Embed Size (px)
Citation preview

TRYPANOSOMIASIS
Dr.T.NIKKIN
II YEAR POSTGRADUATE
DEPT OF COMMUNITY MEDICINE
SRMC&RI
TWO FORMS OF TRYPANOSOMIASIS
• Trypanosomiasis is a vector borne parasitic disease
• Two types:
a) African Trypanosomiasis (sleeping sickness)
b) American Trypanosomiasis (chagas disease)

AFRICAN TRYPANOSOMIASIS (SLEEPING SICKNESS)
INTRODUCTION
• Caused by infection with protozoan parasite , Trypanosoma brucei
• Transmitted to humans by vector, Tsetse fly (glossina species)
• The vector, Tsetse fly is found only in the African regions
• T.brucei gambiense – West African sleeping sickness
• T.brucei rhodesiense – East African sleeping sickness
EPIDEMIOLOGY
• Sleeping sickness occurs only in 36 sub-Saharan African countries
• T.brucei gambiense accounts for > 98% of cases of sleeping sickness
• Annual number of cases – 7000 to 10000
• In 1998 – 40000 cases
• In 2009 – 9478 cases
• In 2013 – 7216 cases

EPIDEMICS IN THE PAST
• One between 1896 and 1906 – Uganda & Congo basin
• One in 1920 – number of African countries
• Recent epidemic in 1970 and lasted till late 1990s
• 1920 epidemic was controlled by mobile teams which screened millions of people
• <5000 cases reported in mid-sixties
• After this success, surveillance measures were relaxed which led to reappearing of the disease
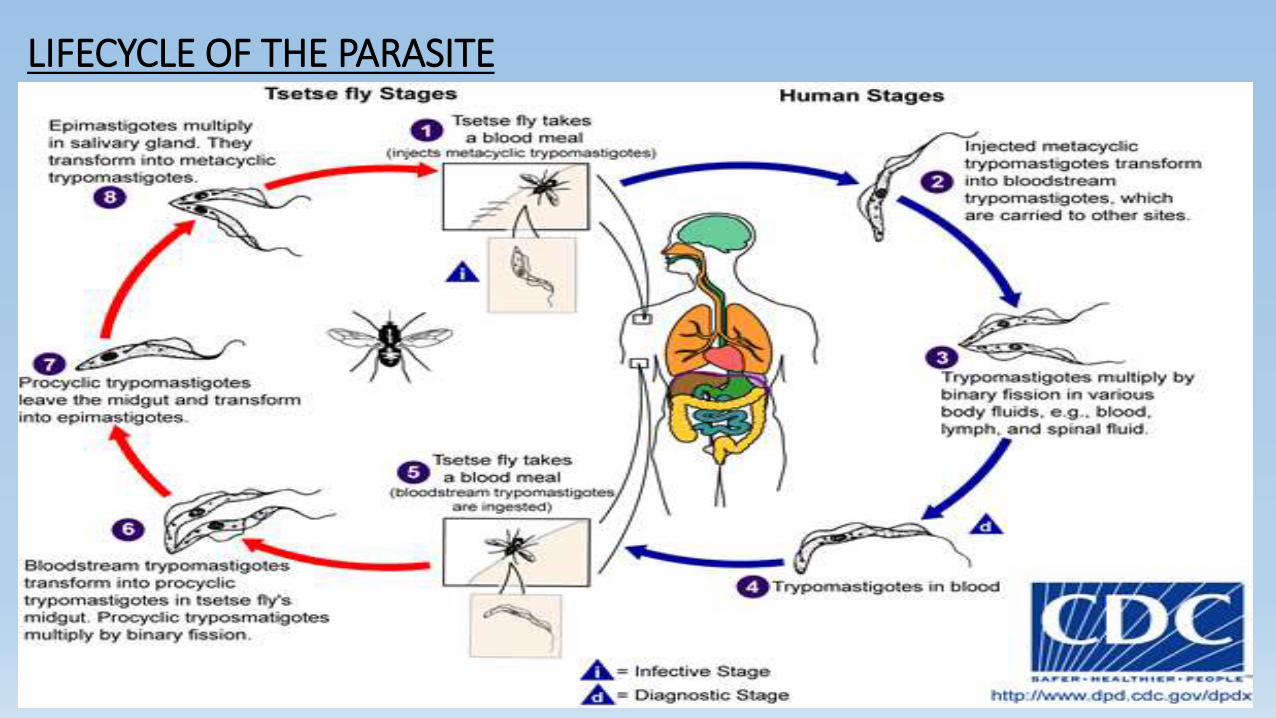
LIFECYCLE OF THE PARASITE

MODES OF TRANSMISSION
• The most common method of transmission is by the bite of the tsetse fly
• Mother to child transmission
• Mechanical transmission
• Accidental infection from laboratories

CLINICAL FEATURES
• Two stages:
a) Haemolymphatic stage: multiplies in peripheral circulation, subcutaneous tissues and lymph
b) Neurological/Meningoencephalic stage: enters CNS by crossing blood brain barrier
Without treatment the disease is fatal…

CLINICAL FEATURES
Characteristic T.b.gambiense T.b.rhodesiense
Disease progression Slow Rapid
Stage I Symptoms Fever, headache, malaise Fever, swollen lymphnodes, itching
Time of CNS invasion 1 to 2 years 4 to 5 weeks
Stage II Symptoms Daytime sleepiness with Night time sleep disturbance, paralysis, coma
Mental deterioration
Time to death 2 to 4 years Within months
DIAGNOSIS
• Screening:
Serological tests are used(available only for T.gambiense)
Serological tests are not reliable
• Microscopic Examination:
Lymph & blood – Stage I infection
CSF – Stage II infection & for staging
Parasites are not easily visible in T.gambiense infections and so concentration techniques may be used
• Clinical Examination:
For Posterior cervical lymphadenopathy
Not a Preferred method for diagnosis

TREATMENT FOR STAGE I• Pentamidine:
- discovered in 1941
- used against T.b.gambiense
- generally well tolerated
• Suramin:
- discovered in 1921
- used against T.b.rhodesiense
- causes Urinary tract problems and allergic reactions

TREATMENT FOR STAGE II
• Melarsoprolol:
- discovered in 1949(derived from arsenic)
- used against both the species
- causes reactive encephalopathy which can be fatal
• Eflornithine:
- discovered in 1990
- effective against T.b.gambiense only
- treatment regimen is strict but less toxic than melarsoprolol
• Combination of nifurtimox & eflornithine is used since 2009, effective against T.b.gambiense only.

VECTOR(TSETSE FLY)
Kingdom: Animalia
Phylum: Arthropoda
Class: Insecta
Order: Diptera
Family: Glossinidae
Genus: Glossina

VECTOR(TSETSE FLY)
• Morphology:
Glossinae are bloodsucking flies
Resembles the common housefly in appearance
Yellow or Dark-brown in colour
Measures about half an inch
Pair of wings are present which when folded, overlap each other
Rigid and non-retractile proboscis for sucking blood is seen
Found only in Africa

TSETSE FLY
• Life history:
The female does not lay eggs, but gives birth to a living larva, one at a time, 10 day intervals
The larva crawls to a suitable place and buries at an inch or so from the surface
Pupation starts in a few hours and lasts for a month
At the end of pupation, adult fly emerges
It lives for 100 days

TSETSE FLY
• Species and Habits:
More than 30 species are found but only 4 are dangerous to man
G.palpalis
G.tachinoides
G.morsitans
G.pallidepes
• Both the male and female flies bites
Riverine species
Savannah species
Attacks man
Attacks game
CONTROL OF AFRICAN SLEEPING SICKNESS
• Control involves 2 strategies:
1) Control of the reservoir
2) Control of the vector
• Control of the reservoir:
Humans are the major vectors for T.b.gambiense and so control is mainly by population screening and treatment of the disease in those who are having the disease
Various animal hosts acts as reservoir for T.b.rhodesienseinfections, hence control of reservoir is very difficult with rhodesiense.
CONTROL OF THE VECTOR(TSETSE FLIES)
• 1) Insecticides: DDT(25%) and Dieldrin(20%) are used. The insecticide is applied from aircraft when large areas are to be covered
• 2) Clearing of vegetation: where tsetse flies live and breed. It gives very slow results
• 3) Game destruction: Large tracts of Africa has been cleared of the tsetse flies by this method in the past but now given up
• 4) Genetic control: Through “sterile male technique”
• 5) Fly traps: Used widely nowadays. Blue coloured traps coated with insecticides are used.

PREVENTION OF AFRICAN TRYPANOSOMIASIS
• Long-sleeved shirts and Medium-weight pants with neutral colourscan be used
• Vehicles should be thoroughly inspected before entering an area of residents
• Avoiding bushes
• Permethrin impregnated clothing and repellents can be used.
AMERICAN TRYPANOSOMIASIS(CHAGAS DISEASE)

INTRODUCTION
• Chagas disease is a potentially life-threatening disease, caused by the protozoan parasite, T.cruzi
• Found mainly in 21 endemic Latin American countries
• Usually transmitted by contact with faeces of Triatomine bugs, which acts as a vector for this disease
• Chagas disease was once entirely present in Latin America but now it has spread to other continents

EPIDEMIOLOGY
• About 7 to 8 million of cases of chagas has been reported worldwide
• Most of the cases are from Latin America alone which is an endemic area for American trypanosomiasis
• In the past decades cases have been reported from other countries too
• It is mainly due to population from Latin America to rest of the world.

LIFECYCLE OF THE PARASITE
MODES OF TRANSMISSION
• T.cruzi infection is mainly spread by the contact with faeces of Triatomine bugs
• Infection can also occur from:
mother-to-baby (congenital),
contaminated blood products (transfusions),
an organ transplanted from an infected donor,
laboratory accident, or
contaminated food or drink (rare)
CLINICAL FEATURES
• Chagas disease has an acute and chronic phase
• Acute phase:
It occurs immediately after the parasite entry into the body and may last for 2 months
Infection may be mild or asymptomatic
Parasites are usually found in the blood during this phase
The symptoms includes fever, headache, enlarged lymph glands, pallor, muscle pain , difficulty in breathing, etc…
In 50% of patients bitten by the bug, the characteristic purplish swelling of eyelid is seen on one eye.

CLINICAL FEATURES
• Chronic phase:
After the acute phase most patients go into the “chronic indeterminate” phase, where parasites are not found on blood
Patients are unaware and may remain asymptomatic for life
About 30% may develop cardiac complications and upto 10% may develop G.I. complications and neurological problems
In later years, patient may die from progressive cardiac failure due to destruction of heart wall by the parasite.
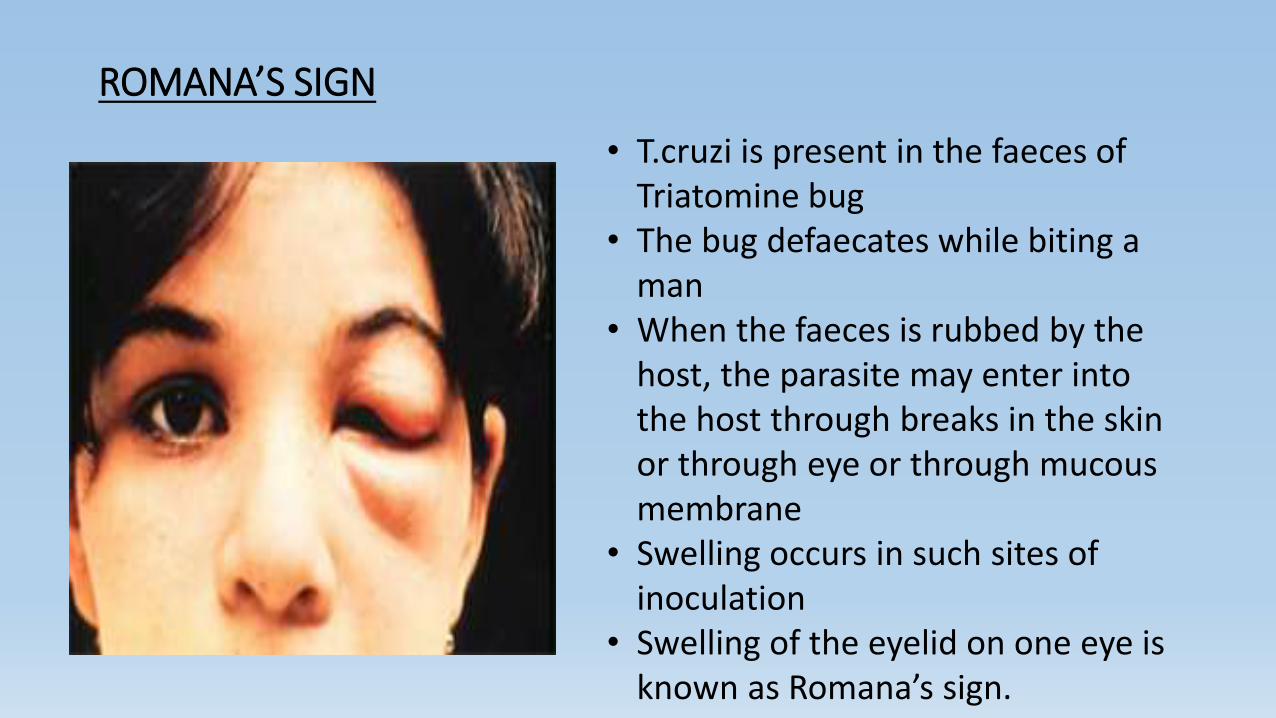
ROMANA’S SIGN
• T.cruzi is present in the faeces of Triatomine bug
• The bug defaecates while biting a man
• When the faeces is rubbed by the host, the parasite may enter into the host through breaks in the skin or through eye or through mucous membrane
• Swelling occurs in such sites of inoculation
• Swelling of the eyelid on one eye is known as Romana’s sign.

DIAGNOSIS
• Acute phase:
Blood smears are used for diagnosis of acute phase
Both thick and thin smears can be made and stained for microscopic visualization of the parasite
• Chronic phase:
Clinical findings along with clinical history is used for diagnosis of chronic phase
Two or more serological tests are also necessary to support the diagnosis.

TREATMENT
• Acute phase:
Benznidazole and nifurtimox are 100% effective against the parasite during the acute phase
Drugs lose their efficacy as the disease progresses
• Chronic phase:
Cardiac drugs may be given as per the symptoms of the patient
Benznidazole and nifurtimox are effective in immunosuppressed patients and in children

VECTOR(REDUVIID BUG)
Kingdom: Animalia
Phylum: Arthropoda
Class: Insecta
Order: Hemiptera
Family: Reduviidae
Subfamily: Triatominae
Genus: Triatoma

MORPHOLOGY
• Cone nosed bugs, assassin bugs, kissing bugs, barber bugs
• Reduviid bugs are relatively larger (20 mm to 28 mm)
• Body can be divided into Head , Thorax and Abdomen
• Head – Cone shaped, 3 segmented rostrum, pair of eyes & antennae
• Thorax – 3 pairs of legs & 2 pairs of wings (forewings,hindwings)
• Abdomen – large in females & slender in males
- Pointed at tip in females & rounded at tip in males
- not fully covered by wings, flattened at uncovered areas
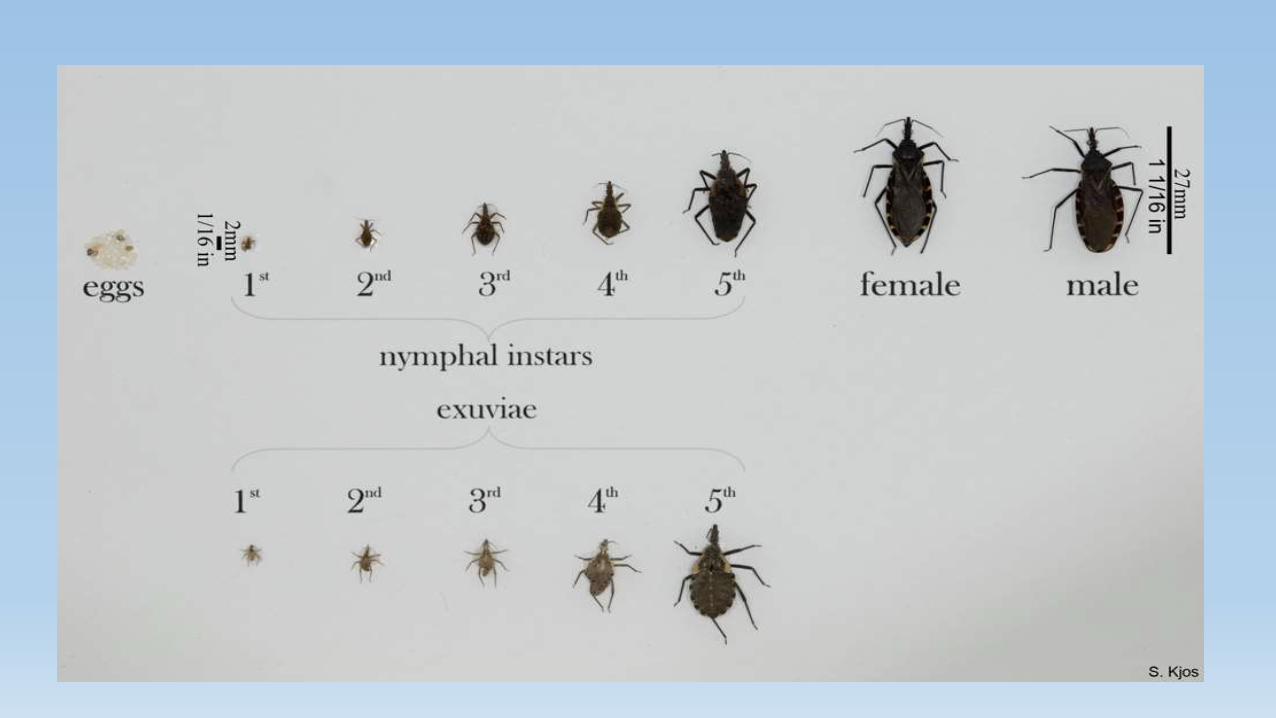
LIFECYCLE
• Life duration ranges between 4 and 24 months
• Incomplete metamorphosis
• Egg develops into 1st instar(nymph)
• Successively passes through 2nd,3rd,4th and 5th instar to develop into adults
• Adults are morphologically similar to the nymphal stages except that they are bigger in size
• Each bug undergoes one or two lifecycles per year
BEHAVIOUR
• During daytime, the bugs rests in dark crevices, behind pictures, palm thatched roof, among furnitures, boxes, clothes and in beds
• At night, the bugs bites and sucks blood
• Average feeding time is 15 to 25 minutes
PREVENTION AND CONTROL
• Improvement of houses to reduce or eliminate the hiding places is the best method
• Spraying of the walls and roofs of the houses with insecticides
- not suitable for porous walls(mud walls)
- synthetic pyrethroids are the insecticides of choice
• Insecticidal paints can be used for mud or porous walls
- contains 8.3% malathion emulsifiable concentrate mixed with polyvinyl acetate
- forms a thin film on the wall


REFERENCES
• http://www.who.int/mediacentre/factsheets/fs259/en/ [internet] ; accessed on 10/03/15
• http://www.cdc.gov/parasites/chagas/gen_info/index.html [internet]; accessed on 10/03/15
• http://www.cdc.gov/parasites/sleepingsickness/ [internet]; accessed on 10/03/15
• Maxcy, K. F., Rosenau, M. J., Last, J. M., & Wallace, R. B. (1998). Maxcy-Rosenau-Last public health & preventive medicine