Embed Size (px)
Citation preview
Transplant immunity
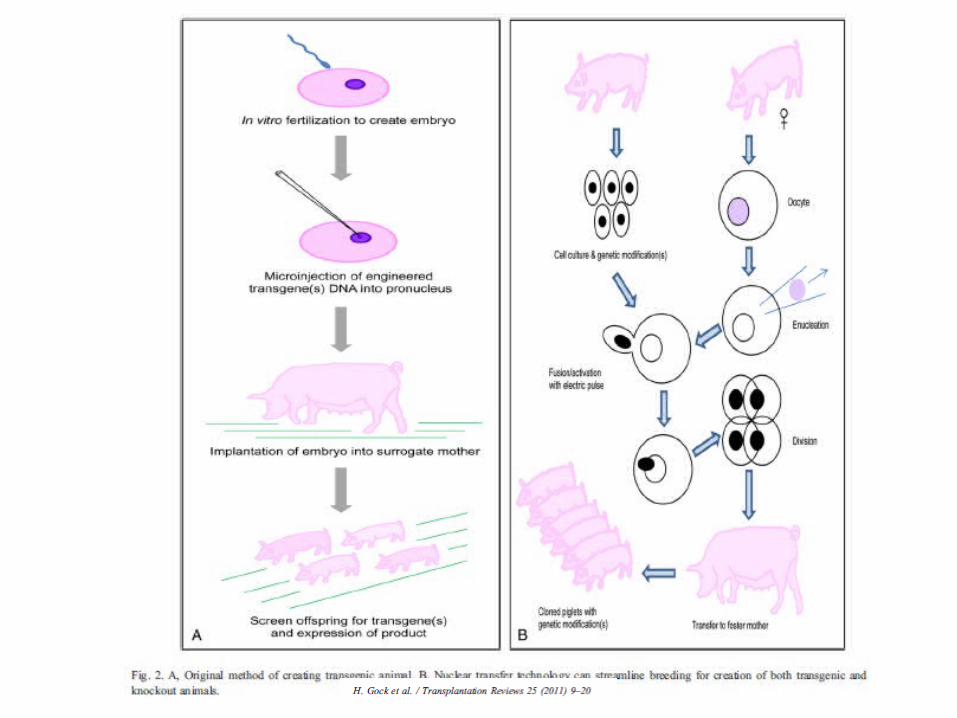
From mythology to transgenic world….
Outline • Introduction & Terminology
• History
• Types of rejection
• Immunologic Basis
• Effector mechanisms of allograft rejection
• Laboratory work up
• Immunosuppressive therapy
• Individual transplants
• Organ donation
• Future prospects
Introduction • Transplantation is one of mankind’s ancient dreams as it
is potentially curative treatment for end stage organ failure.
• Problem? … Achieving the clinical tolerance – in allograft/ xenograft
• Main focus is on identifying the causes and approaches to combat rejection for better survival– i e by recipient Immunosuppression
• Infections, Malignancy are important complications
• Shortage of organs to the current demand and ethical issues
Terminology
• Donor and recipient
• Alloantigen and alloantibody
• MHC or HLA
Epidemiology
• Global Database on Donation and Transplantation gathering data from 97 countries, in 2007 around
• 100,000 solid organ transplantations were performed per
year worldwide: • 68,250 are kidney transplantations (45% from living donors), • 19,850 are liver transplantations (14% from living donors), • 5,179 are heart transplantations, • 3,245 are lung transplantations, and • 2,797 are pancreas transplantations.
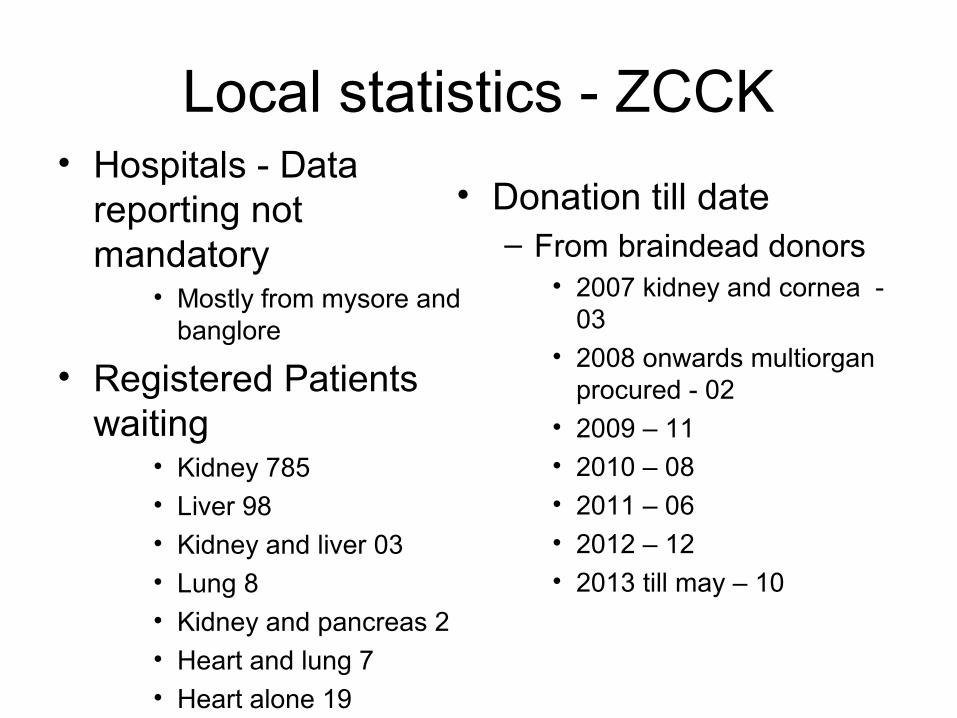
Local statistics - ZCCK• Hospitals - Data
reporting not mandatory
• Mostly from mysore and banglore
• Registered Patients waiting
• Kidney 785• Liver 98• Kidney and liver 03• Lung 8• Kidney and pancreas 2• Heart and lung 7
• Heart alone 19
• Donation till date– From braindead donors
• 2007 kidney and cornea - 03
• 2008 onwards multiorgan procured - 02
• 2009 – 11• 2010 – 08 • 2011 – 06 • 2012 – 12 • 2013 till may – 10
Classification
• Based on organs transplanted
• Autograft, Isograft, Allograft, Xenograft
• Orthotopic vs heterotopic
• Fresh or stored
• Living or dead tissue
History
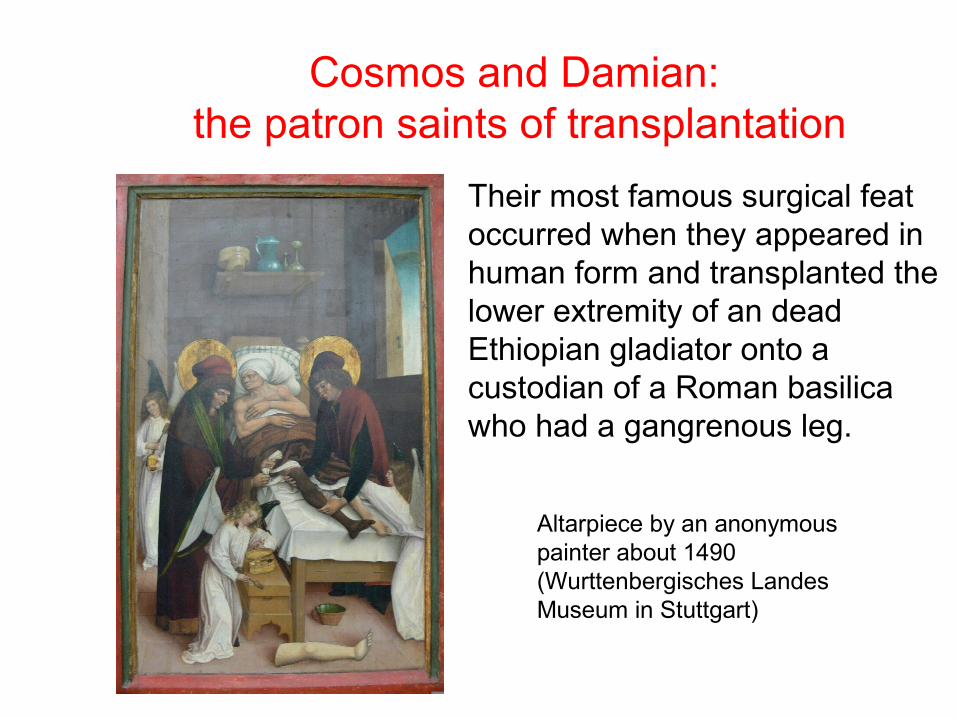
Cosmos and Damian: the patron saints of transplantation
Their most famous surgical feat occurred when they appeared in human form and transplanted the lower extremity of an dead Ethiopian gladiator onto a custodian of a Roman basilica who had a gangrenous leg.
Altarpiece by an anonymous painter about 1490 (Wurttenbergisches Landes Museum in Stuttgart)
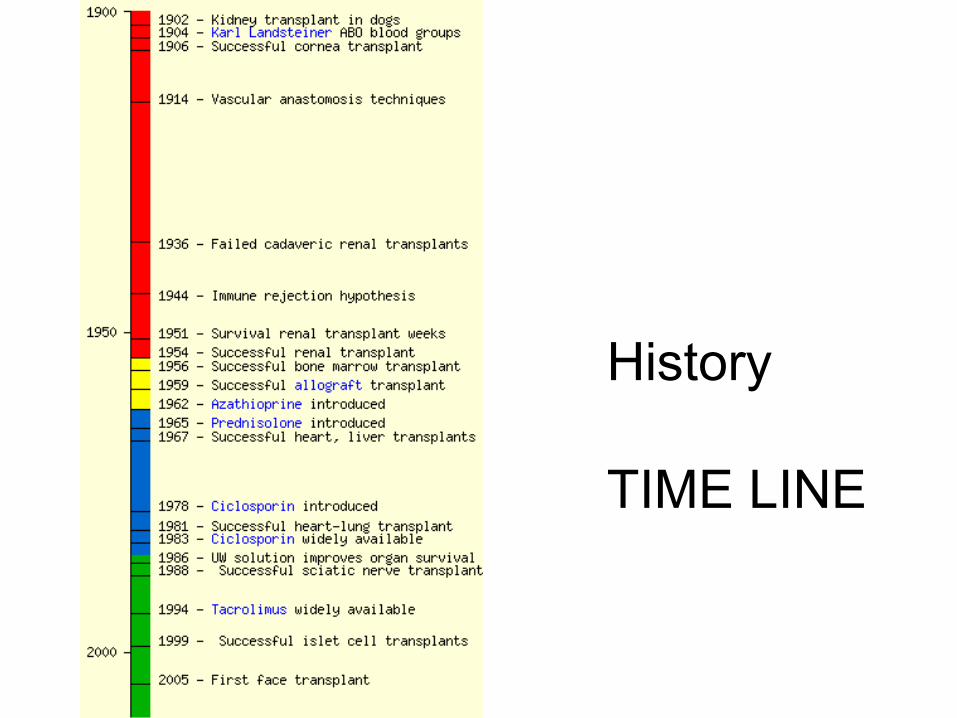
History
TIME LINE
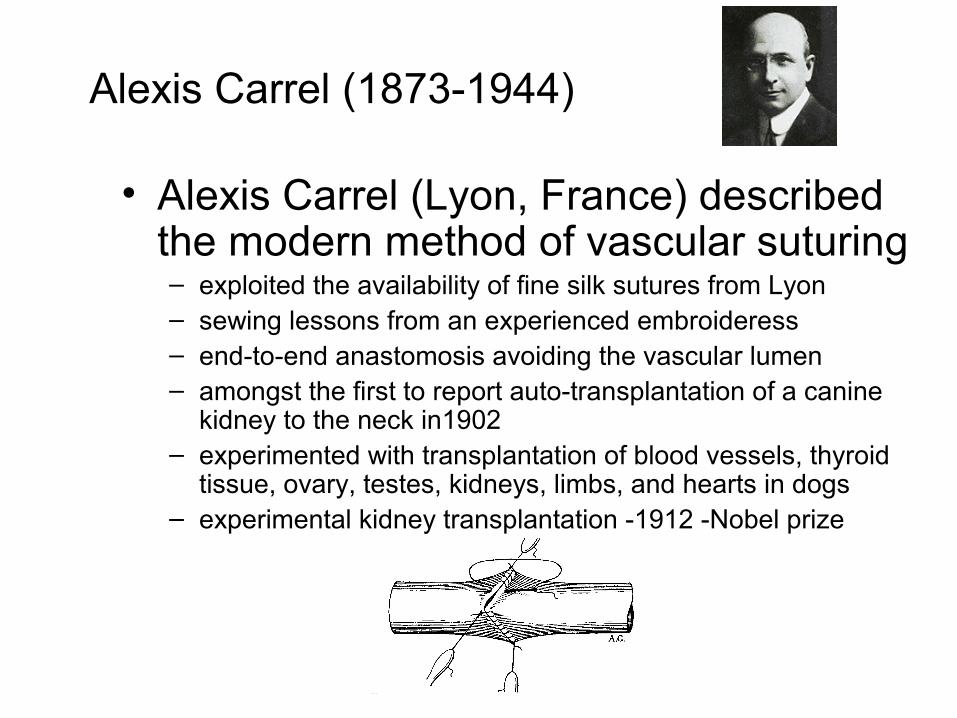
Alexis Carrel (1873-1944)
• Alexis Carrel (Lyon, France) described the modern method of vascular suturing– exploited the availability of fine silk sutures from Lyon– sewing lessons from an experienced embroideress– end-to-end anastomosis avoiding the vascular lumen– amongst the first to report auto-transplantation of a canine
kidney to the neck in1902– experimented with transplantation of blood vessels, thyroid
tissue, ovary, testes, kidneys, limbs, and hearts in dogs– experimental kidney transplantation -1912 -Nobel prize
Alexis CarrelThe Nobel Prize in Physiology or Medicine 1912 was awarded to Alexis Carrel "in recognition of his work on vascular suture and the transplantation of blood vessels and organs".
The immunological barrier
How is it that Rejection immune related?
Karl Landsteiner
The Nobel Prize in Physiology or Medicine 1930 was awarded
"for his discovery of human blood groups".
Blood Relations
http://www.nobelprize.org/nobel_prizes/medicine/laureates/1980/speedread.html
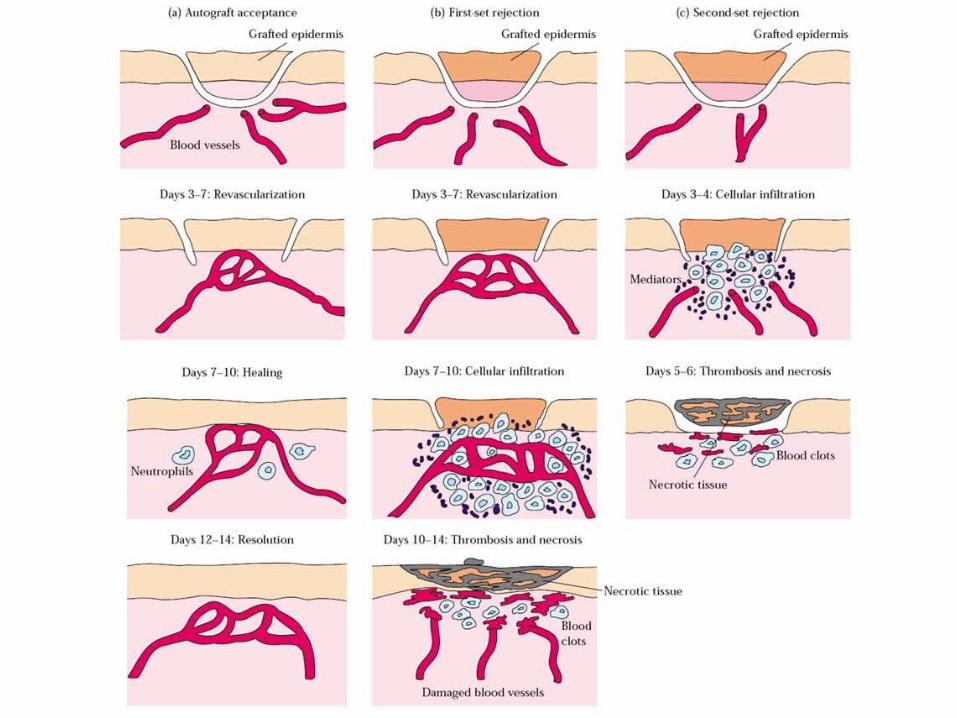
Transplantation History• P.B. Medawar (1945) skin grafts
– Self skin accepted– Relative not accepted
REJECTION is a Immunologic phenomenon
• A. Mitchison (1950)– Lymphocytes are responsible for rejection
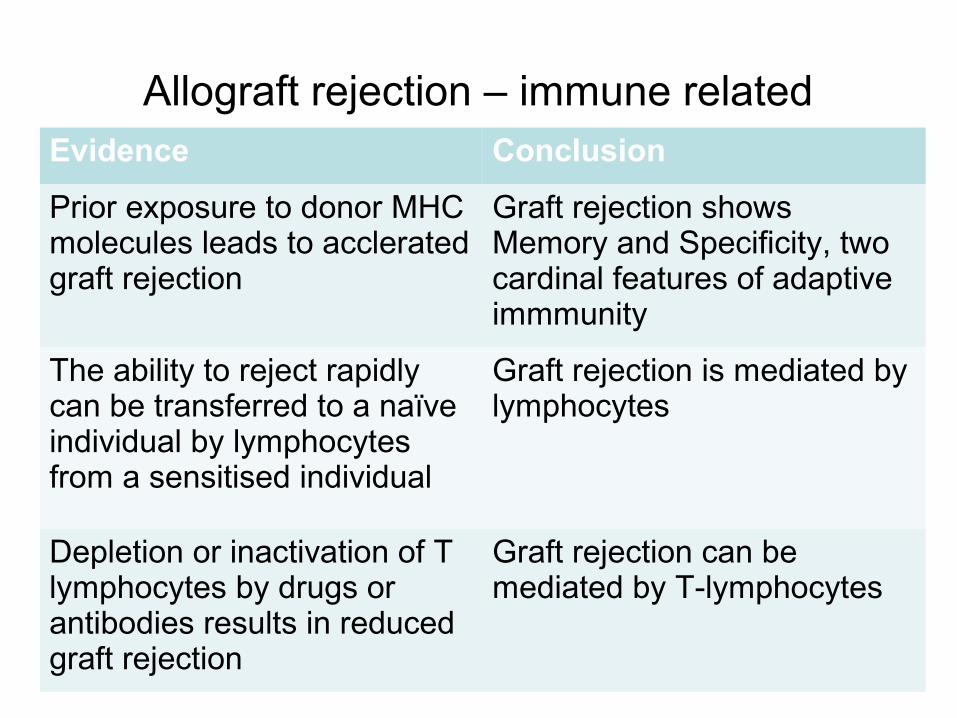
Allograft rejection – immune relatedEvidence Conclusion
Prior exposure to donor MHC molecules leads to acclerated graft rejection
Graft rejection shows Memory and Specificity, two cardinal features of adaptive immmunity
The ability to reject rapidly can be transferred to a naïve individual by lymphocytes from a sensitised individual
Graft rejection is mediated by lymphocytes
Depletion or inactivation of T lymphocytes by drugs or antibodies results in reduced graft rejection
Graft rejection can be mediated by T-lymphocytes
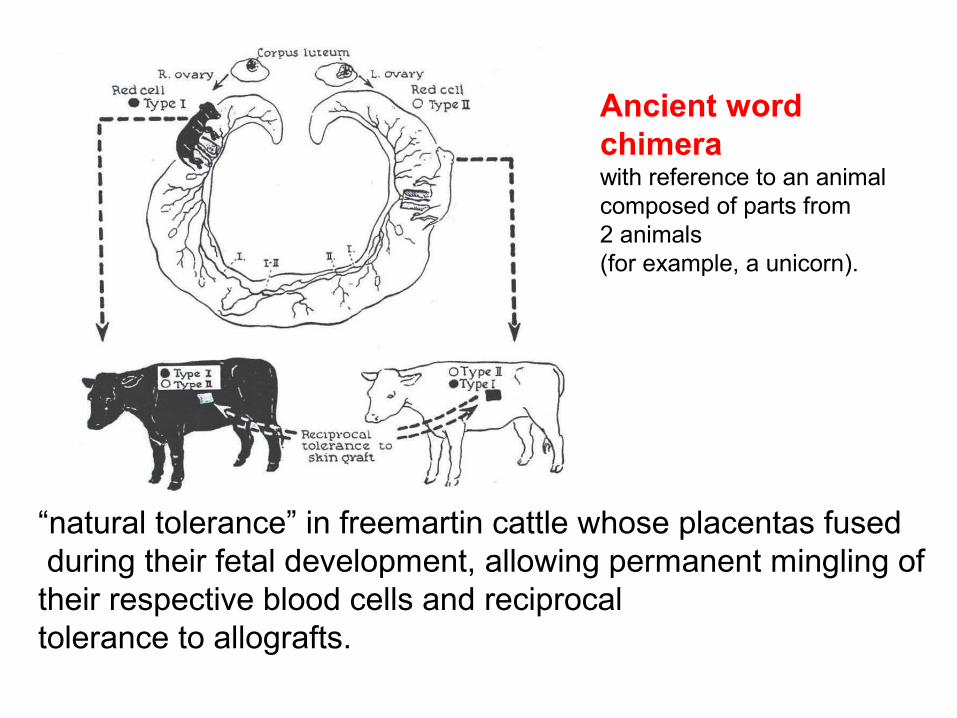
Ancient word chimera with reference to an animal composed of parts from 2 animals (for example, a unicorn).
“natural tolerance” in freemartin cattle whose placentas fused during their fetal development, allowing permanent mingling of their respective blood cells and reciprocal tolerance to allografts.
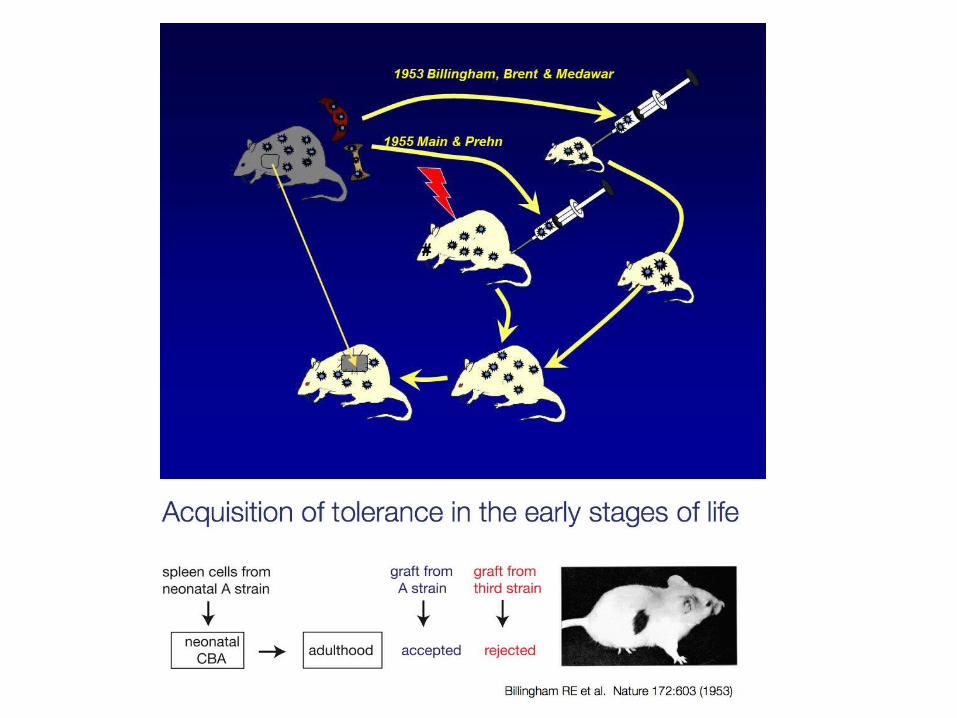
Sir Frank Macfarlane Burnet Peter Brian Medawar
The Nobel Prize in Physiology or Medicine 1960 was awarded jointly
"for discovery of acquired immunological tolerance"
Raising Self-Awareness
http://www.nobelprize.org/nobel_prizes/medicine/laureates/1980/speedread.html
What is the MOLECULAR basis of acceptance/rejection?
In other words
reason for compatibility or incompatibility?
Major proteins that mediate Histoincompatibility found
• Peter Gorer (~1935)
• Gorer and Gorge Snell (~1950)– Narrowed it down to locus causing tumour
REJECTION in inbred Mice experiments– Same could be applied to transplant rejection – H2 antigens are responsible for rejection– Later identified –not one gene ..but set of closely
linked genes which are transferred vertically with recombination as Haplotype
MHC - discovery
• Dausset – • uncovered the first compatibility antigen in humans. • He noticed that a patient receiving several transfusions of ABO
compatible blood still suffered an unexpected immune reaction.
• Dausset discovered that in this case antibodies were being launched against white blood cells belonging to the donor only, and that these antibodies in the patient’s serum triggered a similar reaction in half the samples of white blood cells taken from other people.
• He called the factor responsible MAC, and this turned out to be the first of a series of human leukocyte antigens, or HLAs.
• Now it has became clear that the HLA region constituted the human version of the MHC, and that the HLA genes are so variable and yet so specific for an individual that this provides a form of fingerprint at the cellular level.
MHC - discovery
• Benacerraf – • first indication that immune reactions are controlled by
genes. • was surprised to discover that different strains of
guinea pigs launched different levels of attack towards the same foreign antigen, and he traced the cause to what he termed immune response genes.
• Over the years, many of these immune response genes have been found and traced to the same location, all being members of a previously undiscovered cluster of genes lying within the MHC.
Baruj Benacerraf Jean Dausset George D. Snell
The Nobel Prize in Physiology or Medicine 1980
"for their discoveries concerning genetically determined structures on the cell surface that regulate immunological reactions".
Seeking Signs of Compatibility
What is function of MHC/HLA?
As allograft rejection is iatrogenic effect and not biological
phenomenon
MHC / HLA
• Immune defences must take extreme care not to avoid harming any cells belonging to its own host.
• Achieving this requires a sophisticated self-identification system, and this is centred on a collection of genes called the major histocompatibility complex, or MHC, which encode proteins known collectively as histocompatibility antigens.
• Each individual carries a unique combination of these antigens on the surface of their cells, providing a form of biological ID system for distinguishing one individual from another.
MHC / HLA
• The MHC-system provides an extraordinarily sensitive surveillance system to detect cells with changed membranes.
• It also provides a mechanism to kill cells that are becoming alienated from their community in one way or another.
• The rejection of foreign grafts is then merely an unavoidable by product.
Double-Checking Cells
Unmasked the true purpose of these self-recognition protein molecules,
the major histocompatibility antigens
Peter C. Doherty M. Zinkernagel
The Nobel Prize in Physiology or Medicine 1996 was awarded jointly
"for their discoveries concerning the specificity of the cell mediated immune defence"

Successful transplant in identical twins
Joseph E. Murray E. Donnall Thomas
The Nobel Prize in Physiology or Medicine 1990 was awarded jointly to Joseph E. Murray and E. Donnall Thomas "for their discoveries concerning organ and cell transplantation in the treatment of human disease“
1954 Succesful kidney transplant between identical twins in Boston – Peter Bent Brigham Hospital
Eichwald – Silmser effect
• Highly inbred strain of animals– Female to male transplant successful– Male to female transplant rejected
As XY cells would have antigens expressed by Y chromosome
Successful transplant in unrelated donor & recipient
Immunosuppressants
• Corticosteroids – Goodwin and Mims 1963 reported that they had used
corticosteroids to reverse acute rejection in a living-donor kidney transplant recipient. Starzl and Marchioro, in 1963, confirmed the efficacy with corticosteroids and the “almost miracle” effect.
• Azathioprine / Imuran– Dr Dameshake and Dr Schwartz hypothesis if antimetabolites could be used for
treating leukemia – same could be used for immunosuppression – transplant– Dr Calne used successfully in dog kidney transplants
http://cjasn.asnjournals.org/content/1/5/907.full
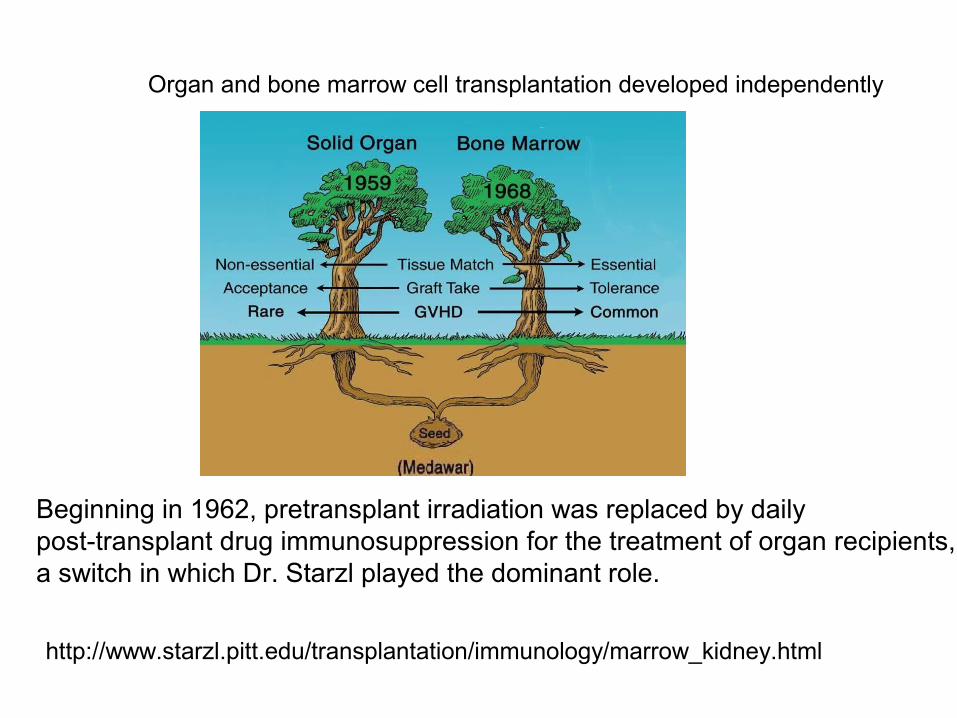
Organ and bone marrow cell transplantation developed independently
Beginning in 1962, pretransplant irradiation was replaced by daily post-transplant drug immunosuppression for the treatment of organ recipients, a switch in which Dr. Starzl played the dominant role.
http://www.starzl.pitt.edu/transplantation/immunology/marrow_kidney.html

Privileged sites
• Cornea - avascular
• Cartilage
Natural Allograft • Fetus from Paternal antigens
– Protection from attack through• Physical barrier, hCG- nonspecific immune
suppression, antigen masking by neg charged muco polysaccharide,
• downregulation of classical MHC class I antigen expression on trophoblast cells, which form the external epithelial layer of the placenta,
• and maintenance of an immunologically favorable immunosuppressive environment in the uterus.
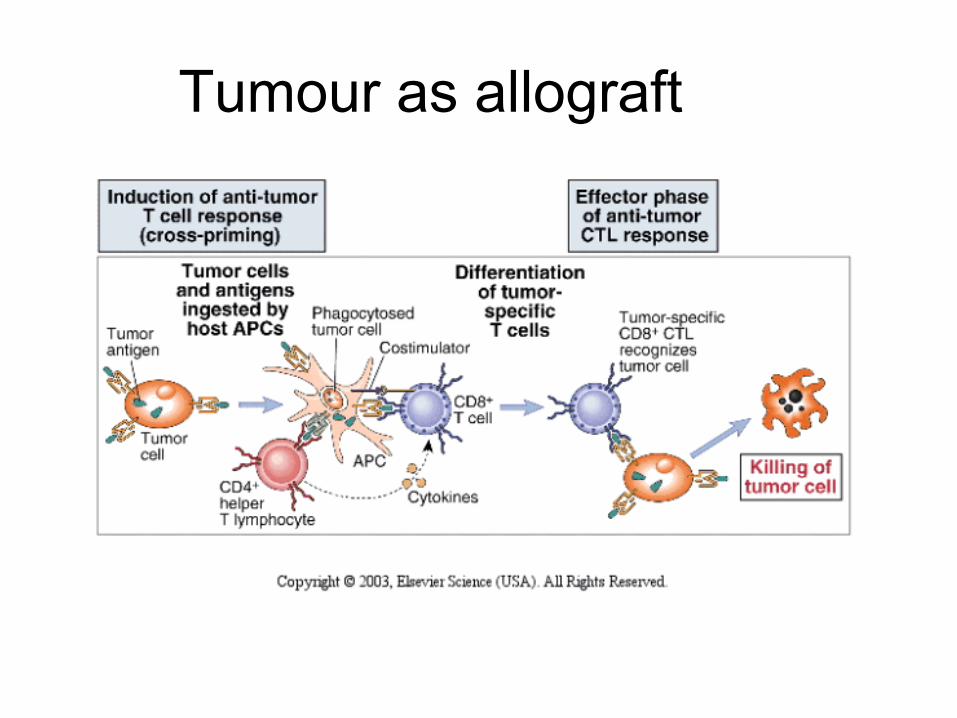
Tumour as allograft
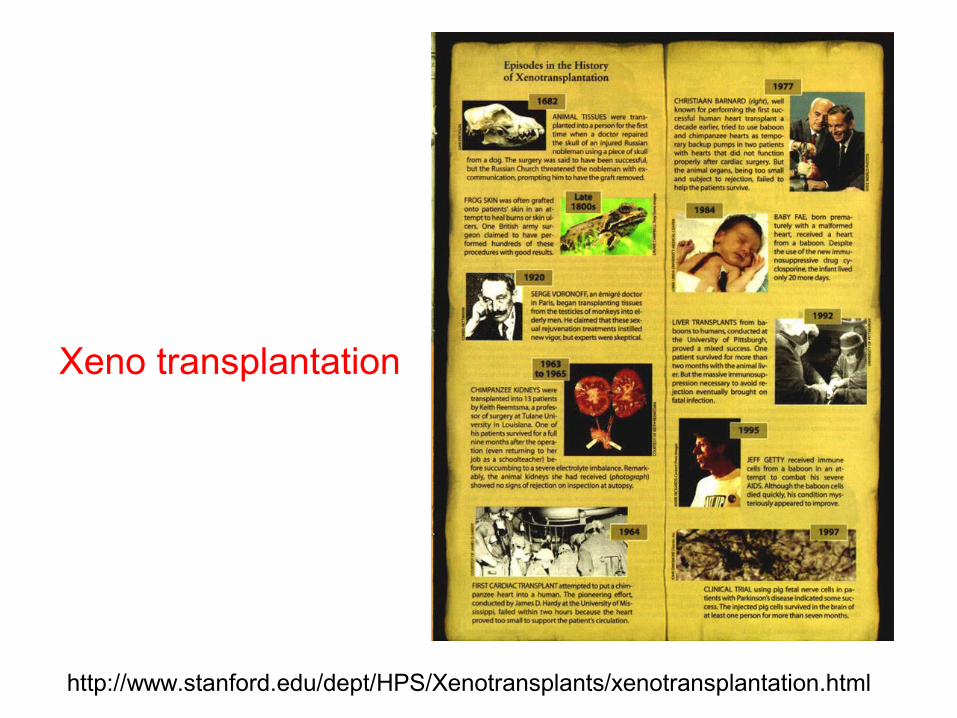
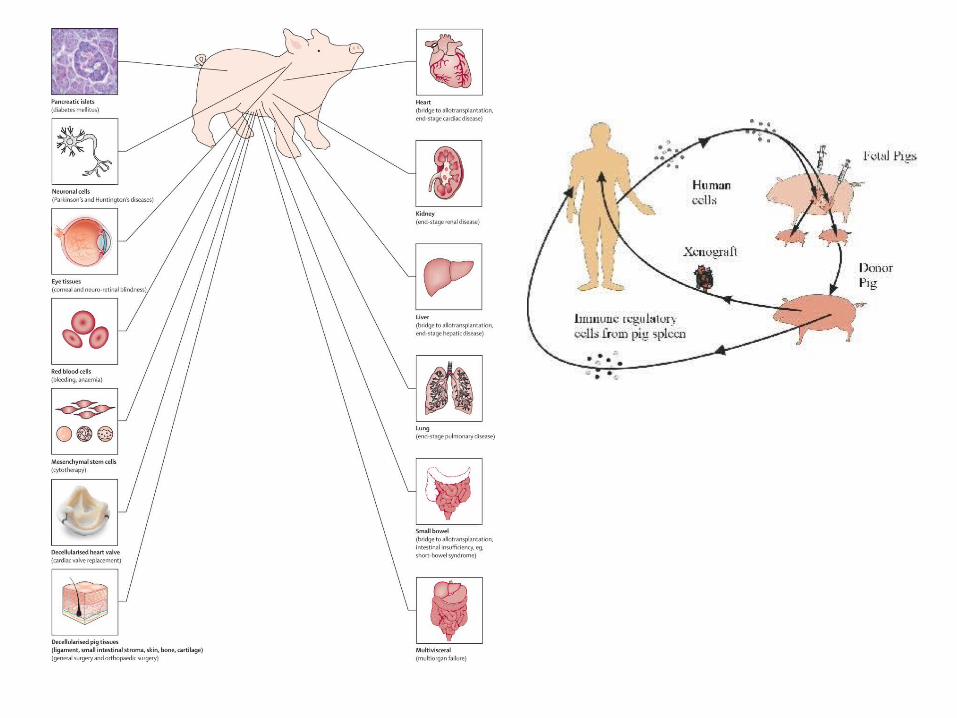
http://www.stanford.edu/dept/HPS/Xenotransplants/xenotransplantation.html
Xeno transplantation
Allograft rejection
Immunologic basis
Immunologic basis
• MHC / HLA role
• What Immune cells are involved?
• Immune response against alloantigens– Direct and indirect antigen presentation
Immune cells involved
• The roles of the different components of the immune system involved in the tolerance or rejection of grafts and in graft-versus-host disease have been clarified.
• These components include:
• antibodies,
• antigen presenting cells,
• helper and cytotoxic T cell subsets, • And
– immune cell surface molecules, MHC - TCR– signaling mechanisms and– cytokines that they release.
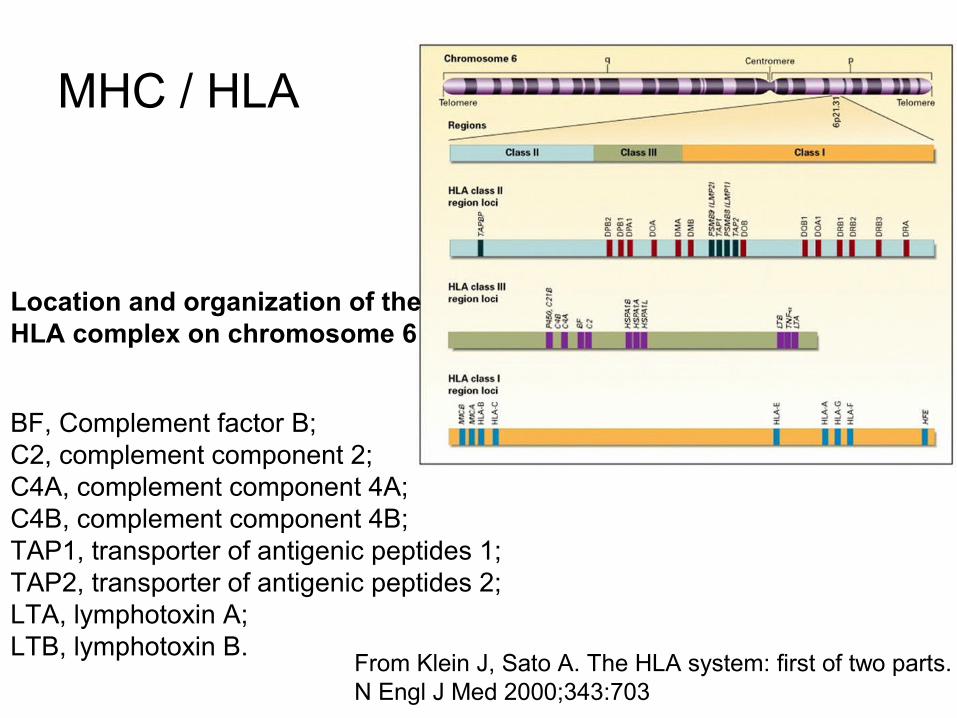
MHC / HLA
Location and organization of the HLA complex on chromosome 6
BF, Complement factor B; C2, complement component 2; C4A, complement component 4A; C4B, complement component 4B; TAP1, transporter of antigenic peptides 1; TAP2, transporter of antigenic peptides 2; LTA, lymphotoxin A; LTB, lymphotoxin B.
From Klein J, Sato A. The HLA system: first of two parts.N Engl J Med 2000;343:703
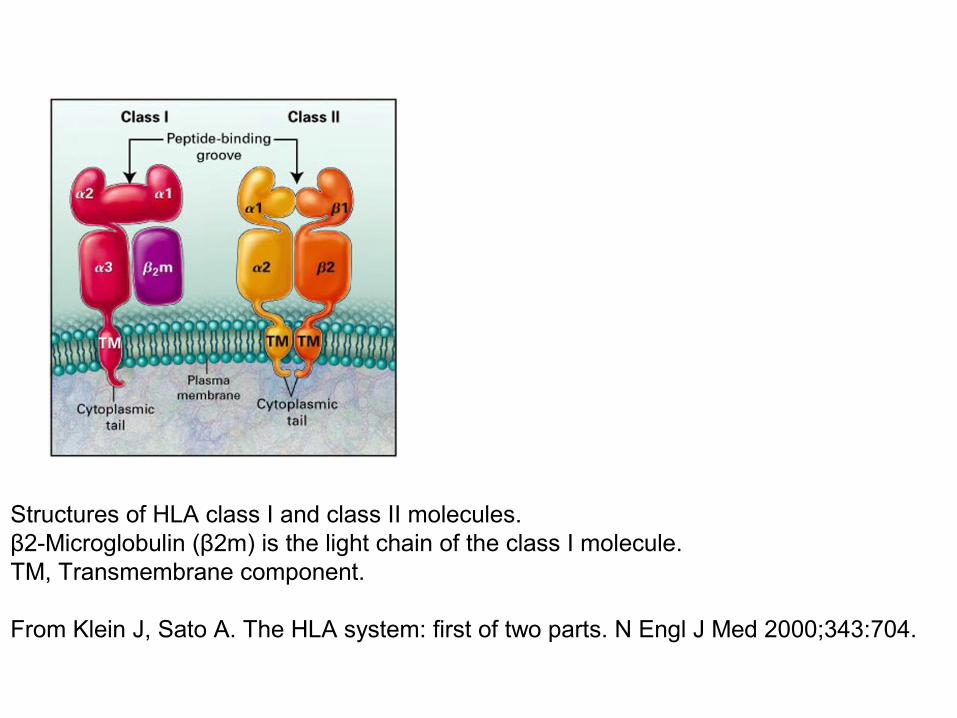
Structures of HLA class I and class II molecules. β2-Microglobulin (β2m) is the light chain of the class I molecule. TM, Transmembrane component.
From Klein J, Sato A. The HLA system: first of two parts. N Engl J Med 2000;343:704.
Major histocompatibility antigens• Cell fingerprint UNIQUE for an individual
• MHC loci are highly polymorphic
• The loci are closely linked to each other, a set of alleles is called a HAPLOTYPE
• So one inherites a haplotype from mother and another from father
• The alleles are codominantly expressed
HLA Polymorphism
• HLA – A 350 alleles
• HLA – B 620 alleles• HLA – DR 400 alleles• HLA – DQ 90 alleles
• RESULT?
– No two individuals in an outbred population have exactly the same set of MHC genes and molecules
Induction of Immune Responses Against Transplants
• alloantigens and xenoantigens:
– graft derived antigens that serve as the targets of rejection
• the antibodies and T cells that react against these antigens are said to be alloreactive and xenoreactive,
respectively.
• allorecognition– direct
– indirect
The Immunology of Allogeneic Transplantation
• Recognition of transplanted cells that are self or foreign is determined by polymorphic genes (MHC) that are inherited from both parents and are expressed co-dominantly.
• Alloantigens elicit both cell-mediated and humoral immune responses.
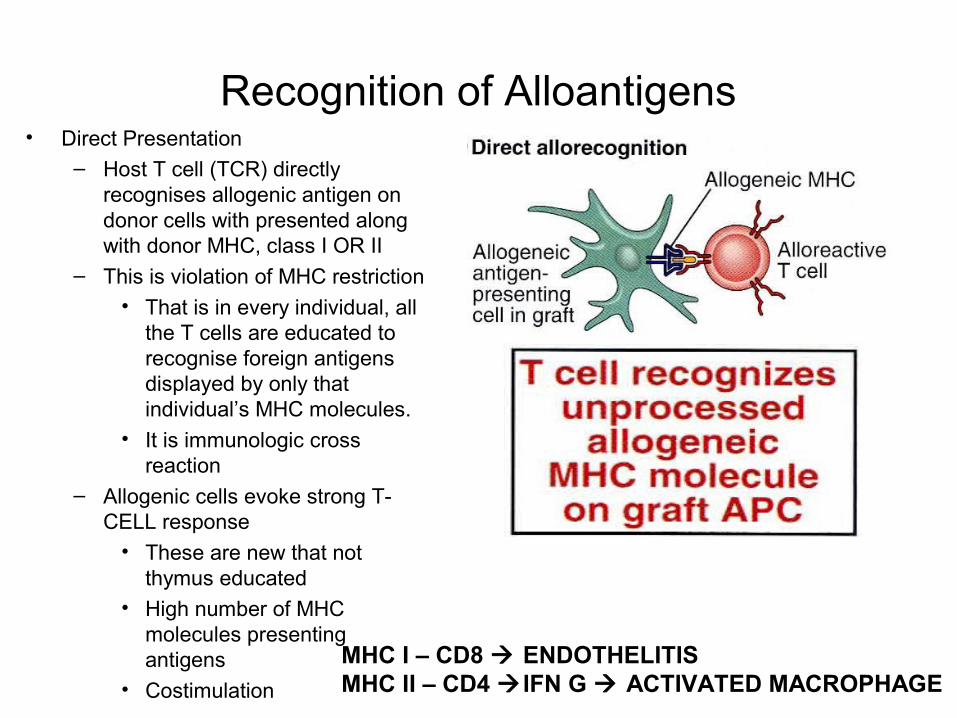
Recognition of Alloantigens• Direct Presentation
– Host T cell (TCR) directly recognises allogenic antigen on donor cells with presented along with donor MHC, class I OR II
– This is violation of MHC restriction• That is in every individual, all
the T cells are educated to recognise foreign antigens displayed by only that individual’s MHC molecules.
• It is immunologic cross reaction
– Allogenic cells evoke strong T-CELL response
• These are new that not thymus educated
• High number of MHC molecules presenting antigens
• Costimulation
• .
MHC I – CD8 ENDOTHELITISMHC II – CD4 IFN G ACTIVATED MACROPHAGE
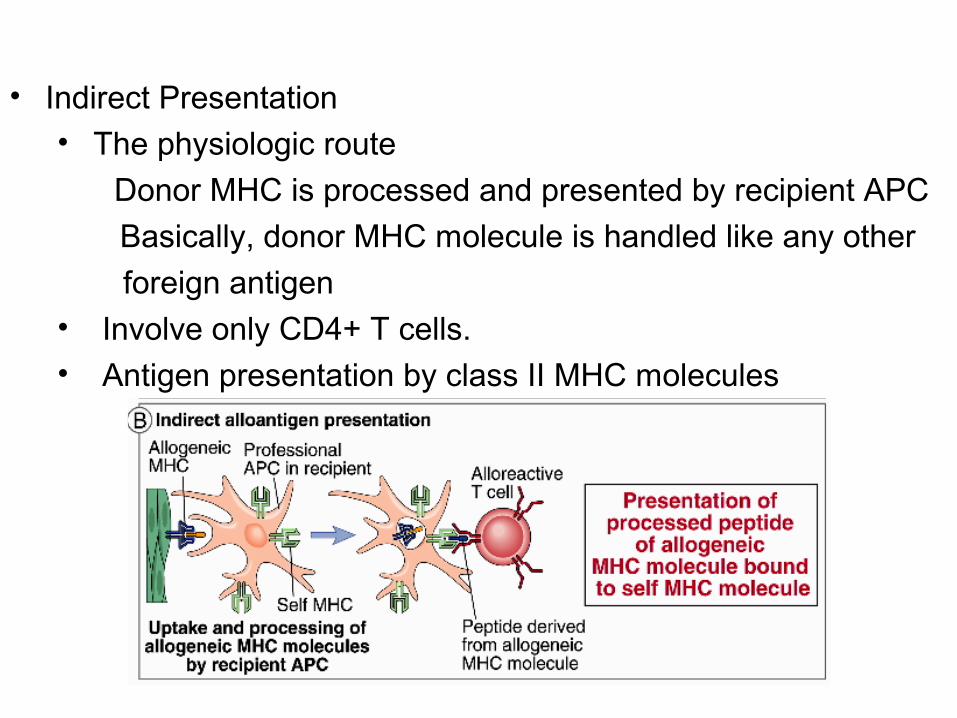
• Indirect Presentation• The physiologic route
Donor MHC is processed and presented by recipient APC
Basically, donor MHC molecule is handled like any other
foreign antigen• Involve only CD4+ T cells.• Antigen presentation by class II MHC molecules
Role of Cytokines in Graft Rejection
IL – 2, IFN – γ, and TNF - β
…are important mediators of graft rejection.
• IL – 2 promotes T-cell proliferation and generation of T – Lymphocytes.
• IFN - γ is central to the development of DTH response.
• TNF - β has direct cytotoxic effect on the cells of graft.
Role of Cytokines in Graft Rejection
• A number of cytokines promote graft rejection by inducing expression of class – I or class – II MHC molecule on graft cell.
• The interferon (α, β and γ), TNF – α and TNF - β all increases class – I MHC expression, and IFN - γ increases class – II MHC expression as well.
Effector Mechanisms of Allograft Rejection
• T cell mediated
– CTL’s kill graft cells parenchymal, endothelial celldeath
• Thrombosis ischemia
– helper T cell’s IFN g DTH reaction
• Increased vascular permeability, local accumulation of lymphocytes and macrophages
• Activated macrophage injures graftcell, vasculature ishemia
• Antibody mediated rejection – Alloantibody + graft
endothelium+ complement injury, 2ndary thrombosis
• Adding fuel to the fire are platelet aggregation, coagulation
• C4d deposit histopathological diagnosis
– Hyperacute rejection
Clinical presentation
Hyperacute Rejection
Acute Rejection
Chronic Rejection
Hyperacute Rejection• White graft response
• Graft remains pale and is rejected within hours, without even an attempt at vascularisation
• Characterized by • thrombotic occlusion of the graft, Begins within minutes or hours
after anastamosis, • Pre-existing antibodies in the host circulation bind to donor
endothelial antigens, • Activates Complement Cascade
• Seen in Xenografts, ABO incompatibility or prior blood transfusions or pregnancies ..sensitisation
• Avoided by blood typing and cross matching ie for Ab’s against the cells of potential donor
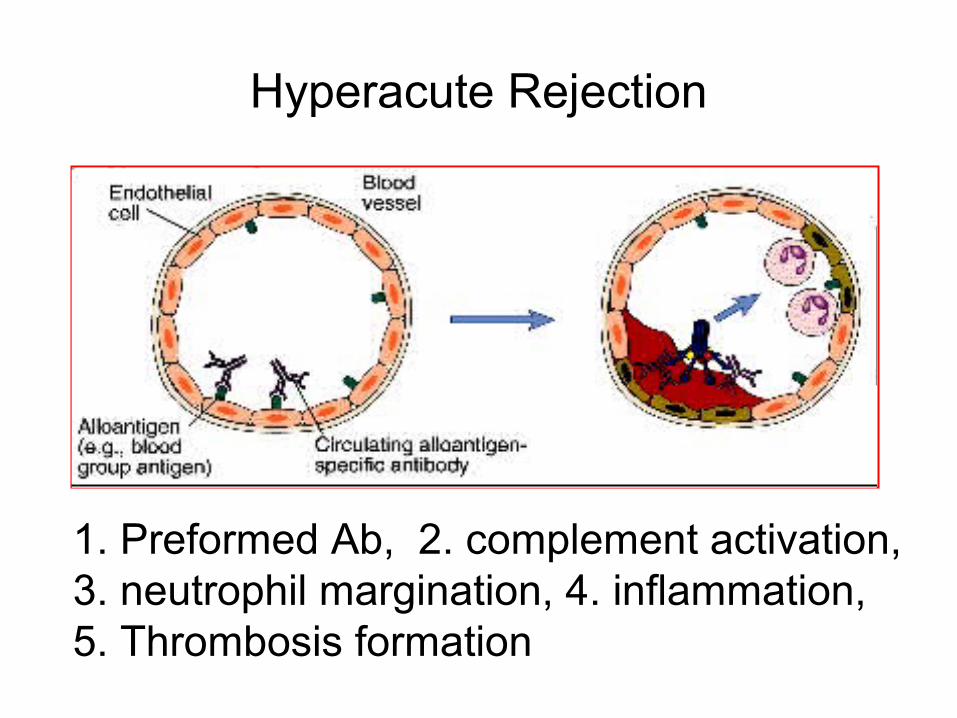
Hyperacute Rejection
1. Preformed Ab, 2. complement activation, 3. neutrophil margination, 4. inflammation, 5. Thrombosis formation
Acute Rejection
• Vascular and parenchymal injury mediated mainly by CTL cells and antibodies
• usually begin after the first week of transplantation if there is no immunosuppressant therapy
• Incidence is high (30%) for the first 90 days
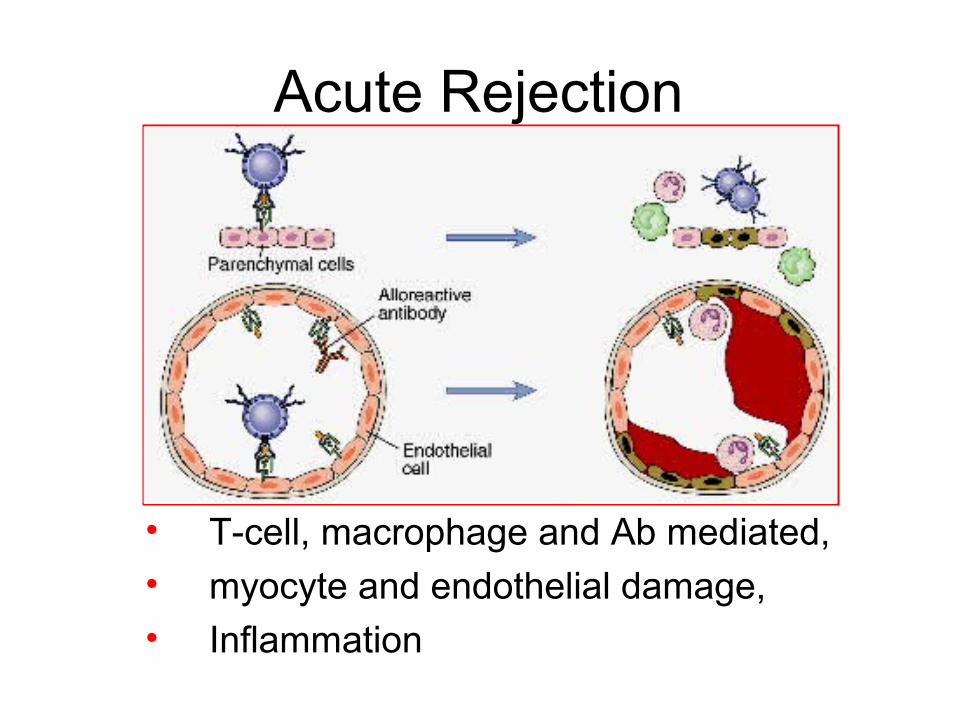
Acute Rejection
• T-cell, macrophage and Ab mediated,• myocyte and endothelial damage, • Inflammation
Chronic Rejection
• Indolent form occurs over mths to years
• Emerged as Important cause of graft loss compared to acute cause which has definite treatment
• Occurs in most solid organ transplants» Heart, Kidney, Lung, Liver
• Characterized by fibrosis and vascular abnormalities with progressive loss of graft function over a prolonged period.
• Arteriosclerosis – gradual narrowing of vessels • Mediated by Tcell cytokines
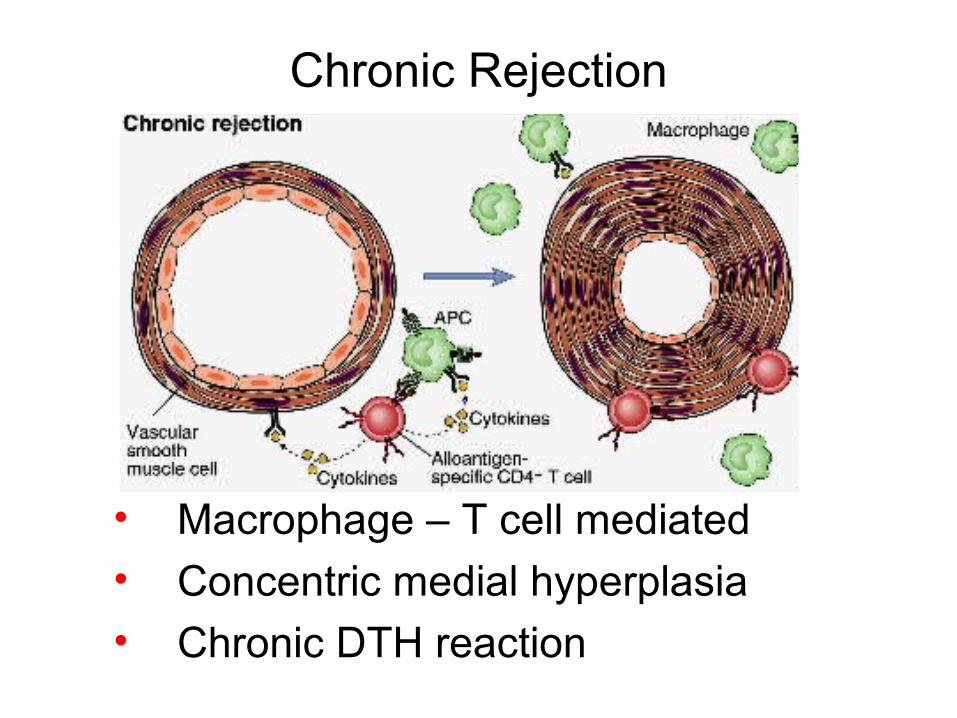
Chronic Rejection
• Macrophage – T cell mediated
• Concentric medial hyperplasia
• Chronic DTH reaction
Transplantation of hematopoietic cells
• Rejection by host T cells resistant to radiotherapy/chemothearapy
• Two problems comlplicate this form of transplant – GVH & immunodeficiency
• Immunodeficiency due to slow reconstitution of host immune system & inability to fully generate all necessary immune cells susceptible to infections mostly viral as CMV, EBV.
Graft vs. Host Disease
• In bone marrow transplantation and lymphoid rich organs like liver– Caused by the reaction of grafted mature T-cells in the marrow
inoculum with alloantigens of the host and recognise host as foreign
– Activation of CD4 & CD8 cells DTH & CTL responces – Due to Mismatch between minor HLA
• Acute GVHD Days-weeks– Characterized by epithelial cell death in the skin, GI tract, and
liver– Bloody diarrhea, jaundice, rash
• Chronic GVHD may follow acute syndrome or occur insidiously– Mimick autoimmune disorders like SLE– Characterized by atrophy and fibrosis of one or more of these
same target organs as well as the lungs
Graft vs. Host Disease
• Lethal complication • combination of methotrexate, corticosteroids and a calcineurin
inhibitor daily for 6 months.– When GVHD becomes established, it is extremely difficult to
treat. Anti-thymocyte serum, steroids, cyclosporine, tacrolimus, anti–IL-2R α chain antibodies, anti-TNF α inhibitors, mycophenolate mofetil, and murine monoclonal antibodies to human T-cell surface antigens
• Prevention strategy– Minimised by HLA matching but not eliminated– Donor T cell depletion before transplant– Mixed blessing
• Risk of GVHD reduced but incidence of graft failure and recurrence of leukemia increase
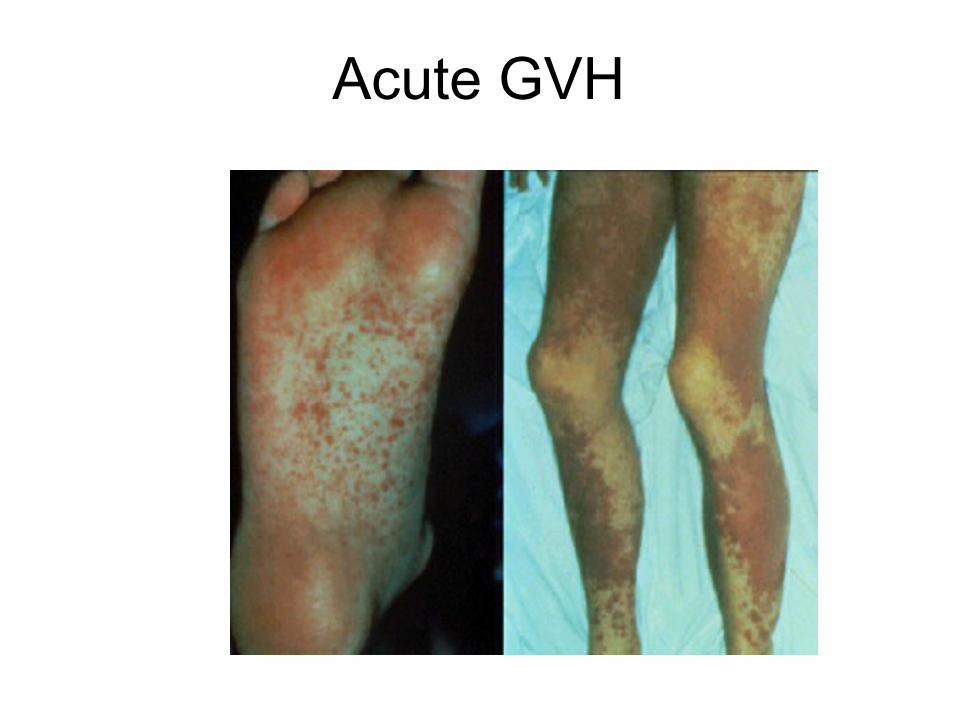
Acute GVH
Laboratory
Factors favoring allograft survival ..Rejection Prevention
• Since difference in blood group and major histocompatibility antigens are responsible for the most intense graft rejection reactions.
– Blood grouping: – HLA typing– Tissue matching
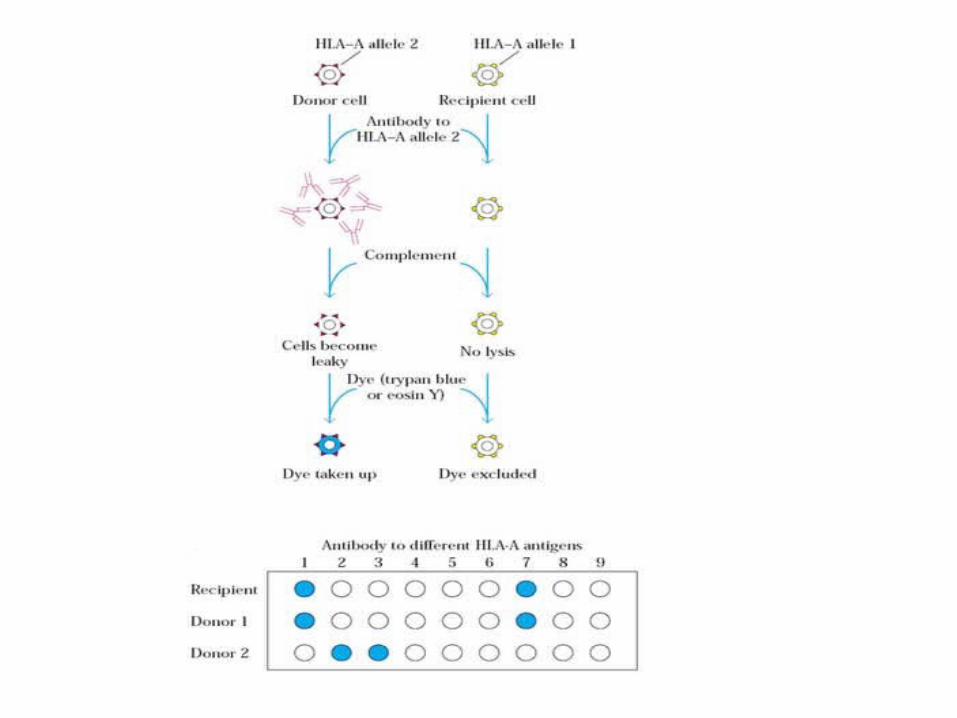
HLA TISSUE typing of potential donors and a recipient
• Microcytotoxicity test for HLA antigens –
– white blood cells from the potential donors and recipient are distributed into a series of wells on a microtiter plate,
– MULTIPAROUS WOMEN/ MONOCLONAL antibodies specific for various class I and class II MHC alleles are added to different wells.
– After incubation, complement is added to the wells, and cytotoxicity is assessed by the uptake or exclusion of various dyes (e.g., trypan blue or eosin Y) by the cells.
– If the white blood cells express the MHC allele for which a particular monoclonal antibody is specific, then the cells will be lysed upon addition of complement, and these dead cells will take up a dye such as trypan blue. – INVERTED MICROSCOPE
– indicate the presence or absence of various MHC alleles. It is not possible to get 100% compatible individuals.
Tissue matching:
• Tissue matching was tested with the help of
– Mixed Lymphocyte Reactions (MLR) is an invitro system for assaying TH cell proliferation in a cell mediated response
– Cell Mediated Lympholysis (CML) is an invitro assay of effector cytotoxic function.
Mixed Lymphocyte Reactions/culture
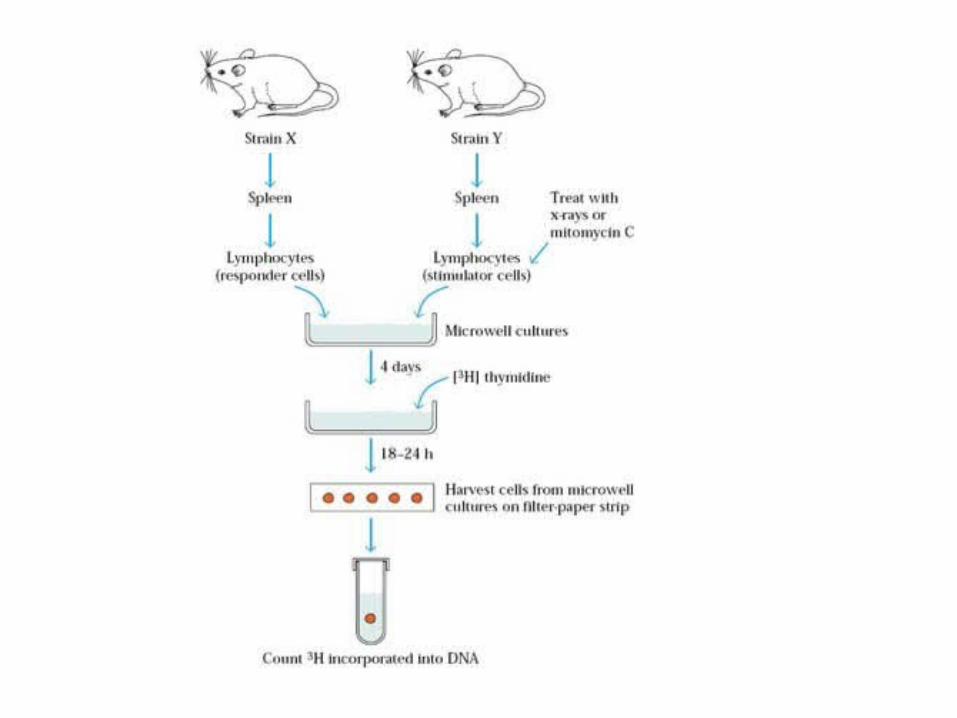
• A one-way mixed-lymphocyte reaction (MLR) can be used to quantify the degree of class II MHC compatibility between potential donors and a recipient.
• Lymphocytes from a potential donor that have been x-irradiated or treated with mitomycin C serve as the stimulator cells, and lymphocytes from the recipient serve as responder cells.
• Proliferation of the recipient T cells, which indicates T-cell activation, is measured by the uptake of [3H]thymidine into cell DNA. The greater the class II MHC differences between the donor and recipient cells, the more [3H]thymidine uptake will be observed in an MLR assay.
Mixed Lymphocyte Reactions/culture contd..
• Intense proliferation of the recipient lymphocytes indicates a poor prognosis for graft survival.
• The advantage of the MLR over microcytotoxicity typing is that it gives a better indication of the degree of TH-cell activation generated in response to the class II MHC antigens of the potential graft.
• The disadvantage of the MLR is that it takes several days to run the assay.
• If the potential donor is a cadaver, for example, it is not possible to wait for the results of the MLR, because the organ must be used soon after removal from the cadaver. In that case, the microcytotoxicity test, which can be performed within a few hours, must be relied on.
Tissue matching:
cell-mediated lympholysis (CML) assay
• contributed to understanding of the mechanism of target-cell killing by CTLs.
• In this assay, suitable target cells are labeled intracellularly with chromium-51 (51Cr) by incubating the target cells with Na2
51CrO4.
– After the 51Cr diffuses into a cell, it binds to cytoplasmic proteins, reducing passive diffusion of the label out of the cell.
– When specifically activated CTLs are incubated for 1–4 h with such labeled target cells, the cells lyse and the 51Cr is released.
– The amount of 51Cr released correlates directly with the number of target cells lysed by the CTLs.
• By means of this assay, the specificity of CTLs for allogeneic cells, tumor cells, virus-infected cells, and chemically modified cells has been demonstrated.

NEWER ASSAYS
• Molecular HLA typing for alleles PCR using sequence specific primers– Low resolution– Intermediate – High
• RFLP with southern blotting
Various types of transplants
Tissue and Organ Transplantation
• Today it is possible to transplant many different organs and tissues including.Most common transplantation is blood
transfusion.Bone Marrow transplantationOrgans : Heart, kidneys, pancrease, lungs,
liver and intestines.Tissues : include bones, corneas, skin, heart
values, veins, cartilage and other connective tissues.
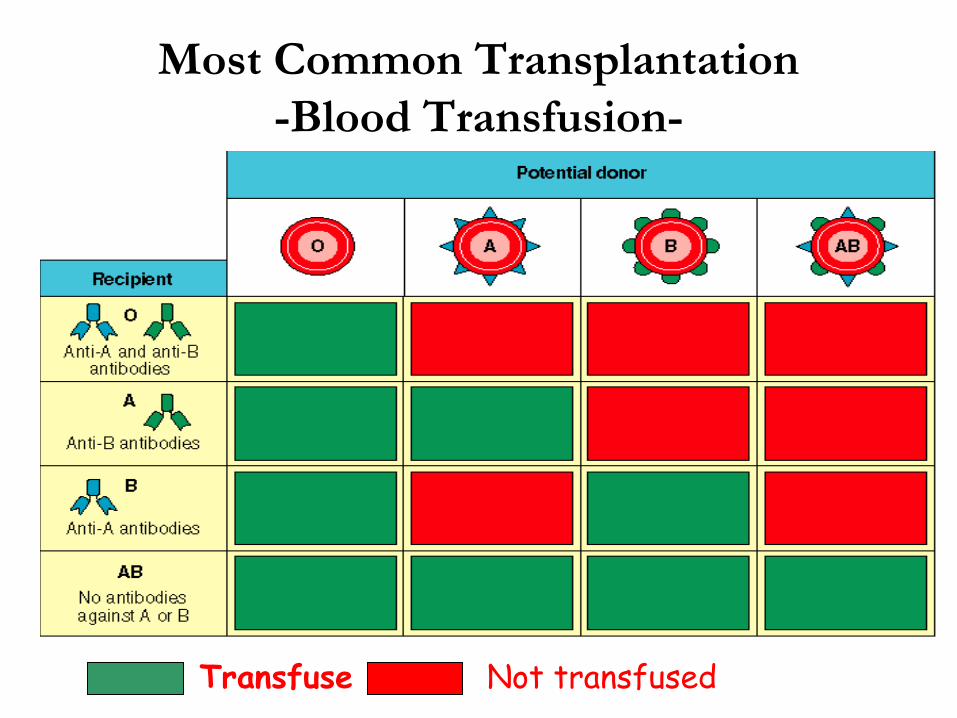
Most Common Transplantation-Blood Transfusion-
Transfuse Not transfused
Bone Marrow Transplantation
• Used for Leukemia, Anemia and immunodeficiency, especially severe combined immunodeficiency (SCID).
• About 109 cells per kilogram of host body weight, is injected intravenously into the recipients.
• Recipient of a bone marrow transplant is immunologically suppressed before grafting.
– Eg. Leukemia patients are often treated with cyclo-phosphamide and total body irradiation to kill all cancerous cells.
• Because the donor bone marrow contains immunocompetent cells, the graft may reject the host, causing graft versus host disease (GVHD).
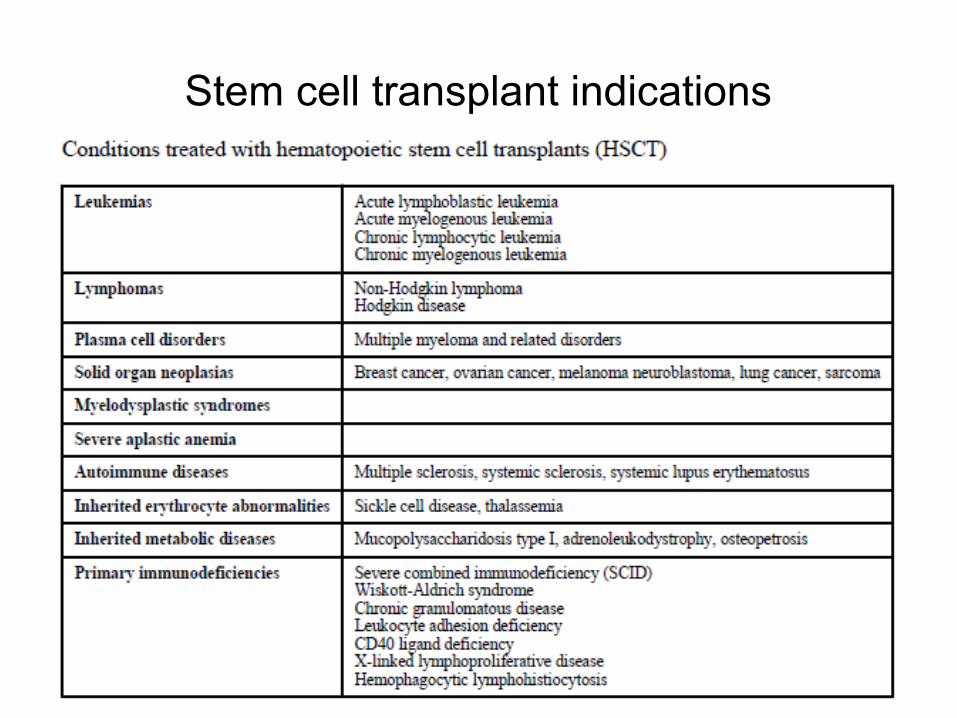
Stem cell transplant indications
Heart Transplantation :– First heart transplant in South Africa by Dr. Christian Barnard in
1964.– One year survival rate is >80%.– HLA matching is desirable but not often possible, because of the
limited supply of heart and the urgency of the procedure.
Lung Transplantation :– First attempt in 1963 by Hardy and Co - workers.– First successful transplantation by Toronto group in 1983.– In conjunction with heart transplantation, to treat diseases such
as cystic fibrosis and emphysema or acute damage to lungs.– First year survival rate is about 60%.
Kidney Transplantation :– Diseases like diabetes and various type of nephritis
can be elleviated by kidney transplantation.– Survival rate after one year transplantation is >90%.– 25,000 candidates are waiting for kidney
transplantation.
Liver transplantation :– It treat congenital defects and damage from viral
(hepatitis) or chemical agents. (Chronic alcoholism).– Liver one year survival exceeds 75% and five year is
70%.
Pancreas Transplantation :• Offers a cure for diabetes mellitus.• Graft survival is 72% at one year.• Further improved if a kidney is transplanted
simultaneously.
• Overall goal - to prevent the typical diabetic secondary complications.
Skin grafting :• It is used to treat burn victims.• In severe burn, grafts of foreign skin may be used and
rejection must be prevented by the use of immunosuppressive therapy.
Management of rejection
Principles of immunosuppression
• Same for all types of organs, intensive for (vital)thoracic organs than for kidney
• Aim is to maximise graft protection and minimise side effects
• Most regimens are based on calcineurin blockade and include steroid and an anti proliferative agent
• Need for immunosuppression is highest in the 1st three months but indefinite treatment is needed
• Risk of infection and malignancy
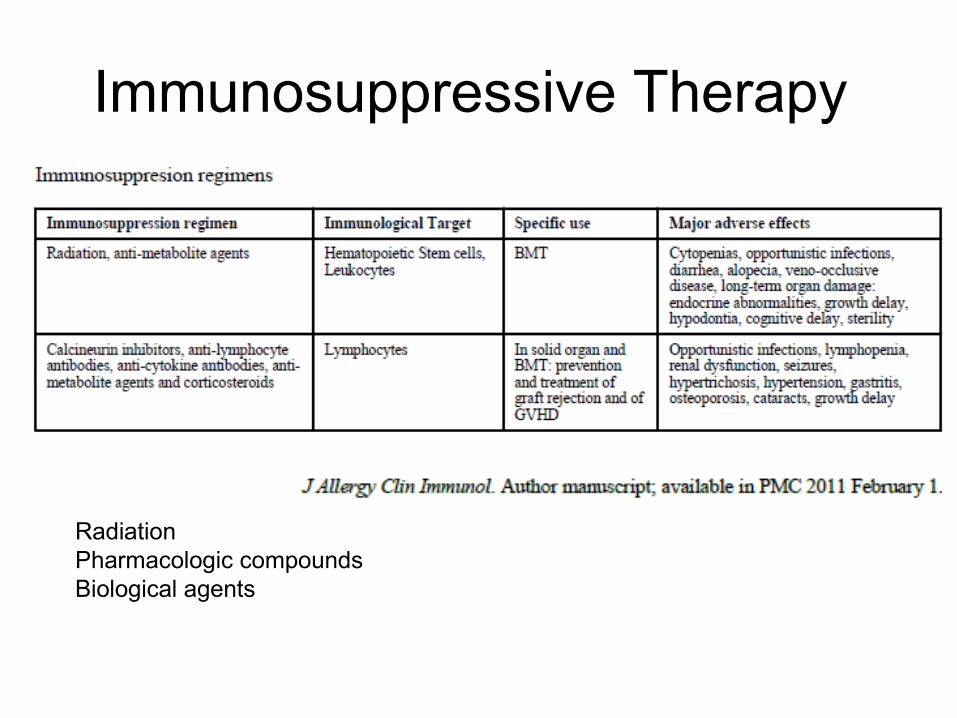
Immunosuppressive Therapy
Radiation Pharmacologic compoundsBiological agents
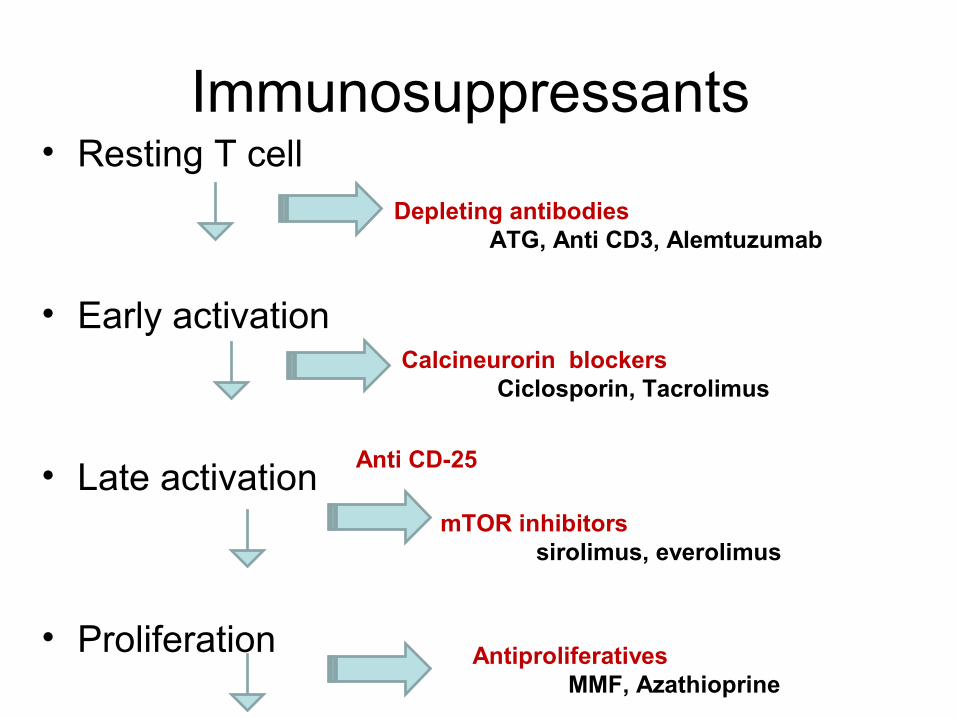
Immunosuppressants • Resting T cell
• Early activation
• Late activation
• Proliferation
Depleting antibodies ATG, Anti CD3, Alemtuzumab
Calcineurorin blockers Ciclosporin, Tacrolimus
Anti CD-25
mTOR inhibitorssirolimus, everolimus
AntiproliferativesMMF, Azathioprine
Immunosuppressive Therapy
Monoclonal antibodies • To suppress the activity of subpopulation of T-cells.• To block co-stimulatory signals.• Ab to the CD3 molecule of TCR (T cell receptor) complex results in
a rapid depletion of mature T-cells from the circulation. • Ab specific for the high-affinity IL-2 receptor is expressed only on
activated T-cell, blocks proliferation of T-cells activated in response to the alloantigens of the graft.
• To treat donor’s bone marrow before it is transplanted. • Molecules present on particular T-cells subpopulation may also be
targeted for immunosuppressive therapy.• Antibody to CD4 shown to prolong graft survival. • Ab specific for implicated cytokine can prolong the survival of graft.
Immunosuppressive Regimen
• Induction and Maintainance• Induction
– Ciclosporin/tacrolimus in combination with anti-CD25 monoclonal antibody
• Maintainance – Dual therapy
» Ciclosporin/tacrolimus in combination with steroids – Triple therapy
» Ciclosporin/tacrolimus in combination with MMF & steroids
– Quadruple therapy» Polyclonal antibody followed by Ciclosporin /
tacrolimus in combination with MMF & steroids
Complications - immunosuppression1. Infections –• more difficult to recognize infection in transplant recipients
• emergence of new clinical syndromes (e.g., polyomavirus type BK nephropathy) and by infections due to organisms with antimicrobial resistance.
• The spectrum of potential pathogens is broad, and infection often progresses rapidly.
• Early and specific microbiologic diagnosis is essential for guiding treatment and minimizing nonessential drug therapy. Invasive diagnostic procedures are often required for accurate and timely diagnosis..
• Vaccines for community acquired infections
• Epidemiologic Exposures
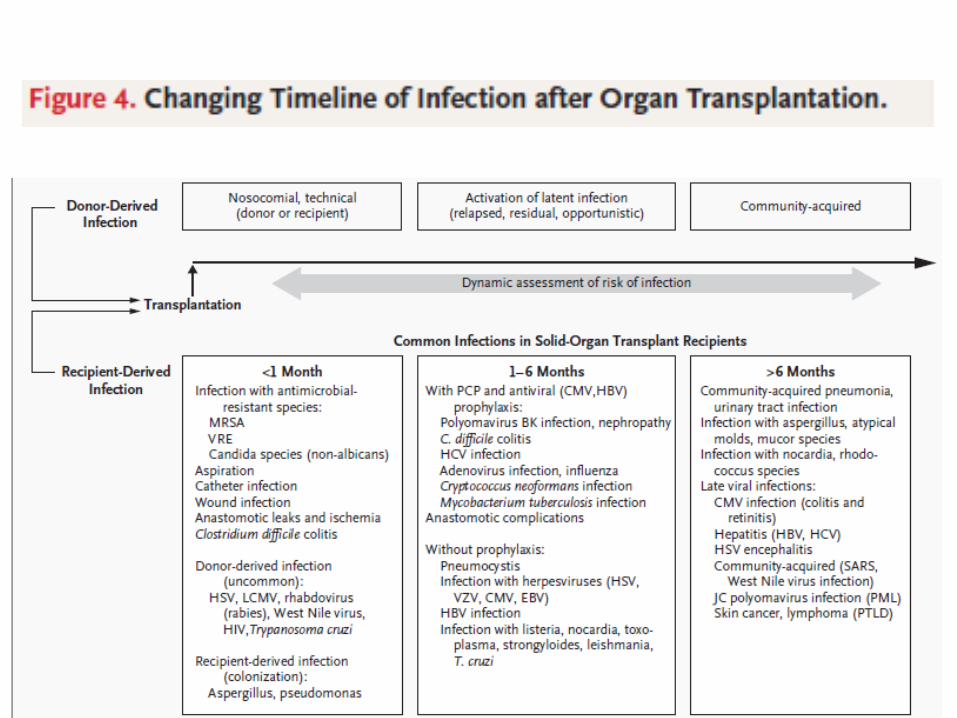
1. donor-derived infections, Example MTB, Trypanosoma cruzi, CMV, VRE
2. recipient-derived infections, example MTB, strongyloides, T. cruzi, CMV, EBV, HSV, VZV, HIV, HBV, HCV, histoplasma, coccidiodes immitis, paracoccidiodes
3. nosocomial infections, methicillin-resistant Staphylococcus aureus, vancomycin-resistant enterococcus, fluconazole-resistant candida species, Clostridium difficile, and antimicrobial-resistant gram-negative bacteria or aspergillus species.
4. community infections: relatively benign in normal person, such as aspergillus or nocardia species, C. neoformans in birds, and respiratory viruses with subsequent bacterial or fungal superinfection.
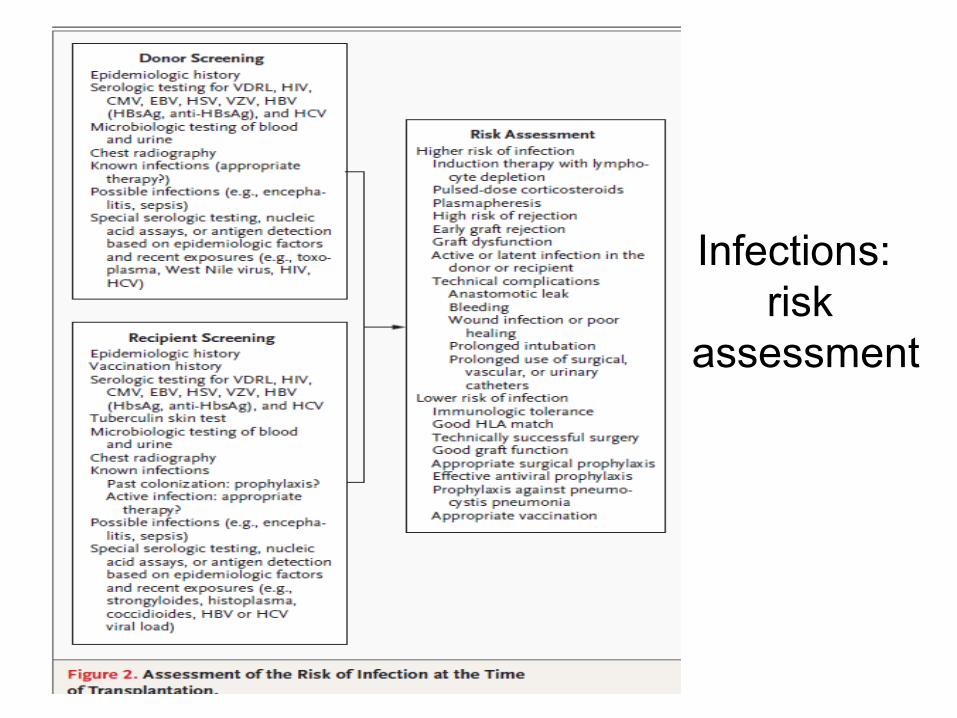
Infections: risk
assessment
Donor tested positive
• Absolute contraindications– HIV, sepsis, or unexplained fever, rash, encephalitis, or
untreated infectious syndromes.• Contraindicated earlier but now accepted
– some livers from donors who were seropositive for Chagas’ disease have been used successfully with benznidazole prophylaxis
– organs from donors infected with the hepatitis B virus (HBV) and who had test results that were positive for antibodies against hepatitis B core antigen and negative for antibodies against hepatitis B surface antigen were rejected in the past, they are currently used for some recipients who have been vaccinated or who were previously infected, provided there is treatment with specific antiserum and anti-HBV antiviral agents.
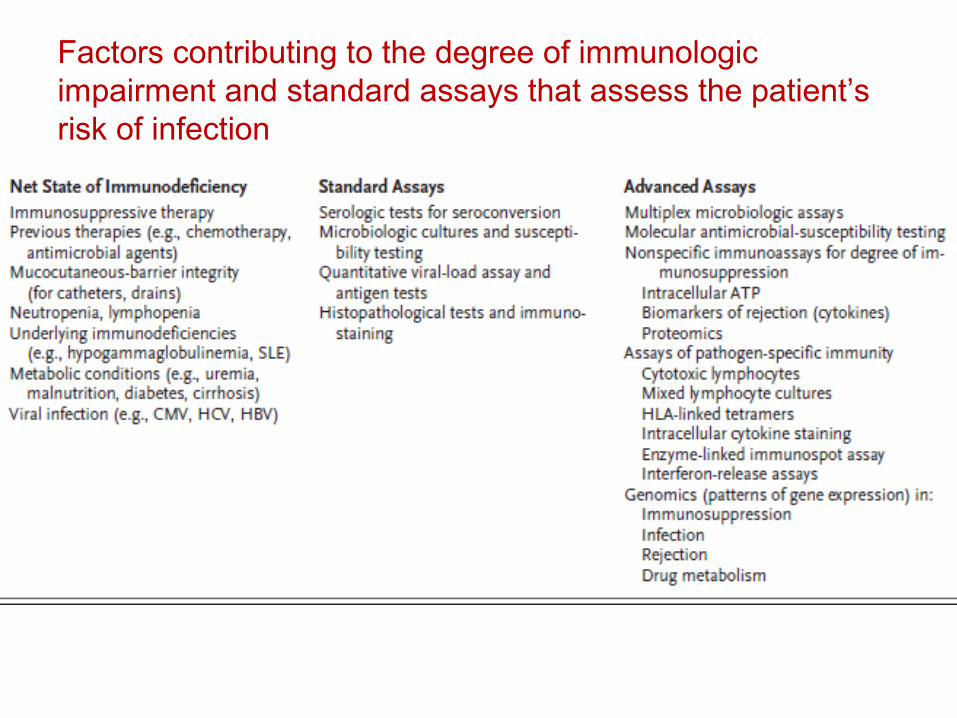
Factors contributing to the degree of immunologic impairment and standard assays that assess the patient’s risk of infection
• CMV– Severe disease - FATAL
• Either endogenous / from new organ • Match if both seronegative but not when donor
seropositive and recipient seronegative• Clinical picture depends on organ most affected
» Pneumonia» Gastrintestinal» Hepatitis» Encephalitis
Organ donation
Networks coordinating
Local network

Donor Eligibility
• Age limit between 2 yrs to 65 yrs
• Blood group same rules apply except for Rh – not considered
What are the steps of donation after death?
• Once patient is admitted; all efforts are made to stabilize the patients. If all efforts fail, patient is pronounced brain-dead after evaluation, testing and documentation.
• Consent from the family is obtained to proceed with donation and organ procurement organization (OPO) is informed. Consent from coroner/legal authorities is obtained.
• In the mean time the organ donor is maintained on ventilator, stabilized with fluids, medications and undergoes numerous laboratory tests. Recipients are also identified for placement of organs.
• Surgical team are mobilized and coordinated to arrive at hospital removal of organs and tissues. Donor is brought to the operating room. Multiple organ recovery is performed with organs being preserved through special solutions and cold packing. Ventilator support is discontinued. Donor’s body is surgically closed and released.
Organ donation• The only organisation in Karnataka through whom organ donations
and transplants are co-ordinated is ZCCK (Zonal Coordination Committee of Karnataka For Organ Transplantation).
• ZCCK is a non-profit medical service working with centres recognised by the government for cadaveric transplantation and co-ordination for the same.
• A list of patients awaiting transplant is maintained. On receiving information about potential donors, ZCCK will assess suitability for organ donation.
• Based on the blood group and other criteria for the organ matching, the recipients will be selected, brought into hospital and prepared for the operation. A team of surgeons will perform the organ retrieval from the donor. In medico-legal cases, ZCCK will help the family with the formalities involved.
Future prospects
Transplant vaccine
• To induce donor-specific tolerance
• The use of tolerogenic dendritic cells(DC) has shown great potential, as preliminary experiments in rodents have demonstrated that administration of tolerogenic DC prolongs graft survival.
• Recipient DC, Donor DC, or Donor Ag-pulsed recipient DC have been used in preclinical studies and administration of these cells with suboptimal immunosuppression increases their tolerogenic potential.
Summary• More than 50,000 people, waiting for compatible donor.
For ethical an practical reasons, species closely related to human such as Chimpanzee have not been widely used.
• Xenogeneic transplantation may be major issue of research xenograft technology including genetically modified animal may become a new source of organ supply.
• Techniques such as transgenic animal production and wide range of research in this field hope to result in opening a new window for the process of transplantation immunology.
Summary
• Advances in transplantation immunology have allowed the exponential growth of organ and tissue transplantation in medicine over the last three decades.
• Newer immunosuppressive agents have allowed the control of solid organ and tissue rejection and of graft-versus-host disease even when HLA incompatibility is present.
• For the treatment of hematological disorders, including primary immunodeficiencies, hematopoietic stem cell transplantation is not only feasible but it is the treatment of choice in many cases.
• Future developments – novel immunosuppressors with less toxicity and more specificity to control graft
rejection while sparing overall immunity and thereby enabling better infection control.
– Gene therapy replacing bonemarroow/stem cell therapy
References
• Robins Basic pathology 8th edition
• Ananthanarayan and Paniker’s text book of Microbiology
• Baily and Love Text book of Surgery
• Stites - Medical immunology 10th edition
• Journal articles

THANK YOU