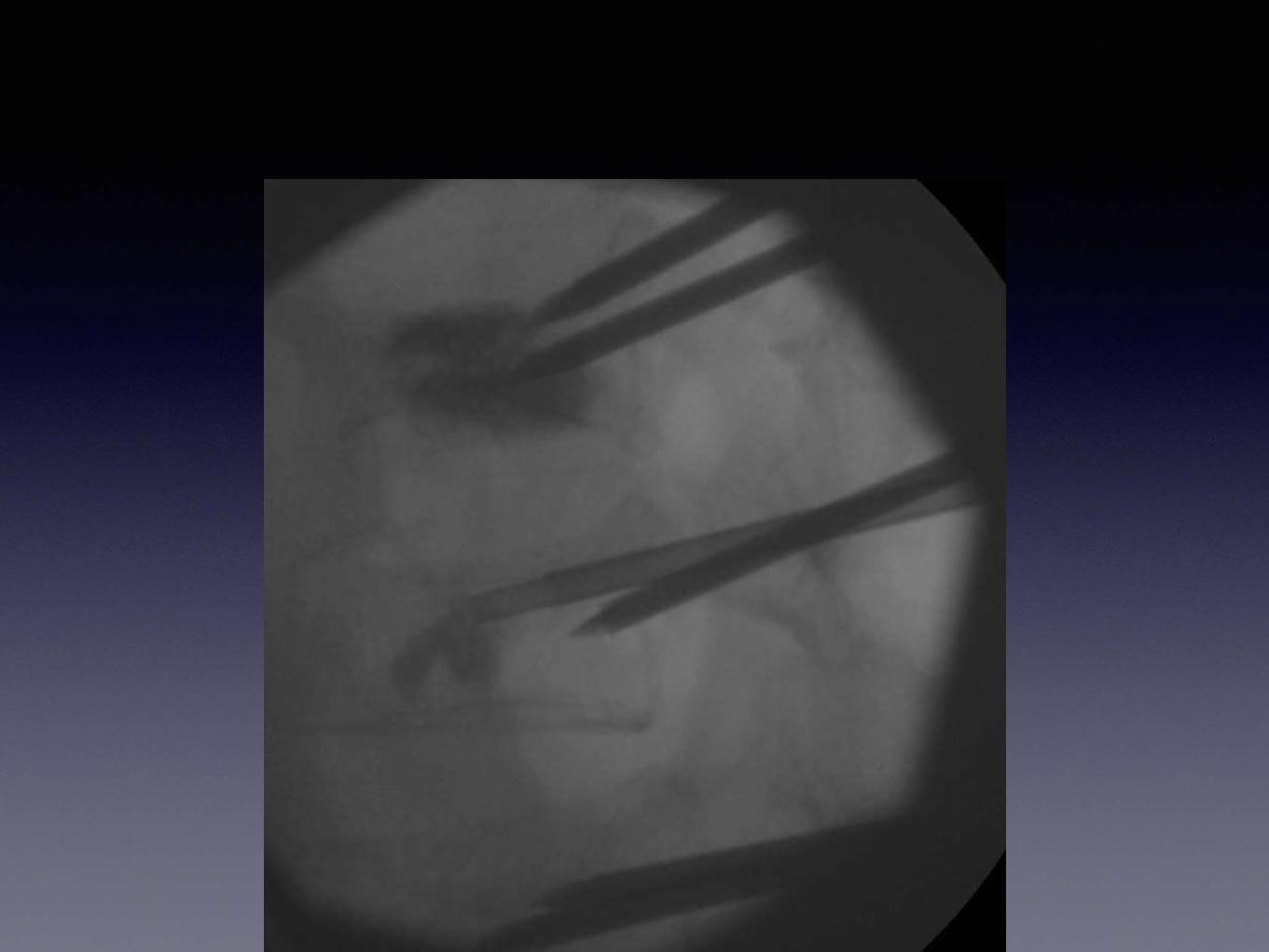
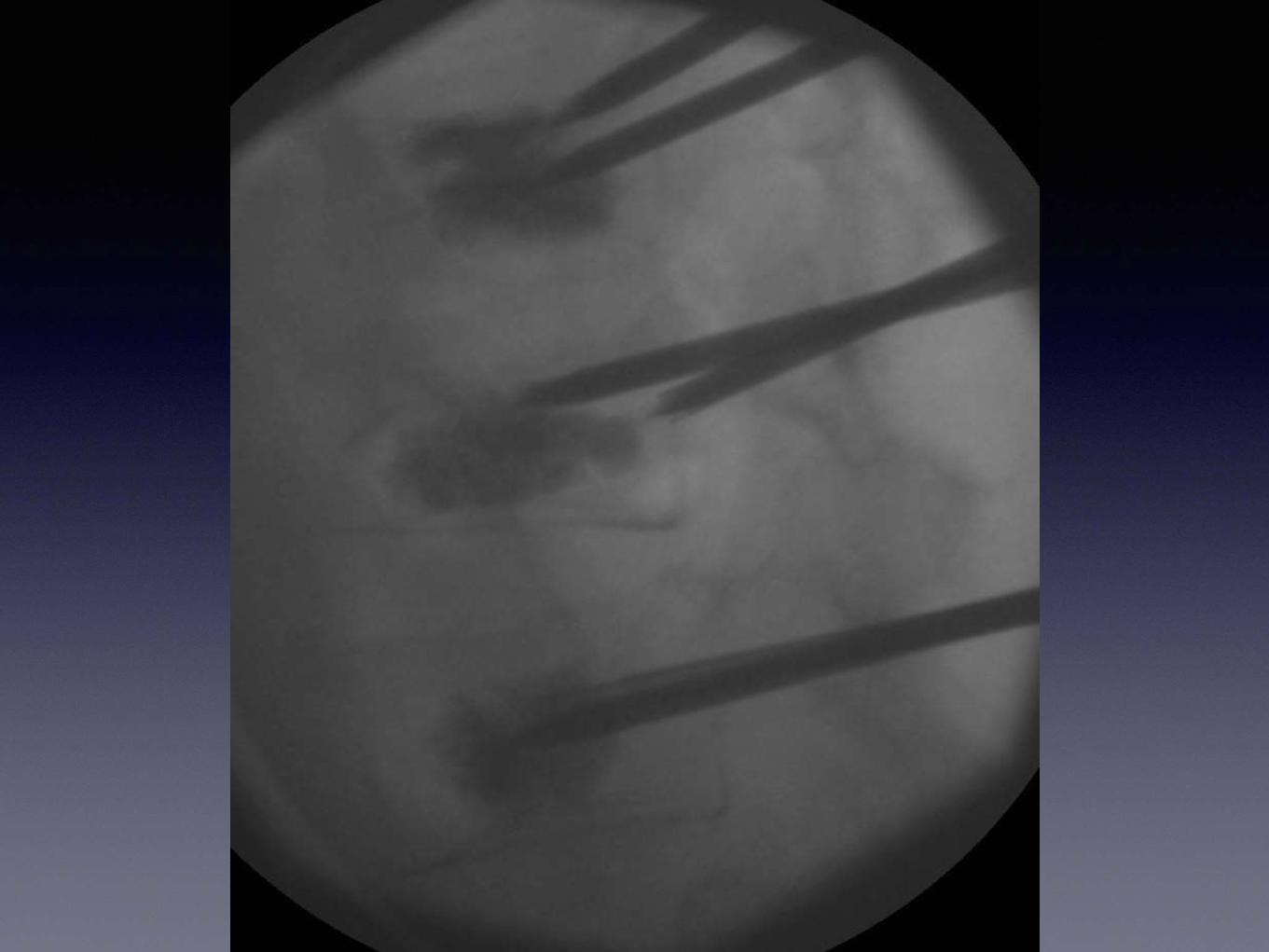
Targeted cement Placement
32
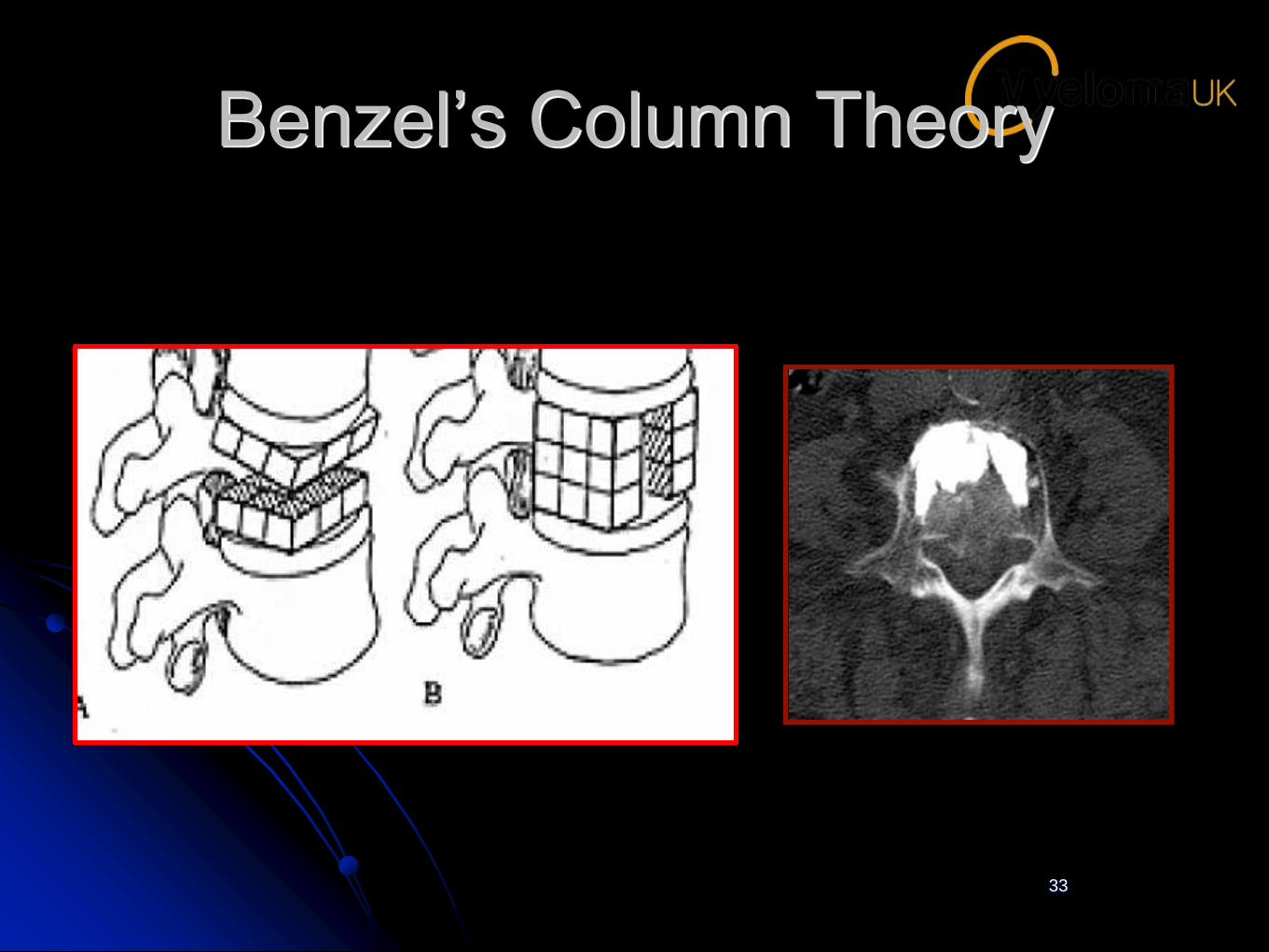
Benzel’s Column Theory
33
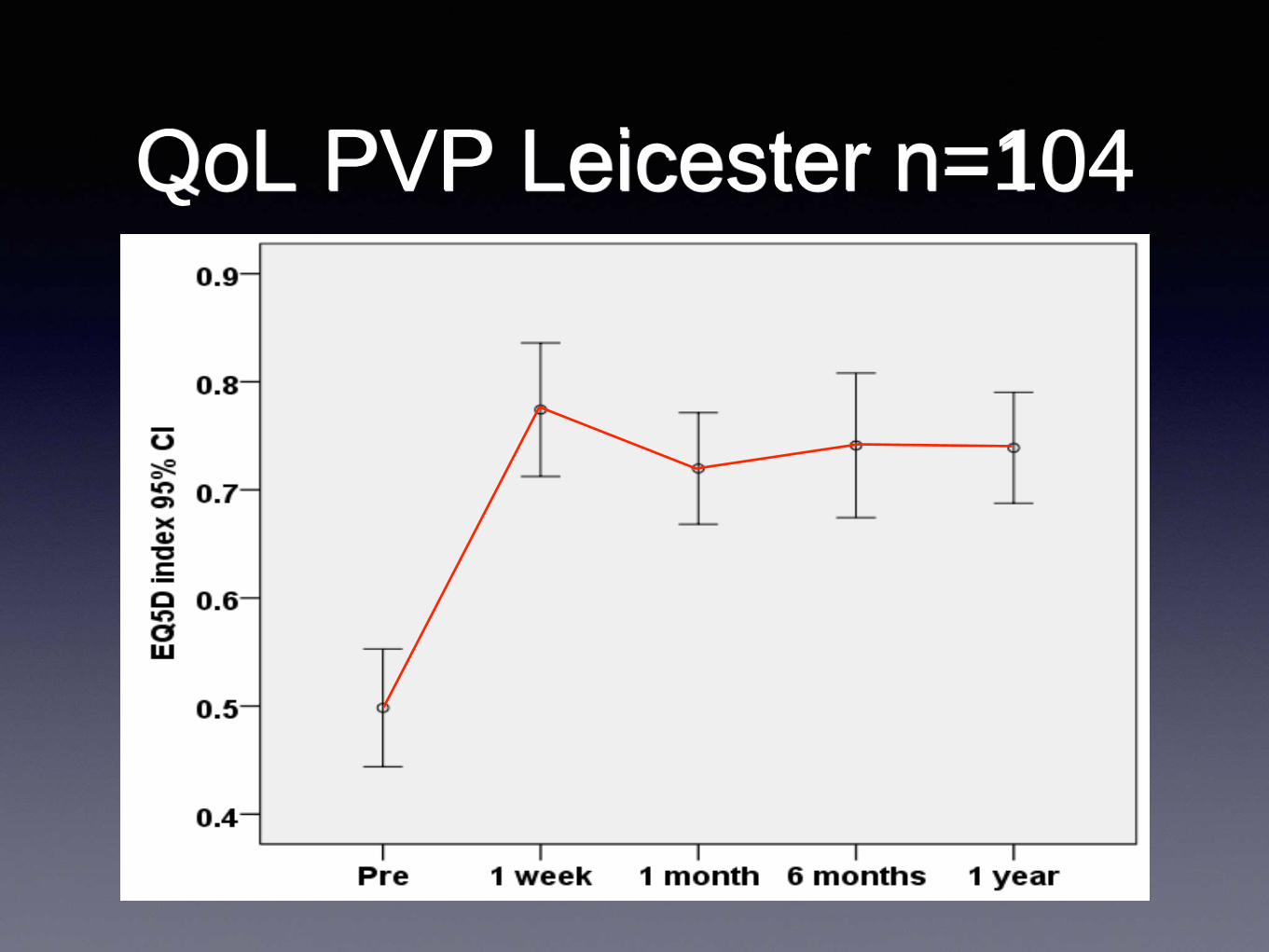
QoL PVP Leicester n=104
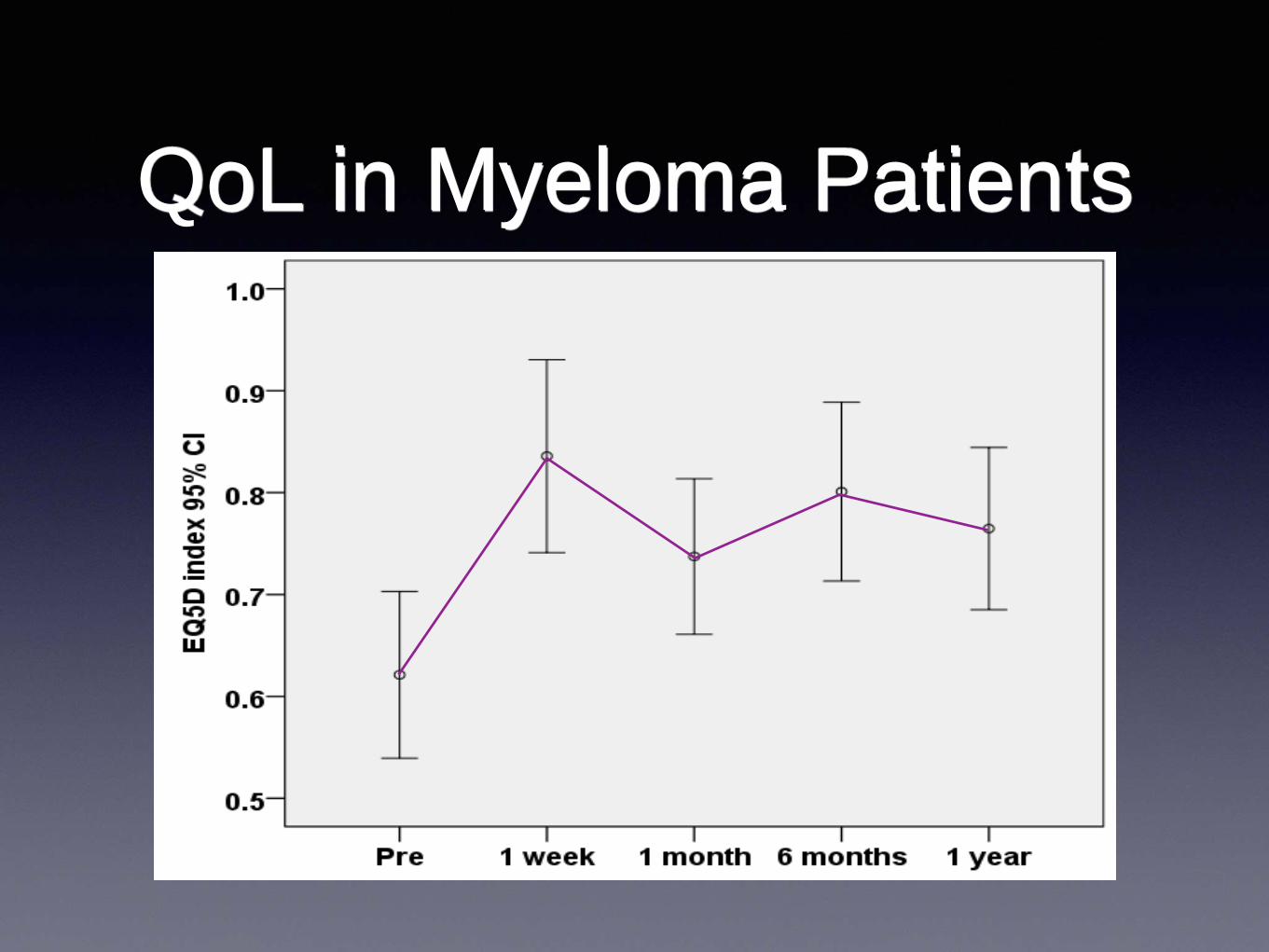
QoL in Myeloma Patients
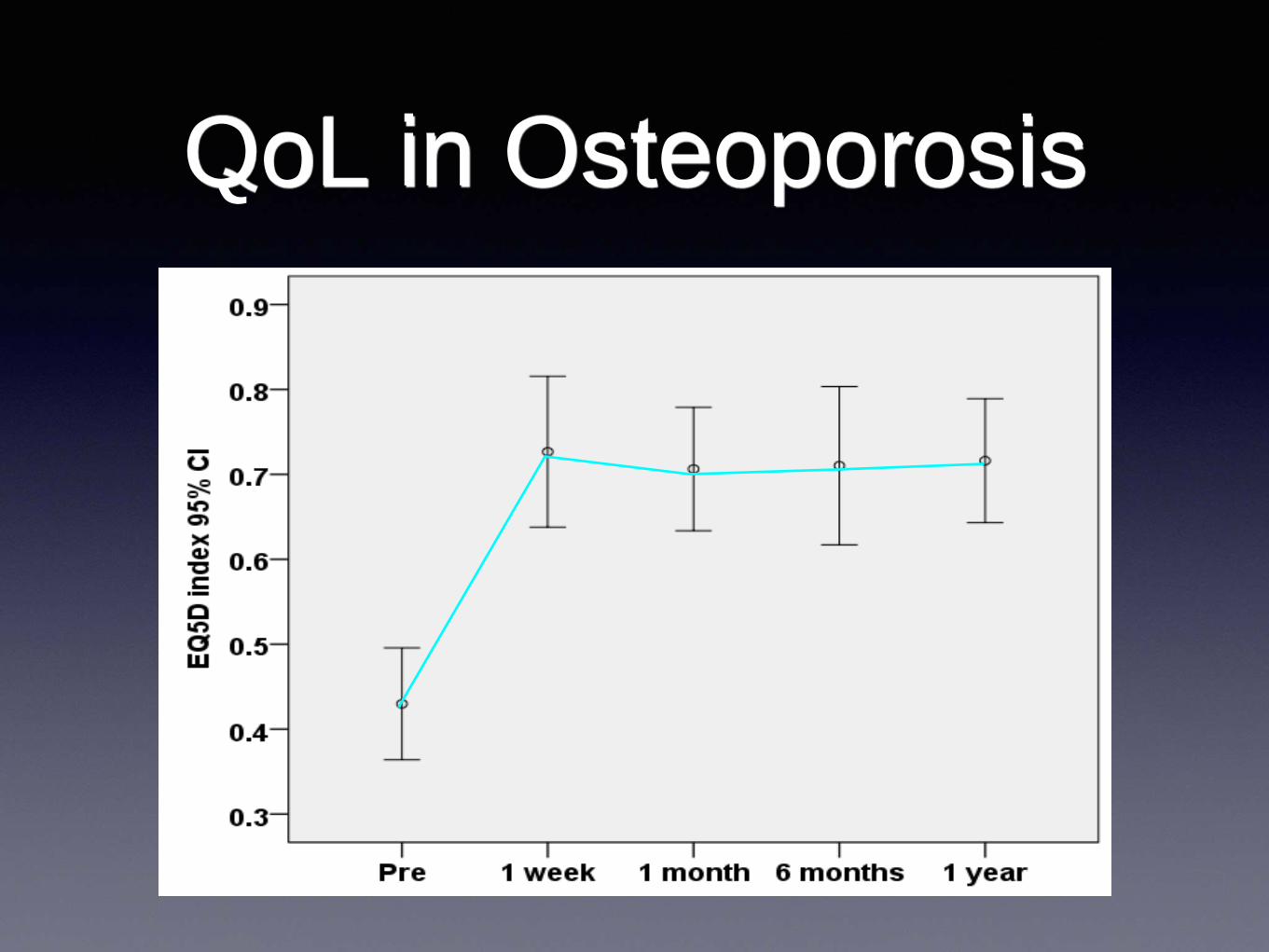
QoL in Osteoporosis
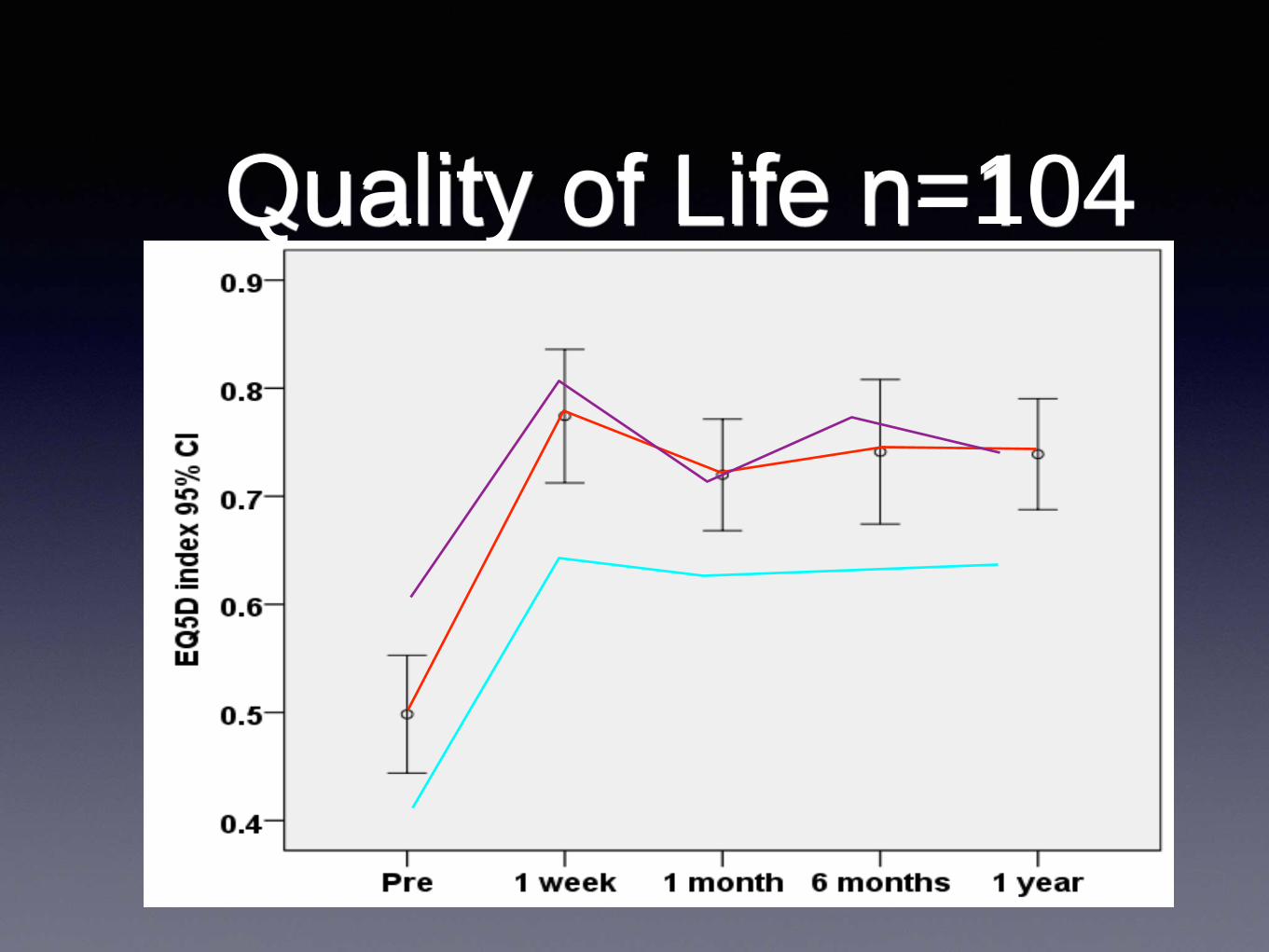
Quality of Life n=104
63
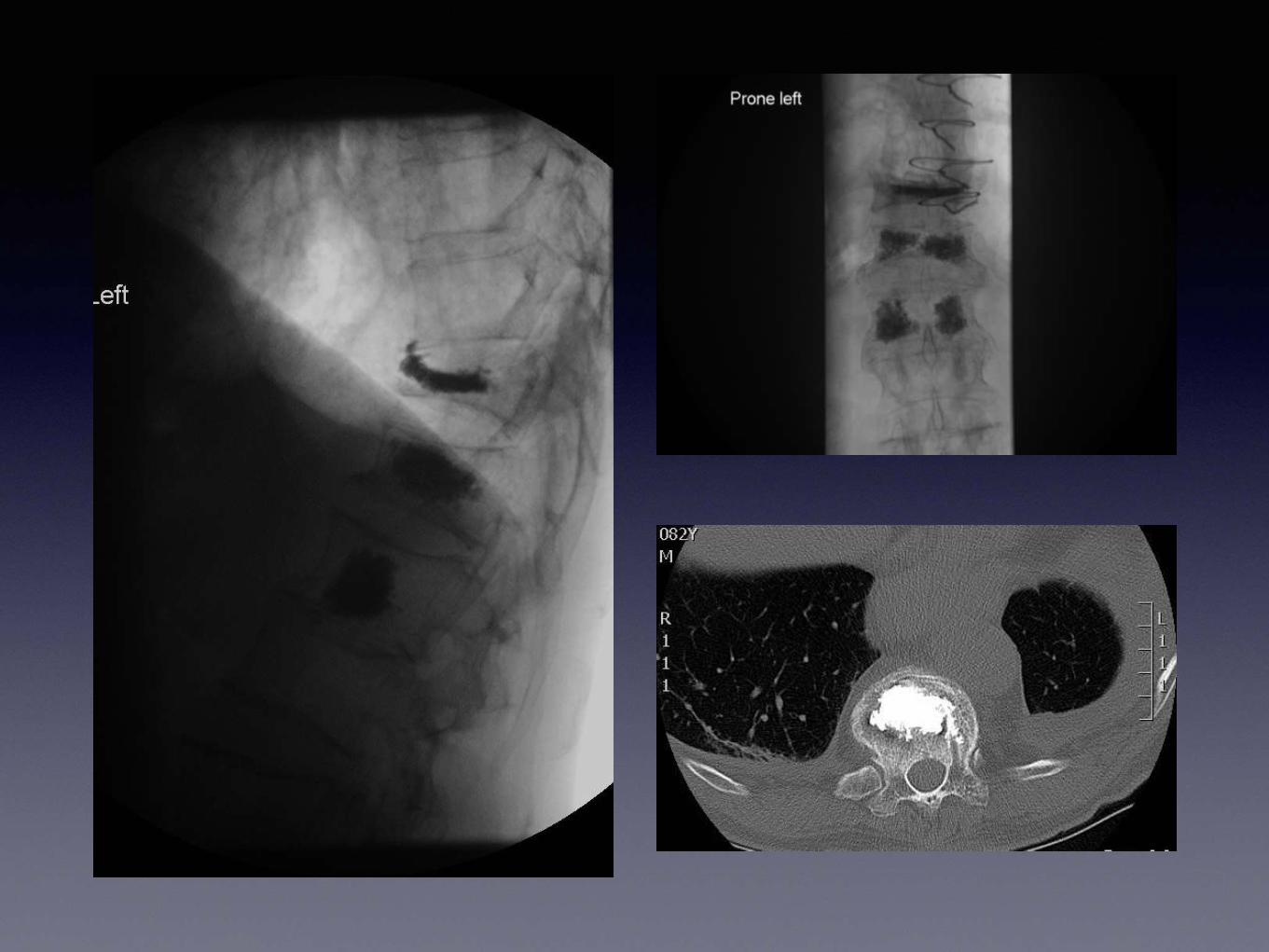
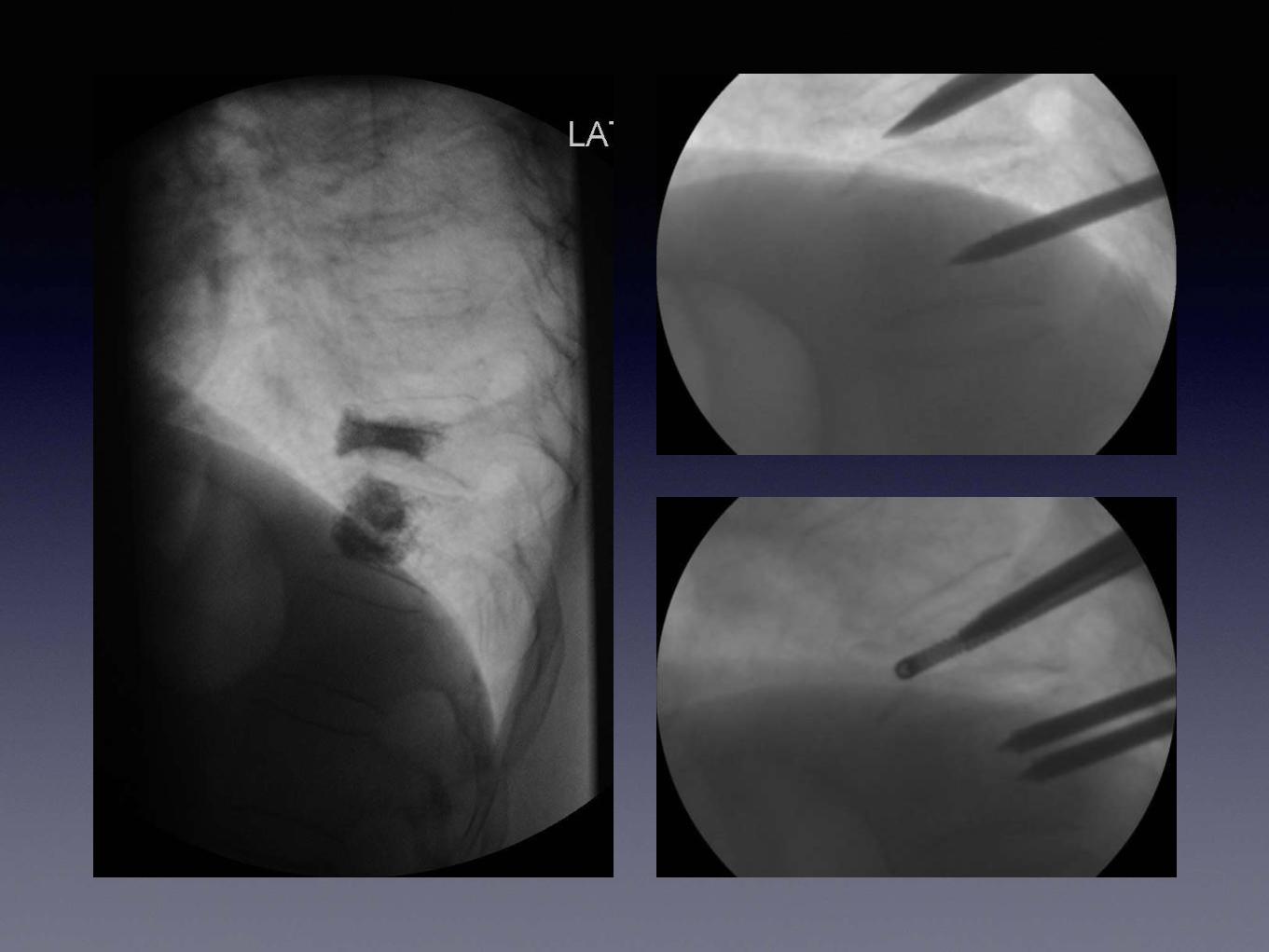
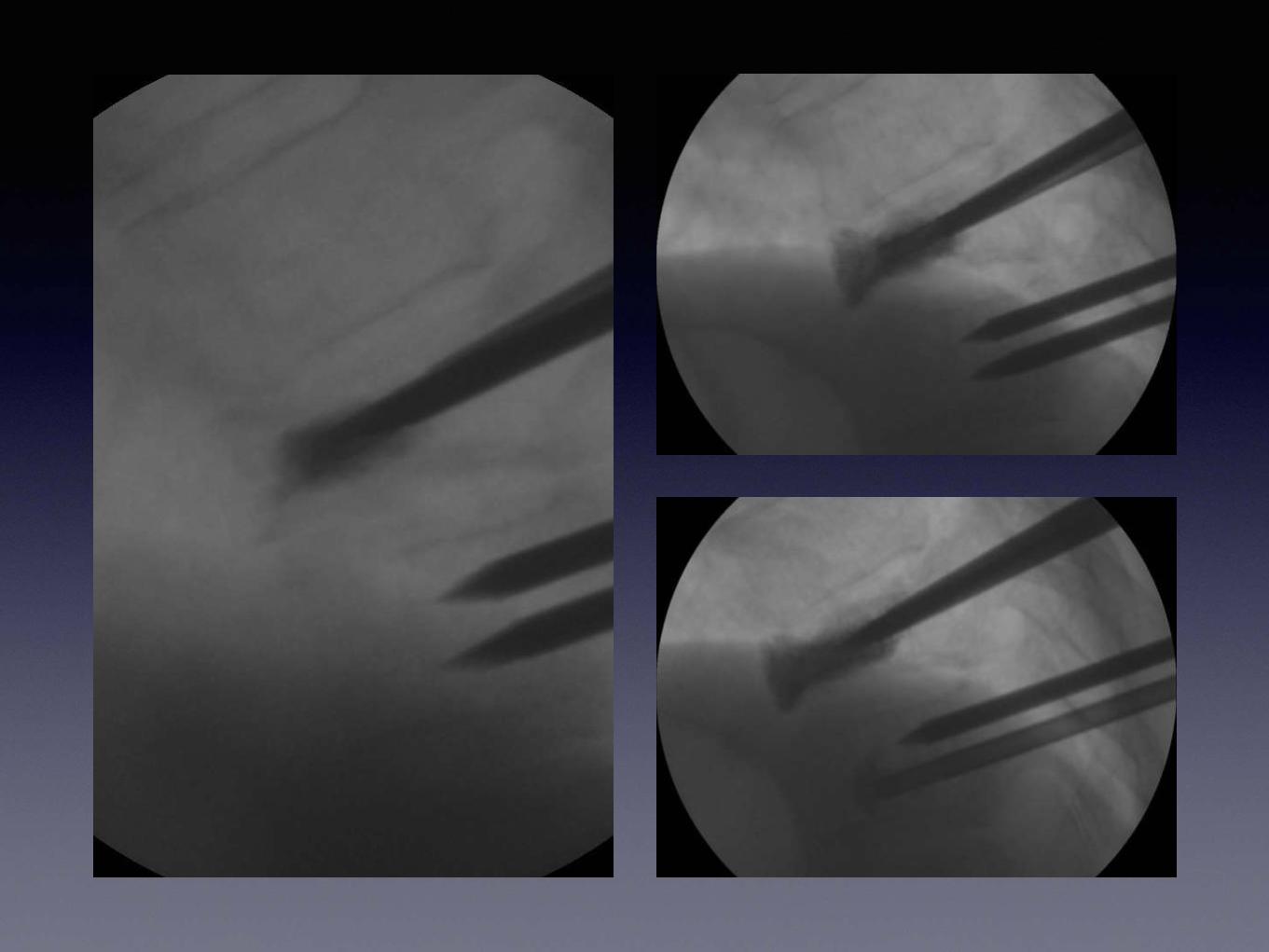
Case 1
• 82 male
• Osteoporosis,Degenerative joint disease,
Kummels disease, Multiple haemangiomata,
Mitral valve repair, Chronic pleural effusion.
• Pre assessment EQ 5D HS 50, M 2 SC 1 UA 3
PD 2 AD 2
Examination
• Erythema ab Igne over the region
• Focal tenderness to percussion
• 7month TTPre assessment clinic
• 11months RTT

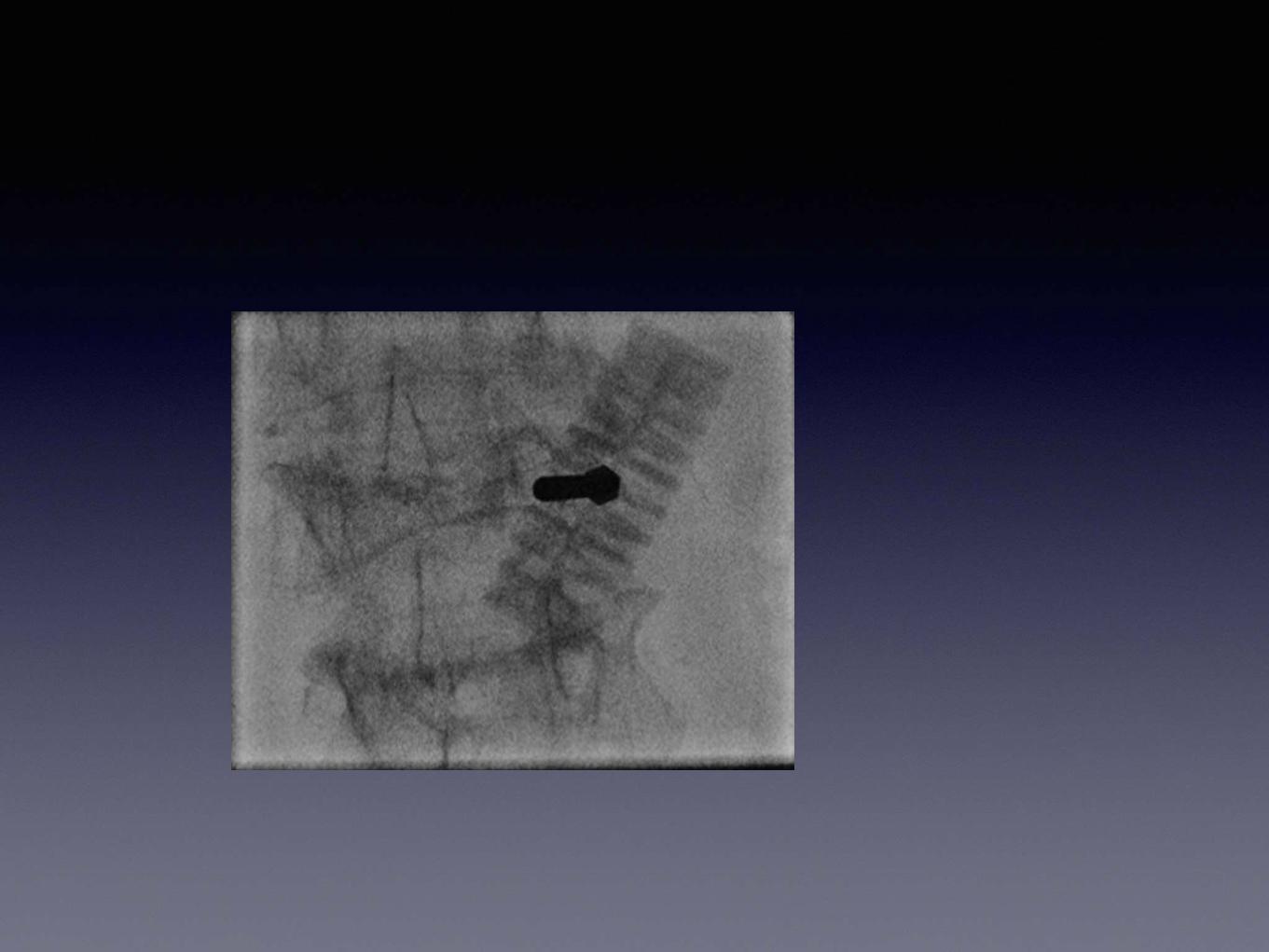
T11 - Fracture Cleft
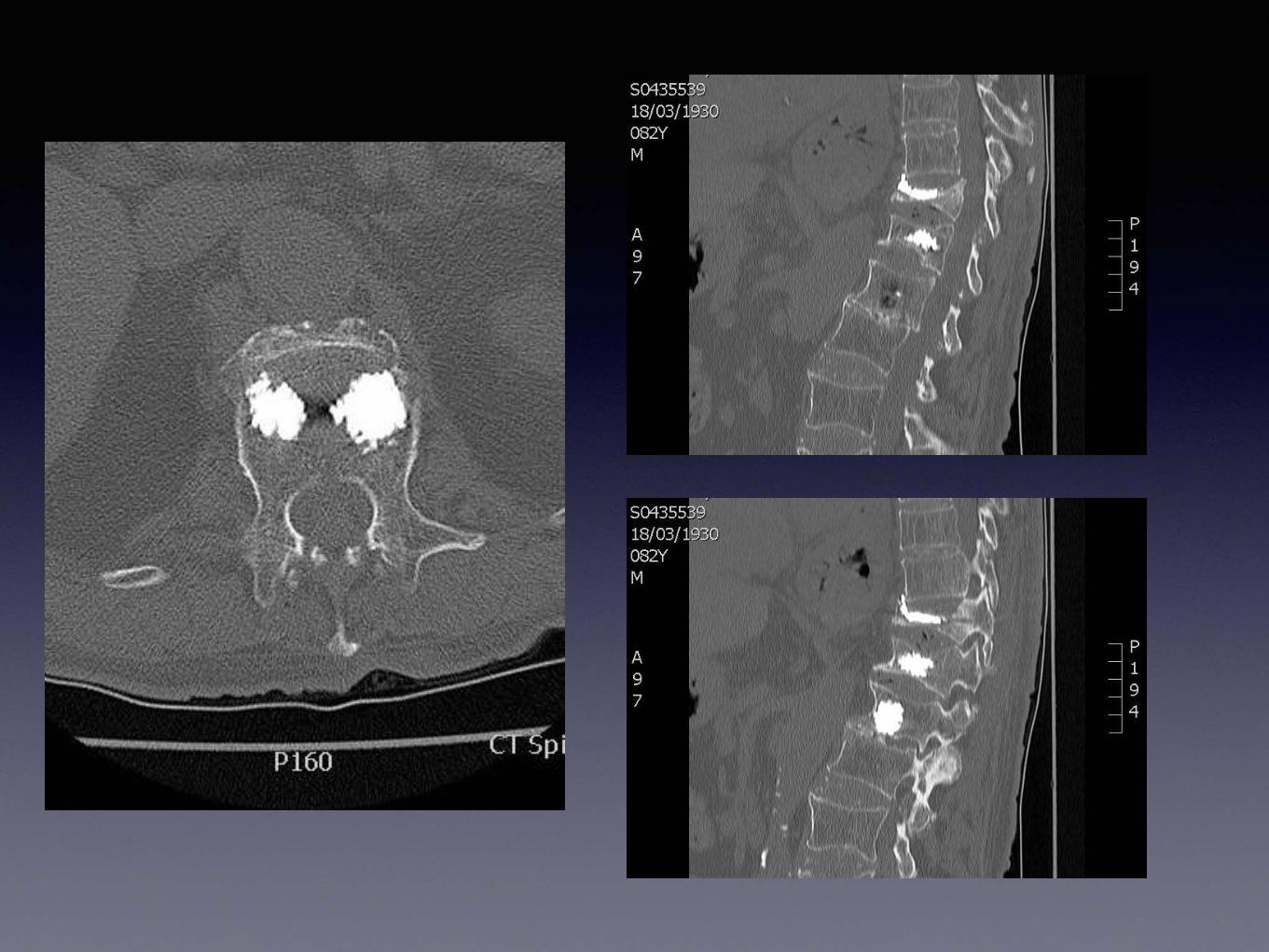
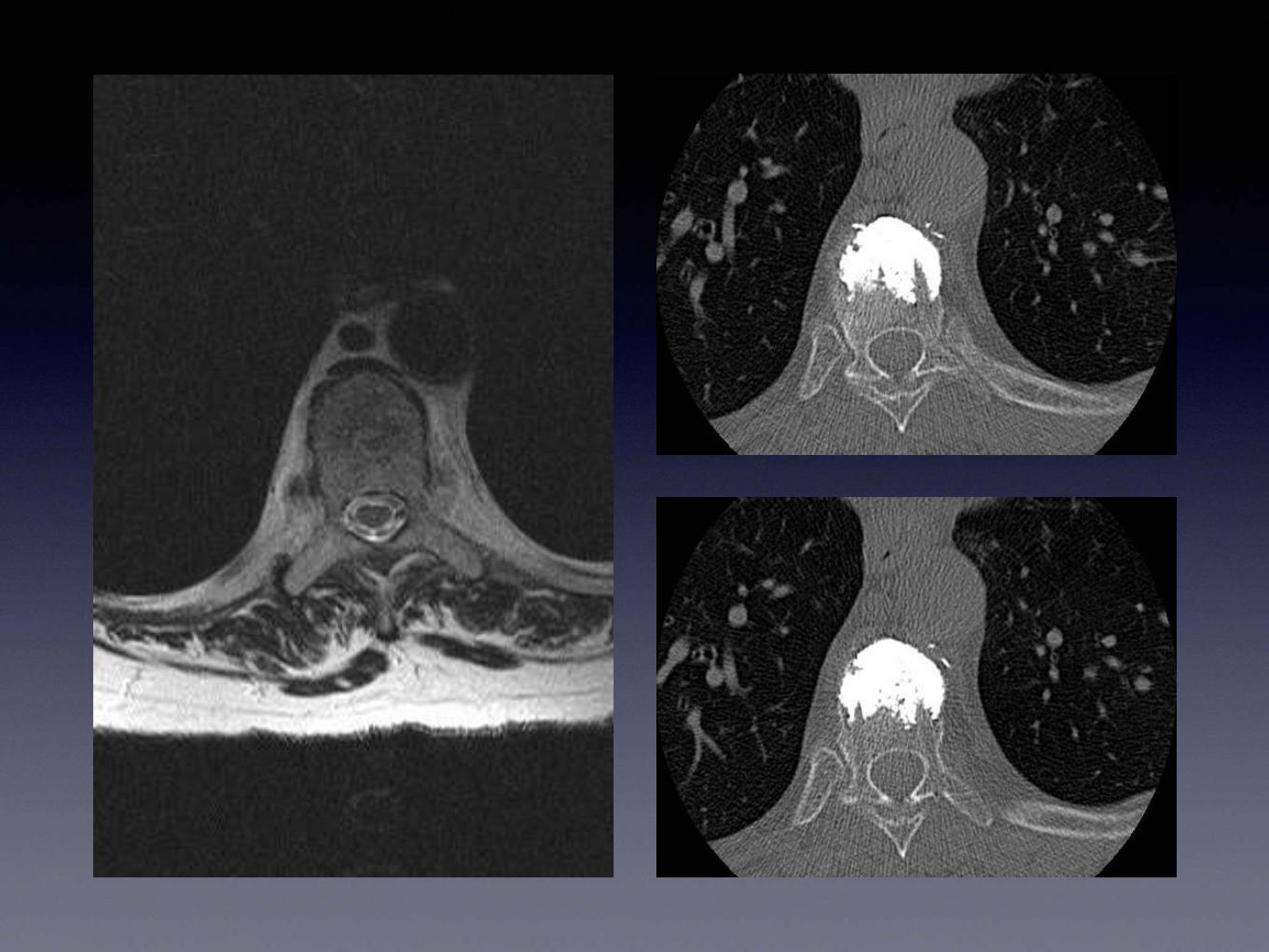
Case 2
• Xray “Worsening Osteoporosis T score -4.0”
• MRI - 3/12
• Pre Assessment 3/12
• Procedure 5/12
• RTT 11/12


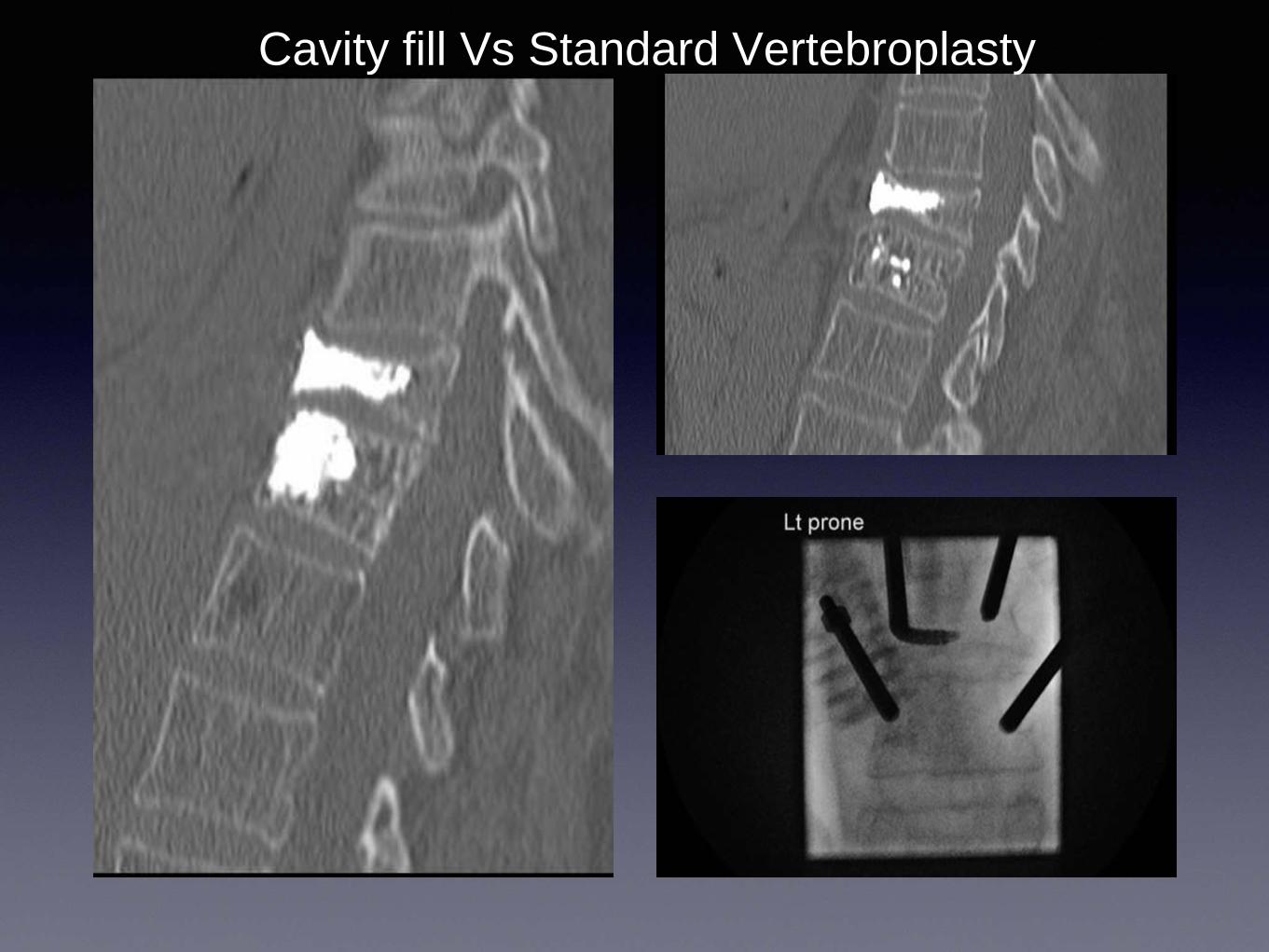
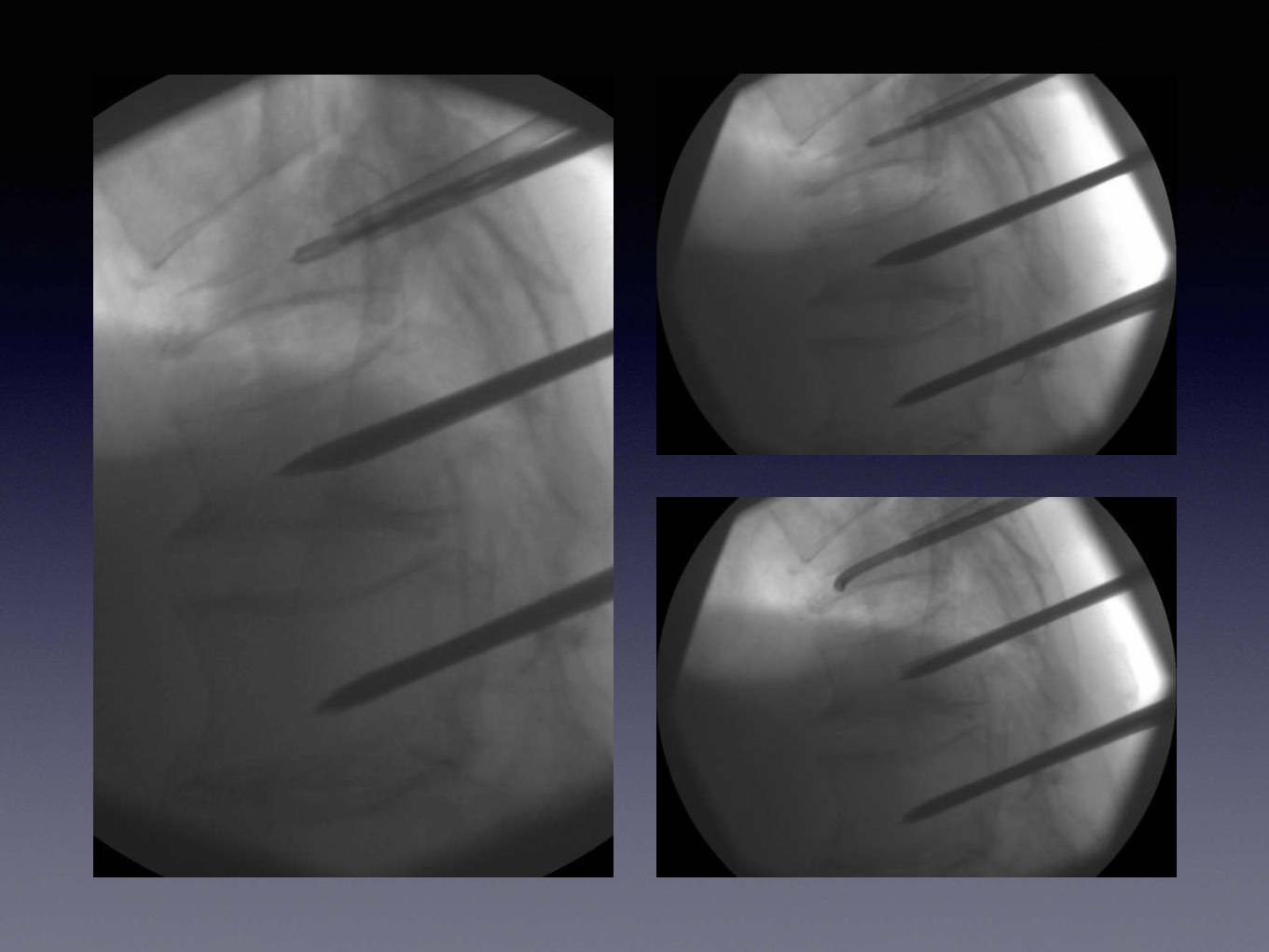
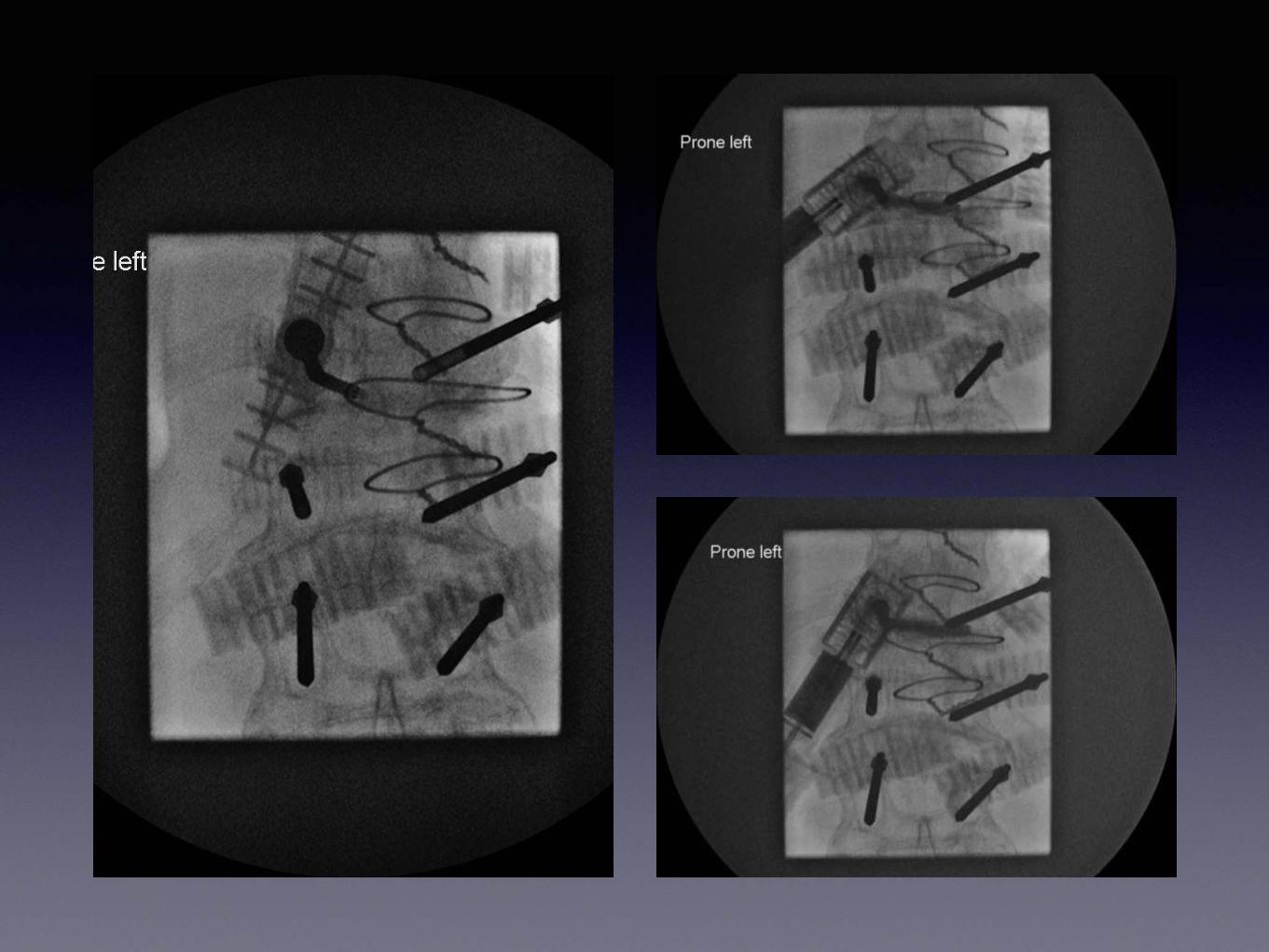
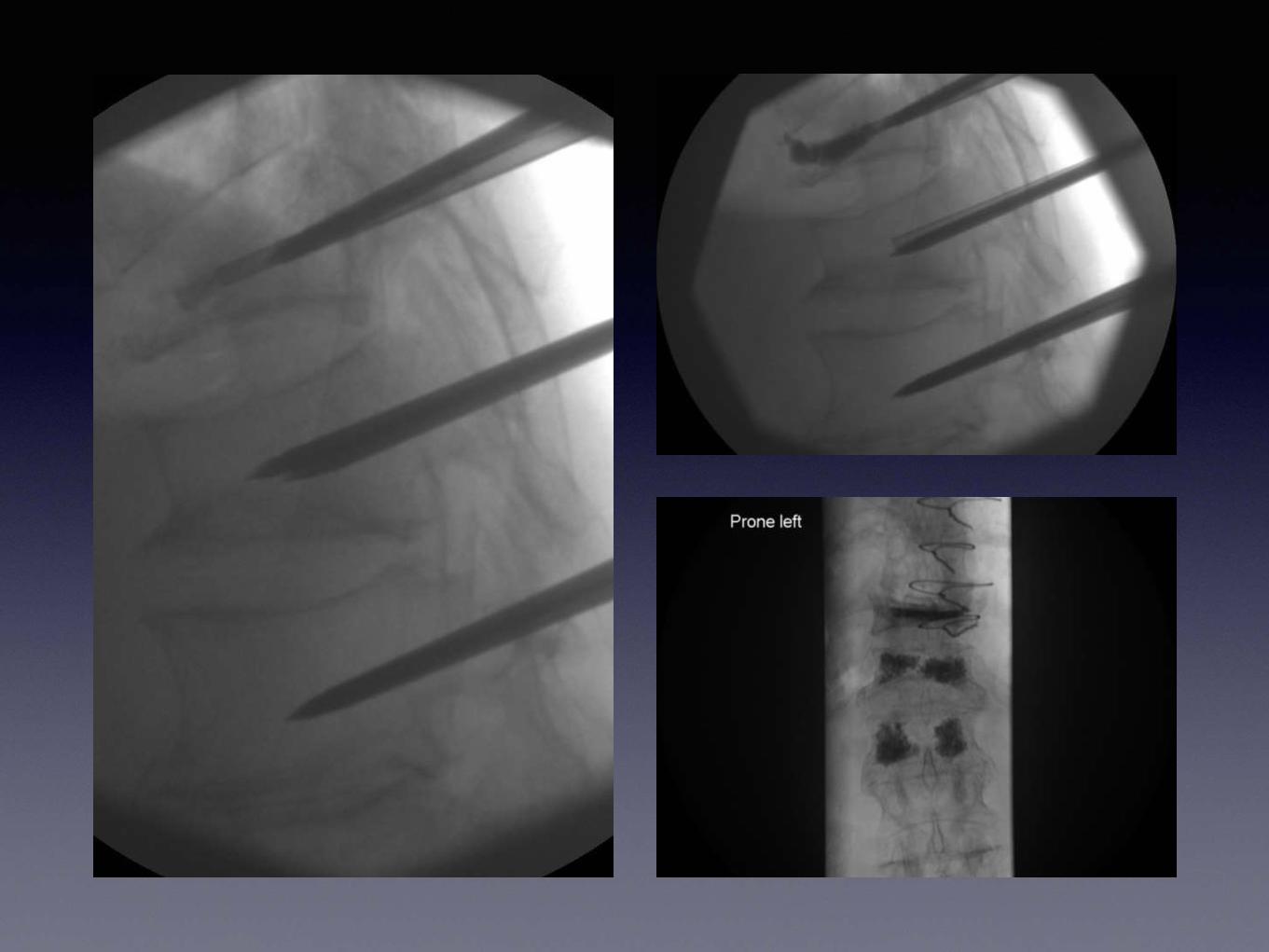
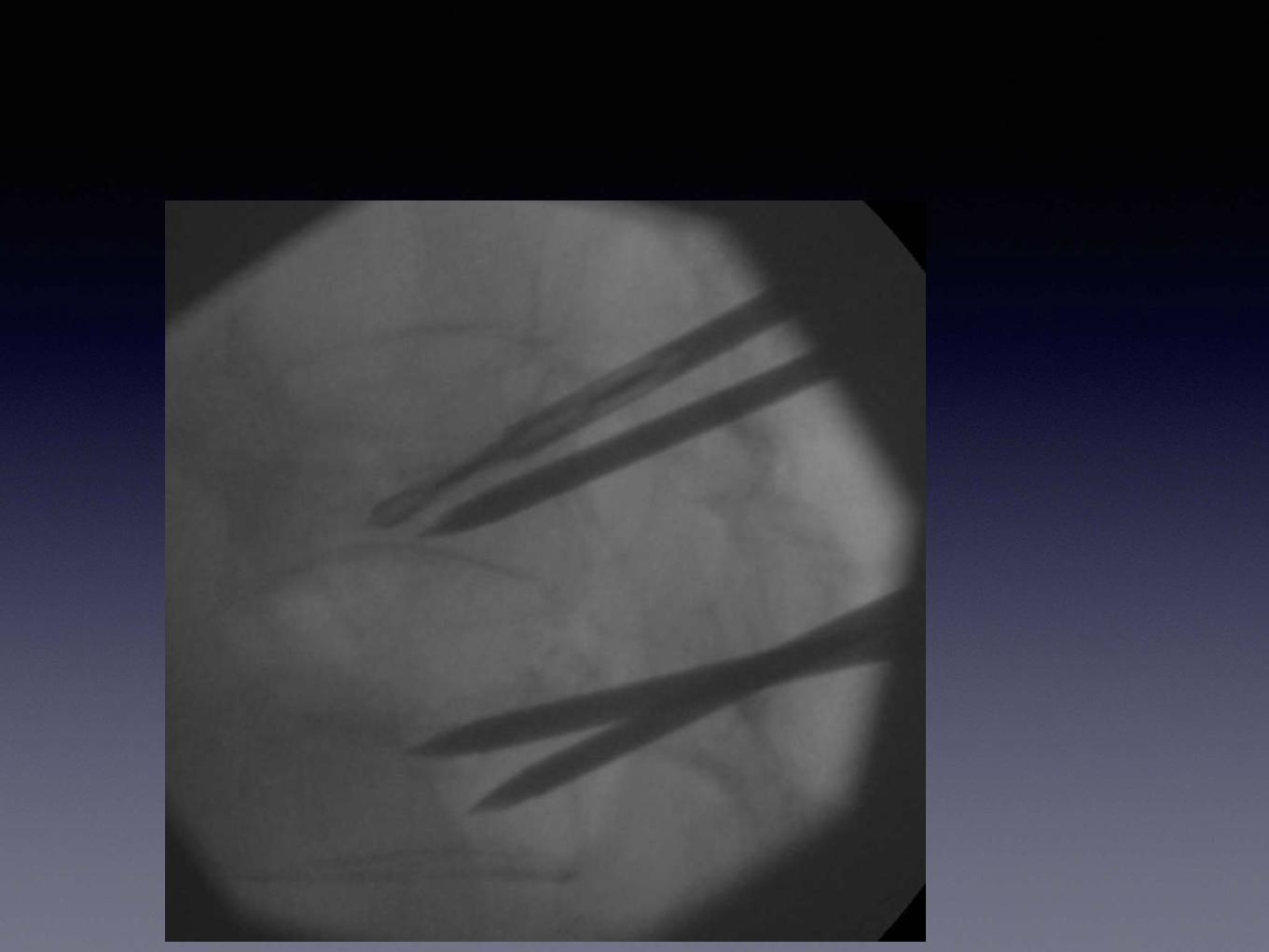
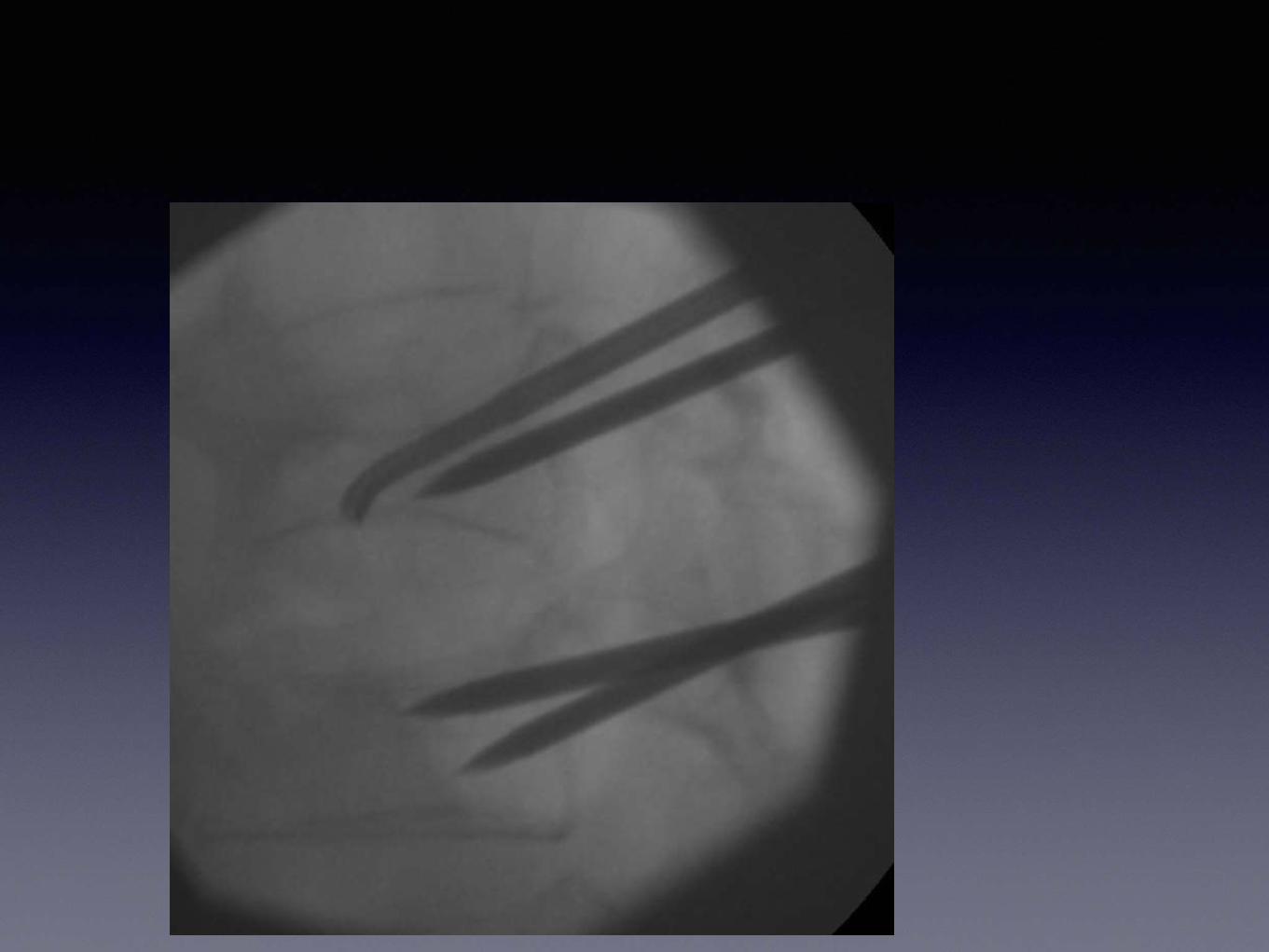
Cavity fill Vs Standard Vertebroplasty
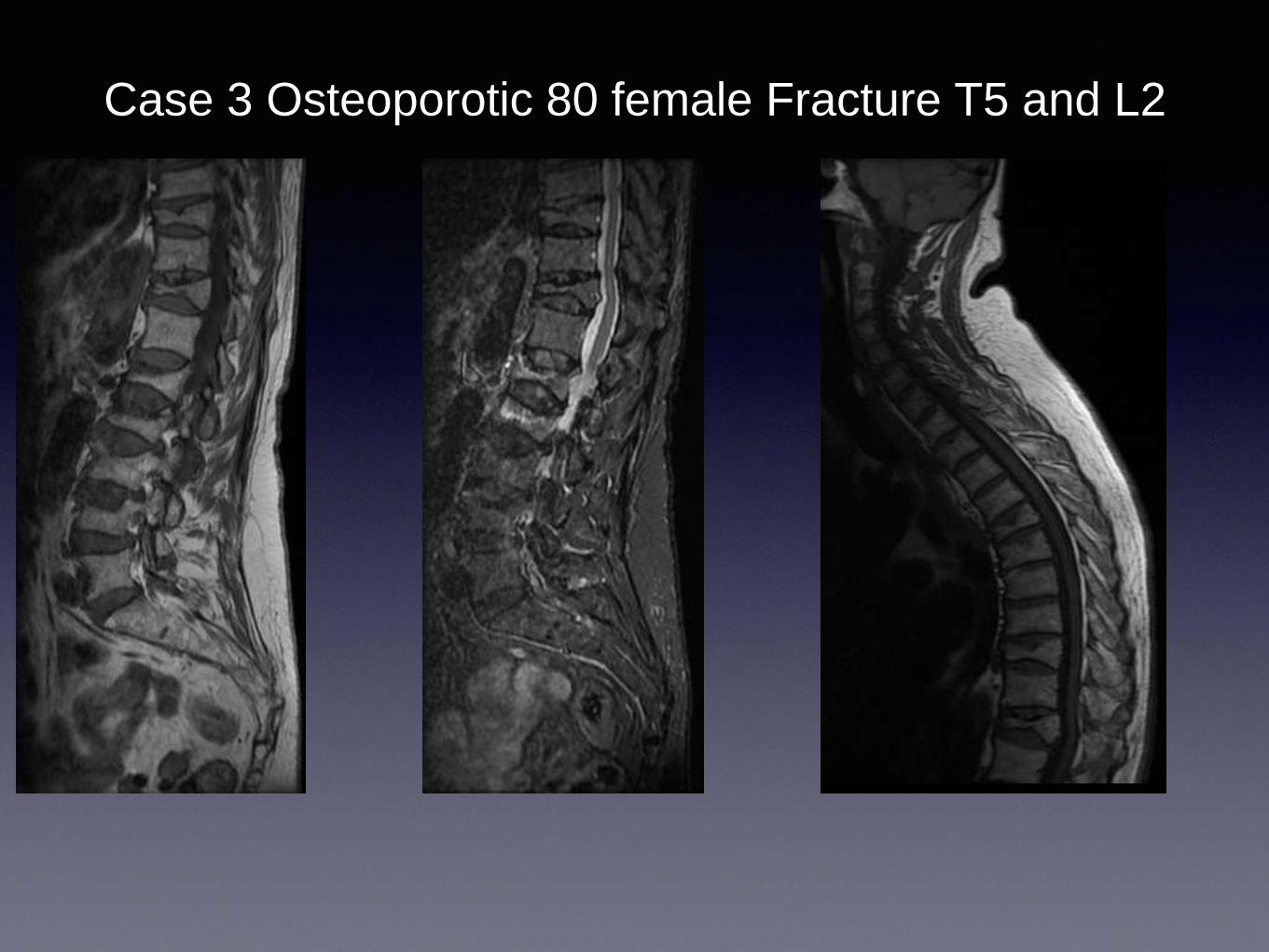
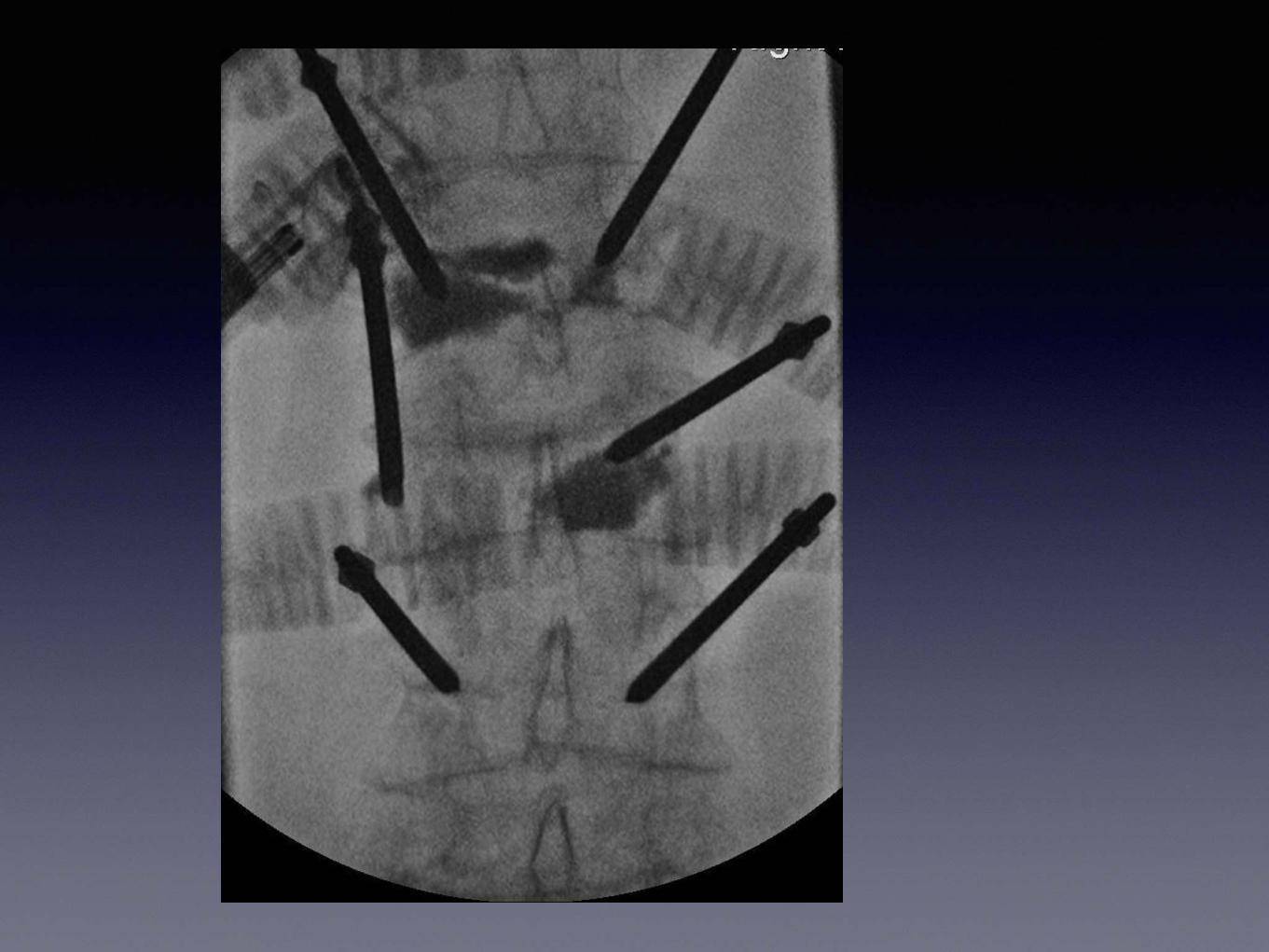
Case 3 Osteoporotic 80 female Fracture T5 and L2
Role of Prophylactic Cement
Augmentation• Redefine an osteoporotic fracture?
• Is loss of height too late for augmentation?
• Biomechanical segment cement augmentation
• ‘Prophylactic’ augmentation in unstable segments
• Targeted cementing with channel creation
• Columnar construct to prophylactic cementing
• Imperative that complications are low/nil- High Viscosity
“nanos gigantum humeris insidentes"
– Sir Isaac Newton
in a letter to Robert Hooke 1676
“If I have seen further it is by standing on the
shoulders of giants.”






![Achilles tenodesis for calcaneal insufficiency …...calcaneal avulsion fractures are fixation with cancel-lous screws, K wires, and tension band wiring [12]. There has yet been a](https://img.pdfslide.net/doc/110x75/5fa08abcc2639d15086b8046/achilles-tenodesis-for-calcaneal-insufficiency-calcaneal-avulsion-fractures.jpg)