Embed Size (px)
Citation preview

By Dr DEEPAK KUMAR DAS
MOD- PROF. R. KAPOOR
PGIMER, CHANDIGARH

ANATOMY
Located anterior and inferior to thyroid cartilage
Consists of two lateral lobes connected by central isthmus
Lateral lobes extend superiorly to the level of midthyroid cartilage and inferiorly to the sixth tracheal ring
Lateral extent is just medial to common carotid artery
Recurrent laryngeal nerve, sympathetic trunk and phrenic nerve are immediately posterior to the gland

BLOOD SUPPLY AND LYMPHATIC DRAINAGE
Blood supply is by paired superior thyroid artery ( branch of external carotid artery) and inferior thyroid artery
First-echelon nodes for thyroid metastasis are located in level 6( paralaryngeal, paratracheal and prelaryngeal nodes)
Second-echelon nodal spread is to level 3 and 4, supraclavicular nodes and upper mediastinal nodes ( level 7)
Retropharyngeal node involvement is unusual and can be encountered in case of advanced disease

PHYSIOLOGY

ETIOLOGY Most important risk factor for differentiated thyroid cancer is previous
irradiation, especially before the age of 16 years
Other predisposing factors are:
- Genetic predisposition
- Hashimoto’ s disease
- Iodine content of the diet

PATHOLOGICAL CLASSIFICATION Follicular epithelial cell
-Differentiated thyroid cancer
papillary and mixed cell variant
Classic
Papillary microcarcinoma
Encapsulated variant
Follicular variant
Aggressive variants
a. Diffuse sclerosing
b. Tall cell variant
c. Columnar cell variant
Follicular cancer
a. Classic morphology- Follicular carcinoma
b. Hurthle cell variant

- Poorly differentiated thyroid cancer- Insular carcinoma
-Undifferentiated thyroid cancer( anaplastic carcinoma)Parafollicular cell ( C cell)
Medullary carcinoma Non epithelial tumors
- Lymphoma- sarcoma- hemangioendothelioma

PAPILLARY THYROID CANCER

PATHOLOGIC FINDINGS- Nuclear enlargement, hypochromasia, nuclear pseudoinclusions,
nuclear grooves and distinct nucleoli- After formalin fixation nucleus resemble “ Orphan Annie’s eyes”
Tall cell variant- At least 70% of the carcinoma is composed of cells that are at least
twice as tall as they are wide
( papillary thyroid cancer) ( tall cell variant)
FOLLICULAR CARCINOMA

Diagnosis of FC is dependent on the presence of one of two histologic features Tumor invasion through the entire tumour capsule or Tumor invasion into a blood vessel located in the tumour capsule or immediately outside the tumour capsule

HURTHLE CELL CARCINOMA-Also called as oncocytic carcinoma-Characterised by large cells with abundant granular eosinophilic cytoplasm- At least 75% of the tumour must be comprised of Hurthle cells to designate it Hurthle cell carcinoma
ANAPLASTIC THYROID CARCINOMA-Comprise <5% of all malignant thyroid neoplasms- Most aggressive form of thyroid carcinoma- Most patients are diagnosed at the age of 65 years or older- Usually accompanied by bulky mediastinal lymphadenopathy and distant
metastatic spread-Mean overall survival from the time of diagnosis is 3-6 monthMEDULLARY THYROID CARCINOMA-Comprise 5-10% of all thyroid cancer- Seen sporadically( 80%) or in association with familial multiple endocrine
neoplasia( MEN IIA, MEN IIB, pure familial MTC)

-50-70% of MEN associated tumour is multifocal, but sporadic tumors are more oftenunifocal-Prognosis depends on the tumour subtype
Non MEN familial> MEN associated> sporadic > MEN- Overall mean 10 year survival is 75-80%

CLINICAL PRESENTATION
Thyroid nodule ( 10-50% of solitary nodule)
Cervical lymphadenopathy
Hoarseness
Haemoptysis
Stridor
Dysphagea
Hyperthyroidism
Diarrhoea


INVESTIGATIVE WORK UP Complete hemogram, biochemistry
CXR
FNAC
- safe, easy, cheap and reliable test to distinguish between benign and malignant thyroid nodule
RESULTS OF FNAC
Degenerative condition( 75%)
Thyroid cyst
-Fluid should be sent for malignant cytology
Degenerative or colloid nodule
- < 1% risk of malignancy
Neoplastic condition( 4% positive, 11% suspicious)
Papillary neoplasm
- 90% accuracy in positive cases
- 60% accuracy in suspicious reports

Follicular neoplasm- Unable to distinguish between adenoma and well differentiated follicular carcinoma: biopsy required
Medullary carcinoma- Reliable test when combined with calcitonin staining
Anaplastic carcinoma- Usually diagnostic but may not distinguish from lymphoma or metastatic
carcinoma Lymphoma
- Open biopsy required for immunohistochemistry Inconclusive(10% cases)
-FNAC should be repeated under USG guidance

ULTRASONOGRAPHY-Most sensitive method for evaluating thyroid nodule- Ideally used in combination with FNAC for preliminary assessment- Distinguishes solitary thyroid nodule from dominant thyroid nodule in a multi-
nodular goitre- Assessing size and position of cervical lymphadenopathy

RADIONUCLIDE SCANNING
TECHNETIUM 99m
Uptake by thyroid gland is low.
Scans are neither sensitive nor specific
Information is provided in terms of hot or cold nodules

I123Ideal No longer used as a first line investigation of thyroid nodule Involuble for total body imaging post total thyroidectomy in case ofwell differentiated thyroid cancer

DMSA AND MIBG scan May locate recurrent or metastatic disease in case of medullary carcinoma Not taken by cells as readily as I123 in differentiated cancer and positive
scans occur only in 30% cases

CT/MR IMAGINGINDICATIONNECK
Possible bilateral involvement
Extrathyroid invasion of trachea, larynx, esophagus, carotid vessels
LN involvement
THORAX
Retrosternal spread
Superior mediastinal nodes involvement
Pulmonary metastasis in MTC/ anaplastic carcinoma
ABDOMEN
Exclusion of pheochromocytoma in MTC
Liver metastasis in MTC/ anaplastic carcinoma
Lymphoma staging

Main disadvantage with CT scan is the necessary administration of iodine contrast which can block both diagnostic and therapeutic useof radioiodine for 6 months.
MR involves neither radiation or iodine and with better diagnostic abilityis the investigation of choice in differentiated thyroid cancer

TFT- Free serum T3, T4 and TSH- Indicated in all patients of thyroid cancer
Thyroid autoantibodies- Anti-microsomal, antithyroglobulin- Indicated if Hashimoto’s disease or thyroid lymphoma suspected
Tumor markers- Thyroglobulin, calcitonin, CEA- Preoperatively in all cases- Proven role in monitoring and follow up- Calcitonin also helps in initial diagnosis

Peak calcium infusion- less than or equal to 130 pg/ml in males- less than or equal to 90 pg/ml in females
Basal calcitonin levels are high in most patients with sporadic MTC but are normal in those with familial MTC or MEN type 2
So in these patients a calcium infusion provocative test or pentagastrininfusion test is used todetect the abnormality
CALCITONIN

OTHER INVESTIGATION Indirect or fibreoptic laryngoscopy to assess vocal cord
and/or intratracheal disease is indicated in all patients with suspected thyroid malignancy.
Mandatory for both preoperative and post operative assessment

STAGING SYSTEMS OF THYROID CANCER

AGES, Mayo clinic, 1987Age>40, grade>1, extrathyroid extension, size>3 cm

AMES( Lahey clinic, 1988)
40 year survival for low risk group was 95% and 45% for high risk group

GAMES( MSKCC 1992)Grade>2, age>45 years, distant metastasis, extension beyond thyroid capsule,Size> 4 cm

MACIS( Mayo Clinic, 1993)Metastasis, Age>40, Completeness of resection, Extrathyroid invasion, Size

DAMES( Karolinska Institute, 1992)DNA ploidy, Age> 40 year in female and 50 year in male, Metastasis, Extension beyondThyroid capsule, Size> 5 cm

AJCC 2010 TNM STAGING SYSTEMTx Primary tumour cannot be assessed
T0 No evidence of primary tumour
T1 Tumour 2 cm or less in greatest dimension and limited to the thyroid gland
T1a Tumour 1 cm or less in greatest dimension and limited to the thyroid gland
T1b Tumour > 1cm but not > 2 cm in greatest dimension and limited to thyroid gland
T2 Tumour > 2 cm but not > 4 cm in greatest dimension and limited to the thyroid gland
T3 Tunour > 4cm in greatest dimension limited to the thyroid or any tumour with minimal extrathyroidal extension to the sternothyroid muscle or perithyroid soft tissue
T4 Advanced disease defined as more than minimal extrathyroid extension
T4a Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve
T4b Tumor invades prevertebral fascia, encases carotid artery or mediastinal vessels

STAGING CONT......
All anaplastic carcinomas are considered T4 tumors
T4a Intrathyroidal anaplastic carcinoma
T4b Anaplastic carcinoma with gross extrathyroidal extension
Regional lymph node(N)
Nx Regional LN cannot be assessed
N0 No evidence of regional LN metastasis
N1 Regional LN metastasis
N1a Metastasis to level VI
N1b Metastasis to unilateral, bilateral, contralateral cervical or retropharyngeal or superior mediastinal LN
Distant metastasis
M0 No distant metastasis
M1 Distant metastasis

COMPOSITE STAGING


MANAGEMENT
Surgery
-Lobectomy or total thyroidectomy
- Extent of neck dissection
Hormonal therapy
Radioactive iodine therapy
EBRT
Chemotherapy

SURGERY Surgery is the primary treatment of localised thyroid cancer of all
histologies
Total thyroidectomy is the preferred oncologic procedure, because
- The gland is surgically accessible
- Its primary endocrine function can be replaced by exogenous
hormones
Even a total thyroidectomy leaves residual thyroid tissue that will have major implication for subsequent therapy and disease monitoring
-The ligament connecting the posterior surface of thyroid capsule
to the trachea harbors microscopic nests of thyroid tissue and is
rarely completely resected in order to reduce the risk of tracheal
injury
- Recurrent laryngeal nerve is embedded in thyroid tissue at the
point where nerve enters the larynx and it is not possible to
remove all of the thyroid tissue without injuring the nerve and
compromising voice quality and laryngeal function

There are three critical issues regarding the surgical management of thyroid CancerWhen is surgery indicated for the evaluation of a thyroid nodule with non-
diagnostic cytologyWhen is it safe to consider hemithyroidectomy for thyroid carcinomaWhat is the appropriate extent of neck dissection

SURGICAL EVALUATION OF THYROID NODULE
Cytology is suspicious for PTC
Cytology contains follicular cells with no concordant functioning nodule on an RAI scan, especially with low to normal range serum TSH
Cytology contains Hurthle cell neoplasm, which does not warrant an RAI study and should be managed with lobectomy or total thyroidectomy, depending on the lesion’ s size and other risk factors
Growing nodules, even in the face of benign cytology

LOBECTOMY IN THE MANAGEMENT OF THYROID CANCER
Age between the age of 15 and 45 years with PTC tumor <4 cm
No prior radiotherapy
No distant metastasis
No cervical LN metastasis
No extrathyroidal extension
Absence of aggressive histologic variant
Completion thyroidectomy is indicated in
Tumor > 4 cm in diametre
Positive margin
Gross extrathyroid extension
Macroscopic multifocal disease
Macroscopic nodal metastasis
Confirmed contralateral disease
Vascular invasion

ADVANTAGE OF TOTAL THYROIDECTOMY

NECK DISSECTION IN THYROID CANCER Elective neck dissection is not performed for DTC of follicular cell
origin
Modified radical neck dissection is done for thyroid cancer when there is visible or palpable positive node
RECOMMENDATION
Central compartmental ( level VI) is recommended for all patients with clinically involved nodes
Prophylactic central neck dissection in clinically N0 patients with T3 or T4 tumors
Lateral level II to level IV should only be reserved for biopsy proven metastatic lateral cervical LAP
Level I, V, VII should only be dissected when clinically suspicious
Central and lateral neck dissection are part of standard primary therapy for all patients with sporadic and hereditary forms of medullary thyroid cancer

RADIOACTIVE IODINE THERAPY
BIOCONCENTRATION
Radioactive iodine is taken up by thyroid tissue, including DTC of follicuar epithelialOrigin at a rate 6.6 times more than most tissues of the body.


RADIOACTIVE DECAY OF IODINE-131 I-131 is produced from the fission of uranium atoms durin the operation
of nuclear reactors
I-131 decays by beta decay to Xe- 131
This first transition results in a beta particle with a range of energies from 250 to 800 KeV
Because energies of this energy range will deposit their energy within a milimeter, only the cells taking up the I-131 are affected.
In the second decay step, unstable Xe-131 decays to stable xenon, releasing photon of energy 364 KeV
This product is therapeutically undesirable, because the photon will travel far from the source where iodine is concentrated.
It contributes very little cytotoxicity to thyroid cancer cells and increases the total body dose, however it is this property that makes RAI useful for diagnostic imaging, forming the foundation for DxWBSand RxWBS.

GOALS OF RADIOACTIVE IODINE THERAPYTwo basic purposes are
a) Thyroid remnant ablation
b) Adjuvant therapy for residual microscopic disease
I. RAI provides potent cytotoxicity by targeting thyroid cancer cells remaining in the operative bed, occult LN metastasis, and distant metastasis
II. Rx WBS provides critical informatiopn including staging, prognosis, and determining which patients are likely to require additional treattments
III. Ablation of the remaining thyroid tissue facilitates the use of serum Tg as a very sensitive and specific marker for disease persistence after primary therapy

PATIENT SELECTION FOR RAI All patients with distant metastasis
Gross extrathyroidal extension of the tumour regardless of tumour size
Primary tumor size> 4 cm, even in the absence of other higher risk features
Patients with 1-4 cm thyroid tumor with high risk features LN metastasis
Age> 45 years
Intra thyroid vascular invasion
Aggressive histologic variants ( tall cell, columnar cell, or insular carcinoma
All patients with follicular and Hurthle cell variants except those with smallest unifocal FCs manifesting as only capsular invasion and without vascular invasion
Patients with persistent disease

RAI is not recommended in Unifocal PTCs< 1 cmWithout high risk featuresWhen all the foci in multifocal disease are < 1 cm Patients without residual disease or high risk histology, when post op
Tg < 1 ng/ml and anti-Tg antibodies and RAI imaging are negative

SELECTION OF I-131 ACTIVITY

FORMS AVAILABLEI131 is available in the form of
Capsule
Liquid preparation
Intravenous
Capsule is the most common used because of safety and easy of administration

PATIENT PREPARATION FOR I-131Low iodine diet -A diet that is low in iodine( <
50mcg/day) for 2 weeks before, and 2 days after I-131- Salty product to be avoided
Intravenous iodine exposure -Should be avoided- Who recieved iodine contrast within 6 months of RAI should have therapy delayed for 3-6 months and require 24 hr urinary iodine measurement
Urinary iodine measurement -Only done in patient with history of iodinated contrast exposure within 6 months- 24 hr urinary iodine on day 7 of a low iodine diet < 150 mcg/ml
rhTSH 0.9 mg im injection 2 day and 1 day before I-131 administration

Stop thyroid hormone replacement
Levothyroxine and other thyroid replacement should be withheld 6 weeks before I-131 unless rhTSH is administered in which case stop T4 and T3 3 days before and the day of I-131 administration
Lithium carbonate to increase the potency of I-131
Lithium carbonate is administered at 20mg/kg/day for 7 days beginning 5 days before I-131 administration

PRECAUTION AFTER RAI


CONTRAINDICATION

ADVERSE EFFECT OF RADIOACTIVE IODINE THERAPY


PGI PROTOCOLCriteria Low Intermediate High
Histology & Tg Non aggressive histology
Aggressive histology( tall cell, columnar & vascular invasion)
Possibly Tg out of proportion to post therapy scan
Tumour status Macroscopic tumour resectedcompletely& no microscopic invasion
Microscopic invasion Incomplete tumour resection/ macroscopic tumour invasion
Metastasis No local or distant metastasis
Cervical LN metastasis
Distant metastasis
Post therapy I131
No uptake outside thyroid bed
Uptake outside thyroid bed
Distant metastasis

Low risk: 30-50 mCiInermediate risk: 100-150 mCiHigh risk: 200 mCi

TSH SUPPRESSION FOR DIFFERENTIATED THYROID CANCERRationale- Administartion of subtherapeutic doses of T4 in an effort to
drive the TSH below detectable limits( < 0.1 Miu/L), thereby decreasing stimulation of residual benign and malignant follicular derived thyroid cells
RECOMMENDATION
TSH suppression to just below 0.1 Mu/L for high risk patients
Maintainance of TSH at or slightly below the lower limit of normal( 0.1-0.5 Mu/l) in low risk patients
LIMITATION
Subclinical and even overt thyrotoxicosis
Tachyarrhythmia
Conduction abnormalities
Ventricular hypertrophy
Systolic and diastolic dysfunction

EBRT
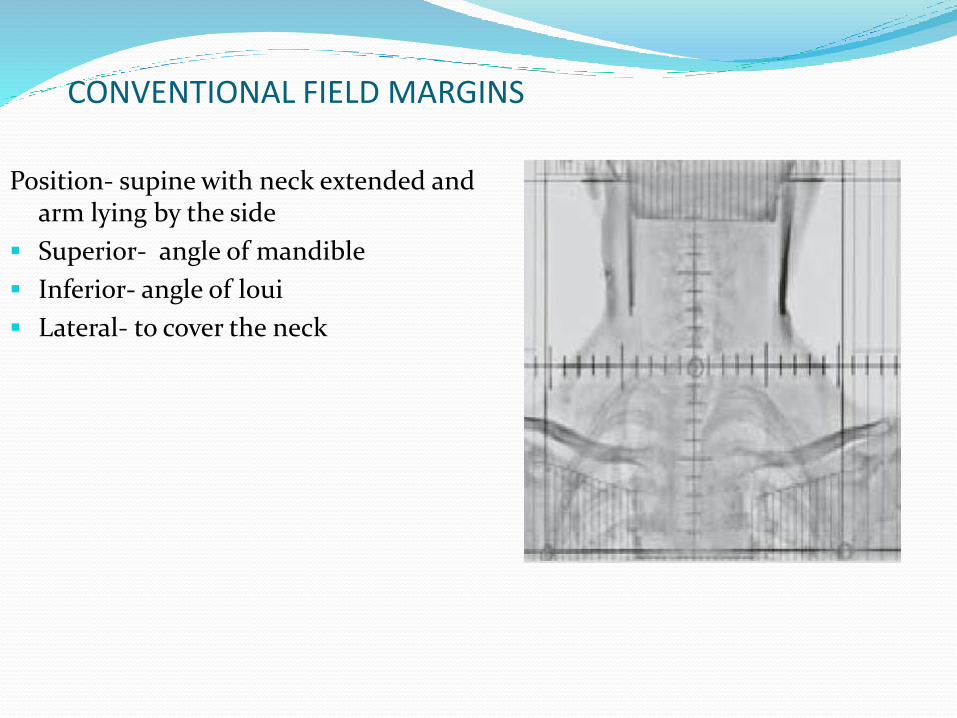
CONVENTIONAL FIELD MARGINS
Position- supine with neck extended and arm lying by the side
Superior- angle of mandible
Inferior- angle of loui
Lateral- to cover the neck

CONFORMAL RADIOTHERAPY High risk CTV: region at highest risk for residual disease
: Positive margin, ETE, LN with extracapsular extension,
gross residual disease
Standard risk CTV: Moderate risk for residual disease
Dose to high risk PTV: 66-70 Gy, 2 Gy per #
Dose to standard risk PTV: 54-56 Gy, 2 Gy per #

Contouring of high risk and standard risk PTV



TOXICITY OF EBRT
ACUTE TOXICITY LATE TOXICITY
Mucositis Fibrosis and atrophy of skin, lung apices, musculature
Taste changes Tracheal stenosis
Xerostomia Esophageal stenosis
Pharyngitis
Dysphagea
Hoarseness
Radiation dermatitis
Weight loss
Malnutrition

RESULTS OF EBRT


CHEMOTHERAPY IN DTC Systemic chemotherapy has no significant role in the management of
DTC
Poor response rate on the order of 25- 40%
The most commonly used agent is doxorubicin, either alone or in combination with cisplatin.

MANAGEMENT OF MTC All patients with MTC should be tested for RET mutation, Including
sporadic cases
Primary management of localised is total thyroidectomy, which is the only completely effective therapy
Central neck dissection should be performed in all cases
Compartment-oriented lateral neck dissection is indicated when clinically involved
No role of adjuvant RAI
INDICATION OF EBRT
CHILDREN(<18 YEARS)
Palliation of symptoms from tumors not amenable to other treatment
When tumour progression is likely to cause normal tissue damage

ADULTSTreatment of unresectable gross diseasePositive marginT4 primary tumorsNodal metastasis with extensive extracapsular extension

CHEMOTHERAPY IN MTC



MOLECULAR TARGETED AGENTS IN MTC

ROLE OF OCTREOTIDE IN MTCOctreotide is recommended to manage symptoms due to elevated
calcitonin level in medullary thyroid cancer like diarrhoea
Dose is
100-250 mcg tid sc
Octrotide LAR 20-30 mg im every 4 week

ROLE OF I131 MIBG THERAPY IN MTC MIBG( meta-iodo benzyl guanidine) is a radiopharmaceutical specific
for tumors originating from neural crest, including MTC. It is structurally similar to norepinephrine.
It is taken up actively and transported to the catecholamine storing granules of sympathomedullary tissues
INDICATION
Patients with tumour progrssion
Quality of life compromising symptoms including diarrhoea
Should be indicated when conventional therapies and chemotherapy fails
Surgical options should be excluded
Diagnostic MIBG scan should be prominent to allow successful treatment
Medications interfering with MIBG like sympathomimetics, calcium channel blockers, reserpine should be withdrawn according to biological half life.

Dose: 200-300 mCiInfusion should last 45-60 minutes to prevent acute side effectsManagement of rise of BP should be managed by alpha blockers

MANAGEMENT OF ATC Complete surgical excision should be the goal of initial therapy, when
feasible
Surgery should be avoided when complete excision is not possible as debulking does not improve outcomes
No therapeutic role for RAI
EBRT is the standard of care for palliation of local symptoms from unresectable disease or as adjuvant therapy in rare case a completely resected tumor

TREATMENT ALGORITHM

CONCLUSION Surgery is the primary treatment modality in localised thyroid cancer
of all histologies.
Total thyroidectomy is preferred surgical procedure in most cases.
LN dissection is indicated when clinically involved except MTC where level VI is indicated in all cases.
In DTC, RAI is indicated in patients with distant metastasis or high risk histopathological features
EBRT is indicated in DTC when there is gross residual tumor or gross ETE which is not amenable for surgery or RAI.
EBRT is the standard of care for palliation of symptoms in ATC.


![Thyroid Cancer and Thyroid Nodules.ppt [Read-Only] · Thyroid CaThyroid Ca 20012001. Newer Exceptions Unfortunately recent Studies have shown exceptions: *** *** In one study of papillary](https://img.pdfslide.net/doc/110x75/5d4794b388c9931b4f8b7654/thyroid-cancer-and-thyroid-read-only-thyroid-cathyroid-ca-20012001-newer.jpg)