Embed Size (px)
Citation preview
ULTRASOUND
BIOMICROSOPY IN
GLAUCOMA
Dr. Aditi Singh
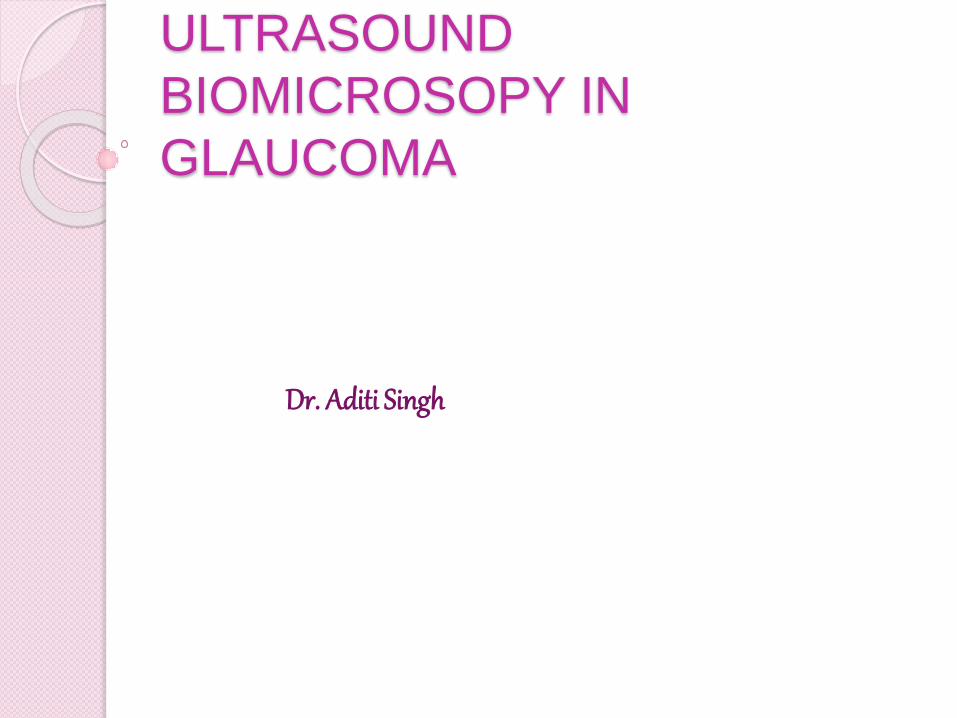
Ultrasound biomicroscope (UBM) is a high
frequency ultrasound machine used to image
ocular structures anterior to the pars plana region of the eye
Provides images of the tissues and structures
in vivo at microscopic resolution
Princess Margaret
Hospital at Toronto,
Canada in 1989.
Dr . Stuart Foster
They developed three probes - 50, 80 & 100 Mhz for
clinical trials .
50 MHz is an ideal compromise between depth and
resolution to visualize the entire anterior segment.
The first commercially available machine was
developed by Zeiss in 1991.
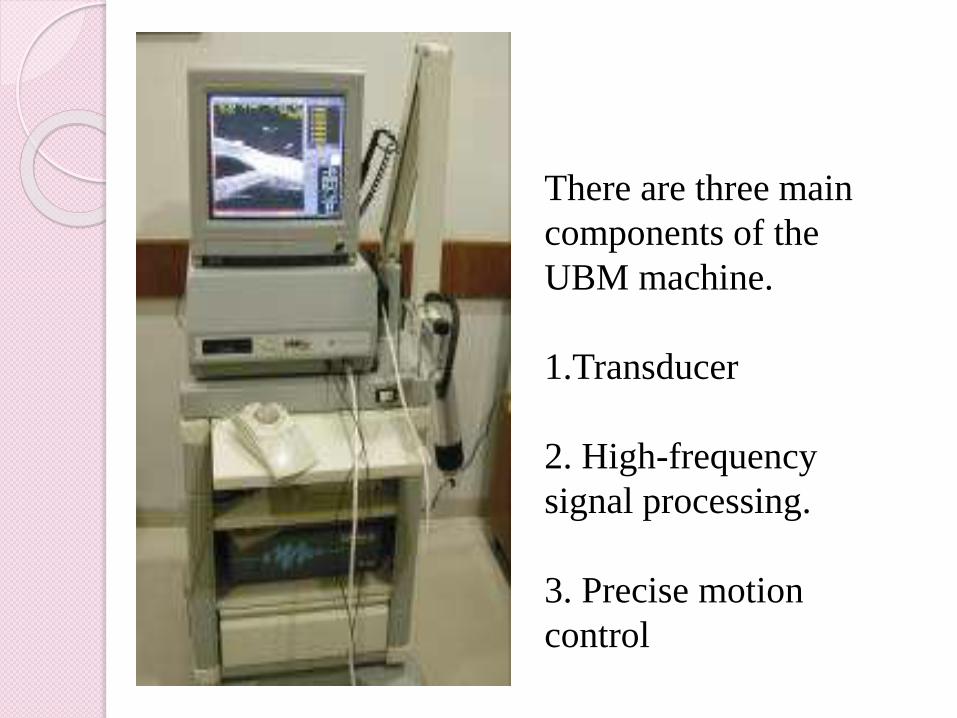
There are three main
components of the
UBM machine.
1.Transducer
2. High-frequency
signal processing.
3. Precise motion
control
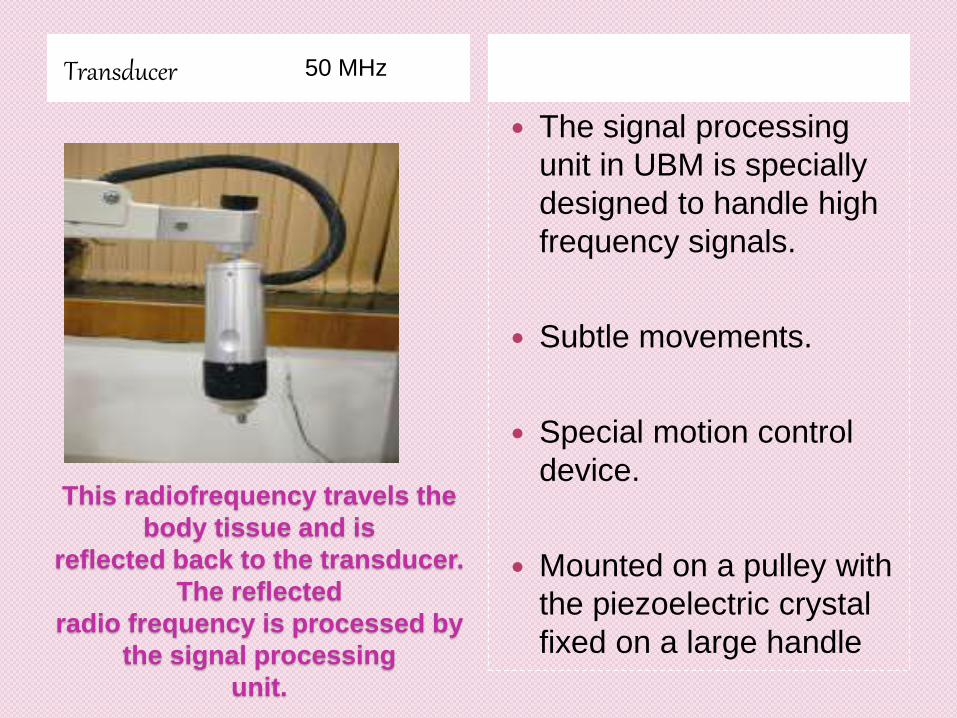
This radiofrequency travels the
body tissue and is
reflected back to the transducer.
The reflected
radio frequency is processed by
the signal processing
unit.
Transducer
The signal processing
unit in UBM is specially
designed to handle high
frequency signals.
Subtle movements.
Special motion control
device.
Mounted on a pulley with
the piezoelectric crystal
fixed on a large handle
50 MHz
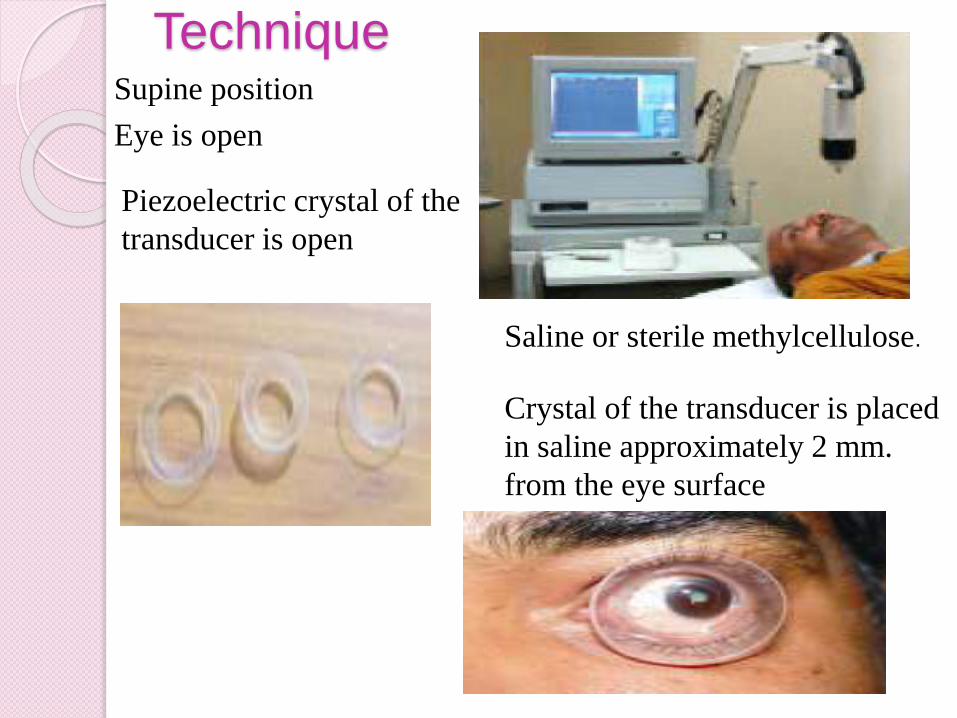
TechniqueSupine position
Eye is open
Piezoelectric crystal of the
transducer is open
Saline or sterile methylcellulose.
Crystal of the transducer is placed
in saline approximately 2 mm.
from the eye surface
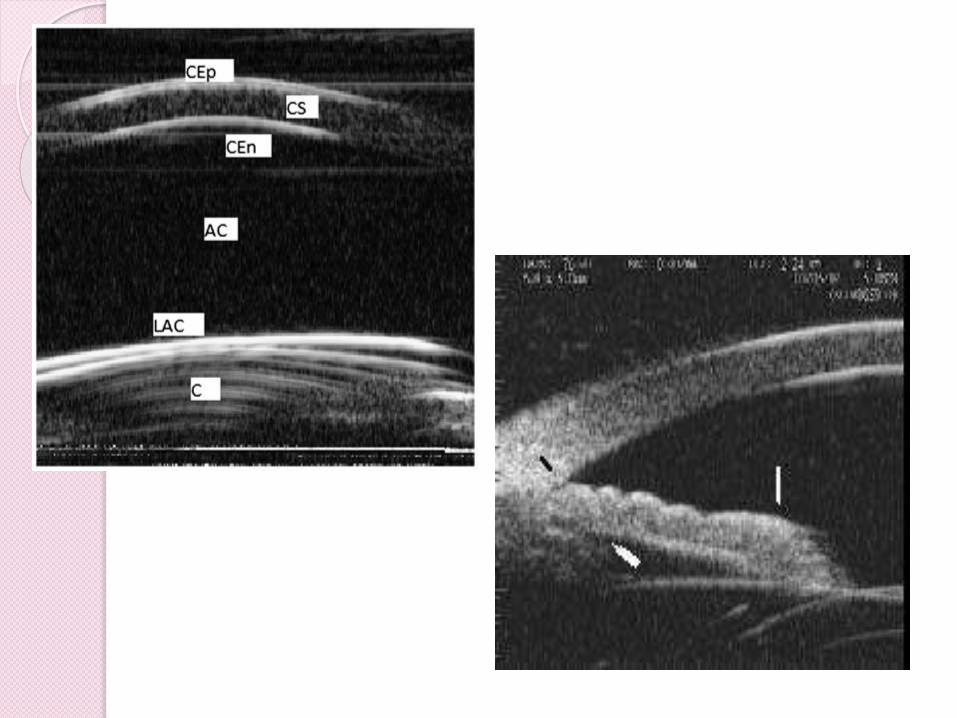
Normal anatomy Lateral resolution - 50µ
Axial resolution - 25µ
Depth of penetration- 4-5 mm.
Field of view is 4 x 4mm
Scan rate is 5 frames/second.
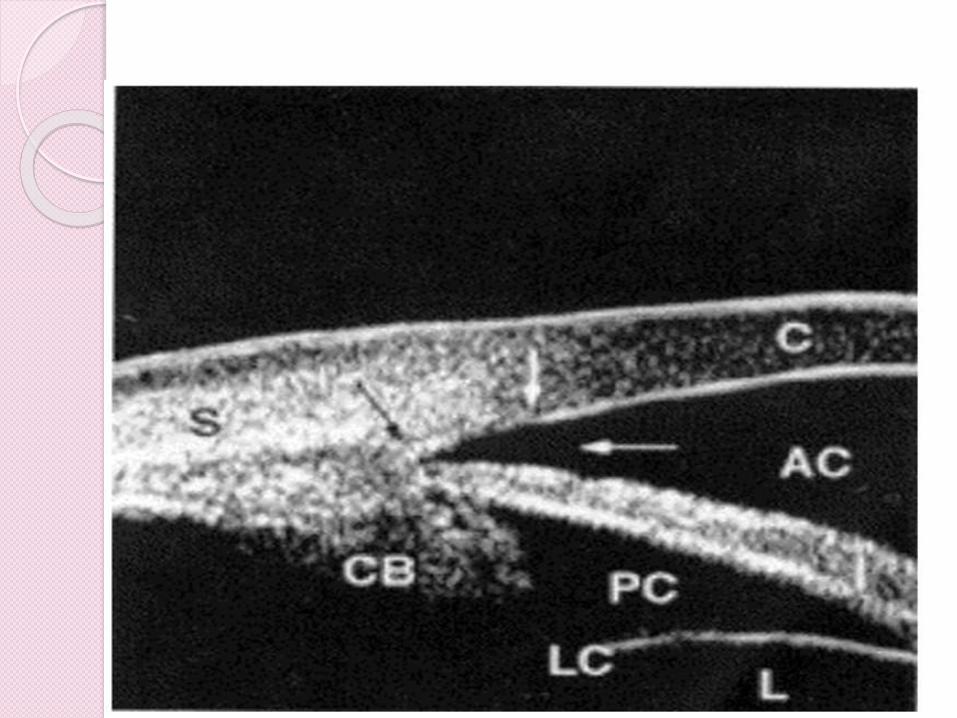
Cornea is the first structure.
Corneo-scleral junction
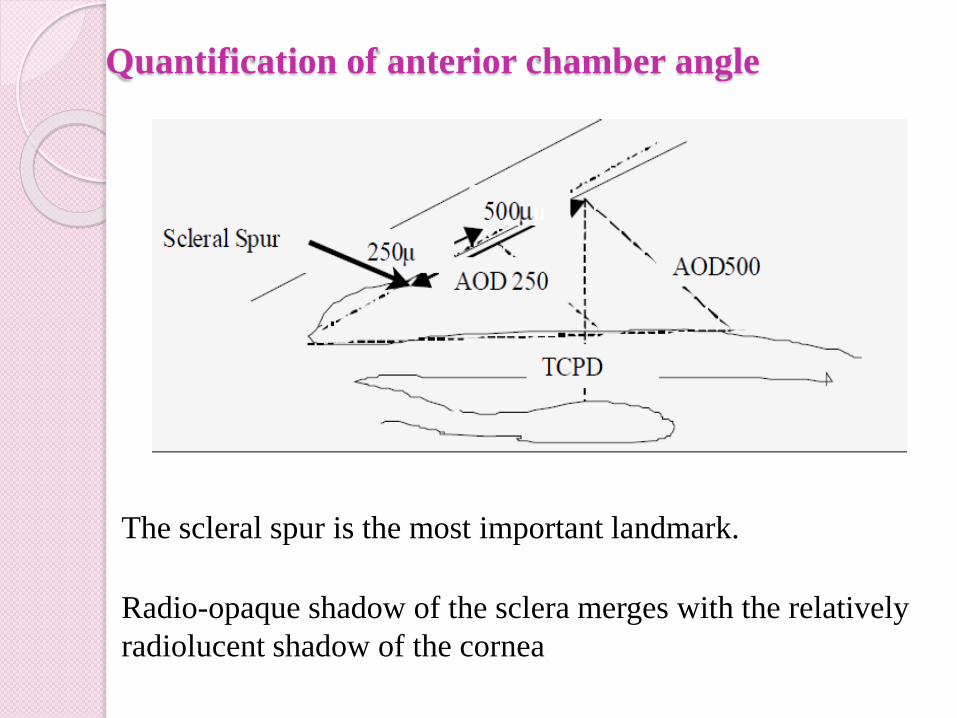
Quantification of anterior chamber angle
The scleral spur is the most important landmark.
Radio-opaque shadow of the sclera merges with the relatively
radiolucent shadow of the cornea
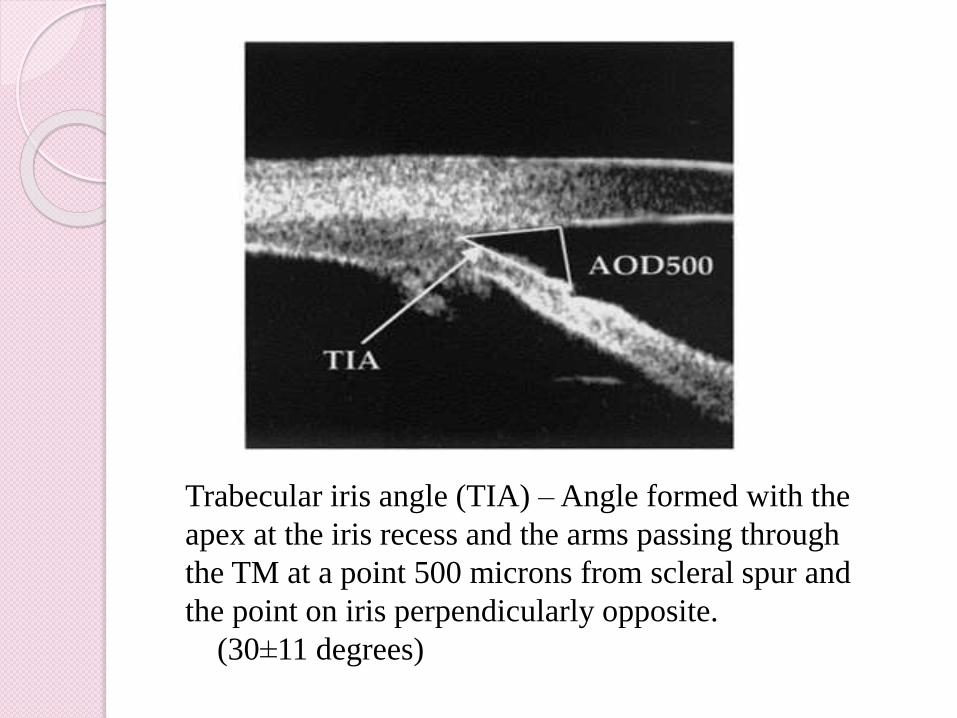
Trabecular iris angle (TIA) –Angle formed with the
apex at the iris recess and the arms passing through
the TM at a point 500 microns from scleral spur and
the point on iris perpendicularly opposite.
(30±11 degrees)
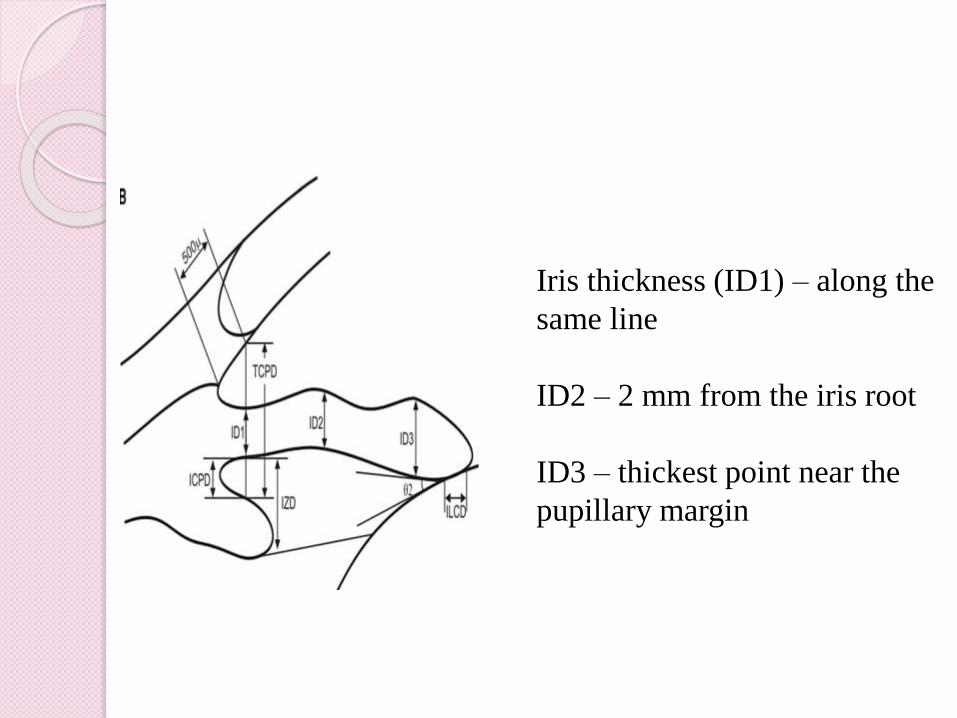
Iris thickness (ID1) – along the
same line
ID2 – 2 mm from the iris root
ID3 – thickest point near the
pupillary margin
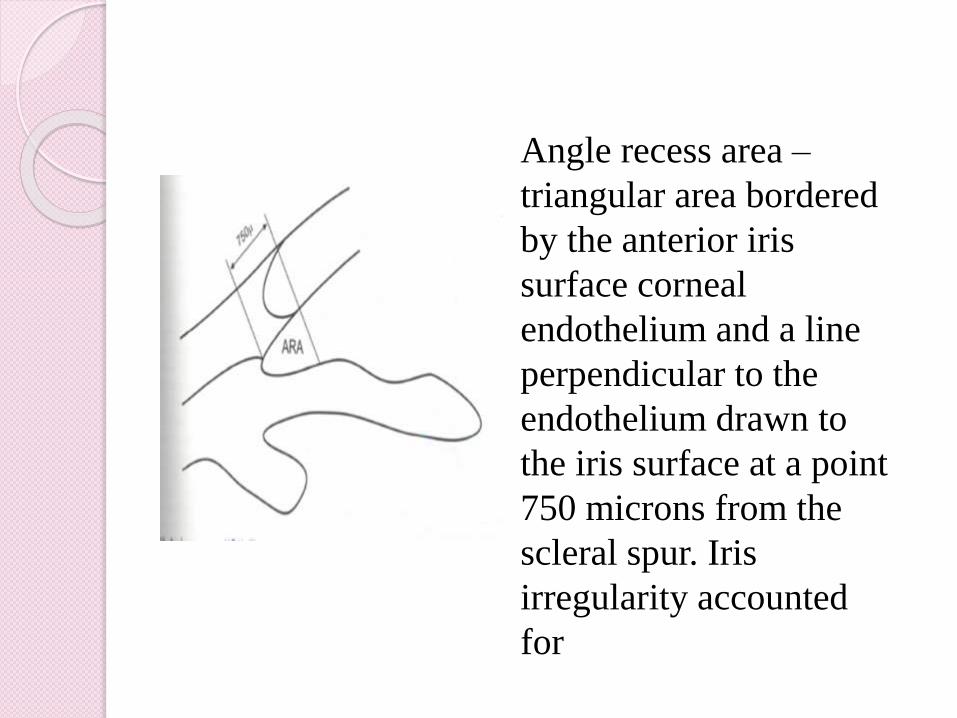
Angle recess area –
triangular area bordered
by the anterior iris
surface corneal
endothelium and a line
perpendicular to the
endothelium drawn to
the iris surface at a point
750 microns from the
scleral spur. Iris
irregularity accounted
for
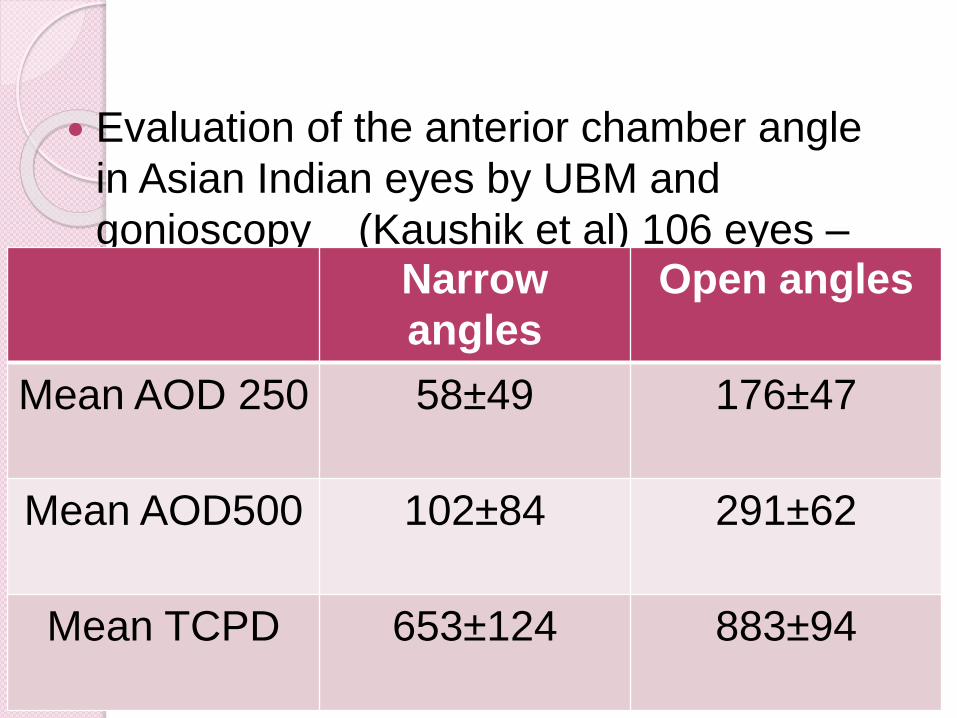
Evaluation of the anterior chamber angle
in Asian Indian eyes by UBM and
gonioscopy (Kaushik et al) 106 eyes –
narrow angles,57 eyes – open anglesNarrow
angles
Open angles
Mean AOD 250 58±49 176±47
Mean AOD500 102±84 291±62
Mean TCPD 653±124 883±94
Biometry of the Anterior Segment
Corneal thickness
Anterior chamber depth
Posterior chamber depth
IOL thickness
Iris thickness
Ciliary body thickness
Scleral thickness .
Cannot determine lens thickness
Determination of the Mechanism of Primary
Glaucoma
Able to determine the mechanism of elevated IOP
(angle-closure vs open-angle) by showing the
relationship between the peripheral iris and the
trabecular meshwork.
Imaging is possible, even in eyes with corneal
edema or corneal opacification that precludes
gonioscopy.
Open-angle glaucoma
Can measure the anterior chamber angle in
degrees
Assess the configuration of the peripheral iris
Evaluate the iris insertion in relation to the
trabecular meshwork
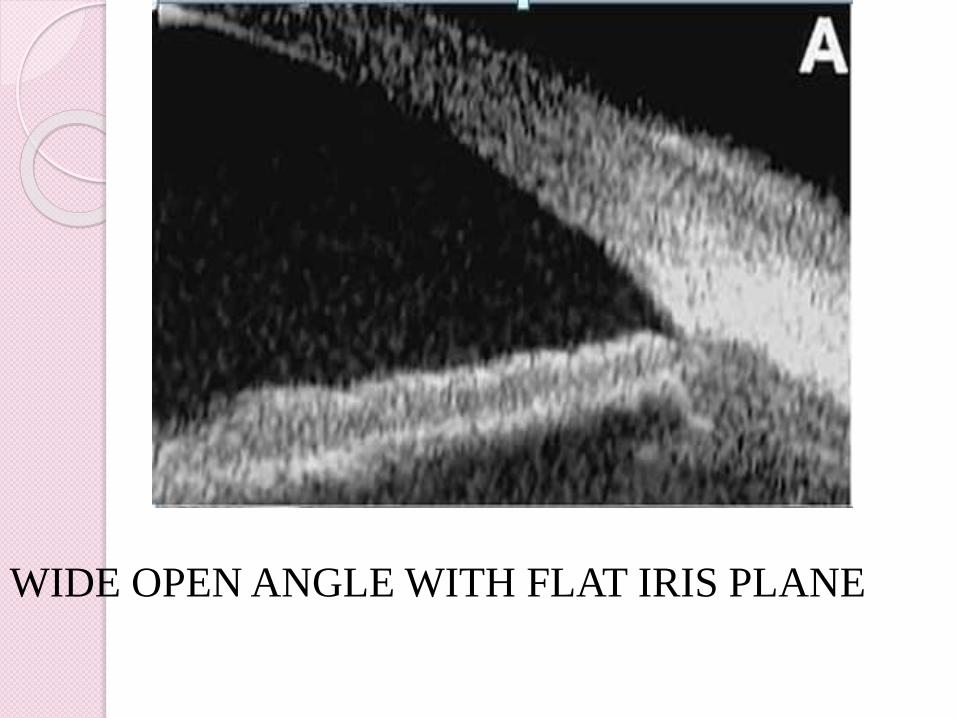
WIDE OPEN ANGLE WITH FLAT IRIS PLANE
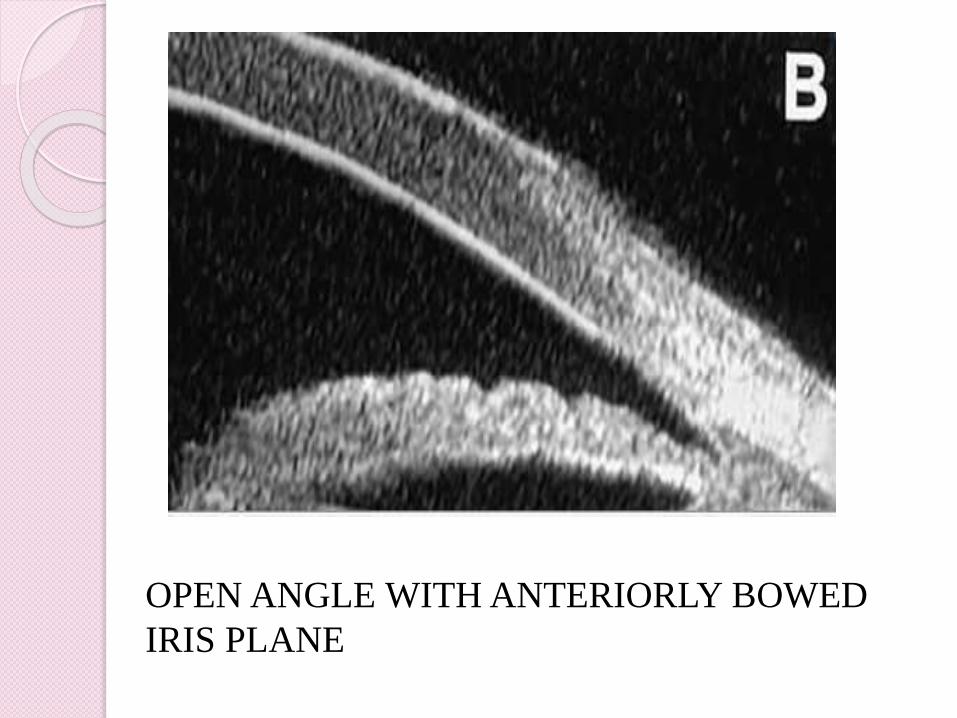
OPEN ANGLE WITH ANTERIORLY BOWED
IRIS PLANE
Determination of the Occludability of the
Angle
Dark room provocative testing
Studies the spontaneous occlusion of the angle
under conditions of decreased illumination
Provides useful qualitative information about
angle recess anatomy.
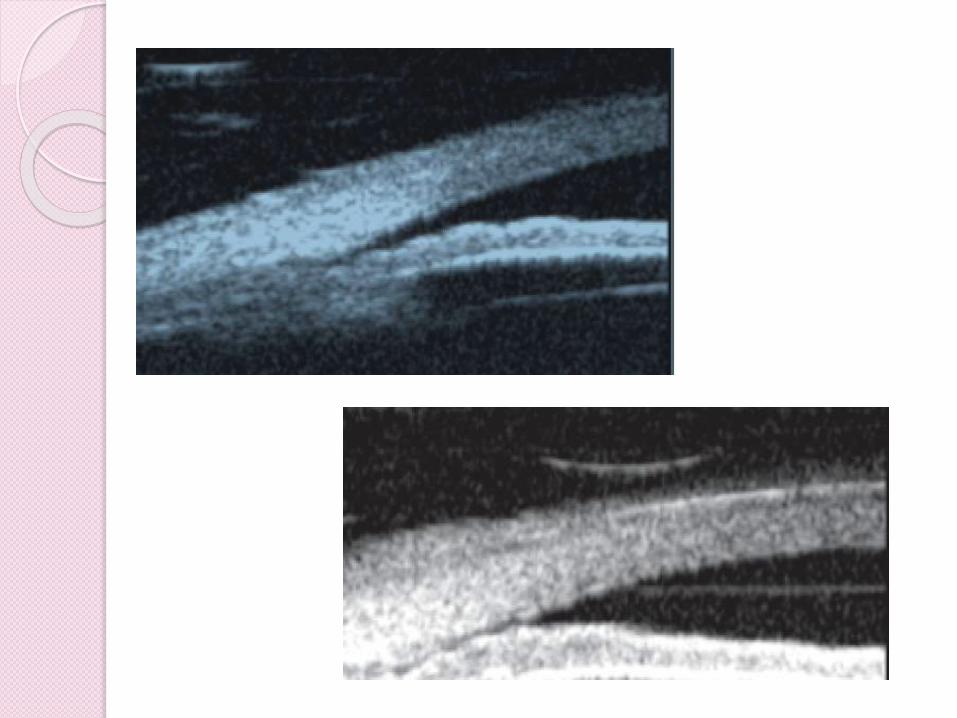
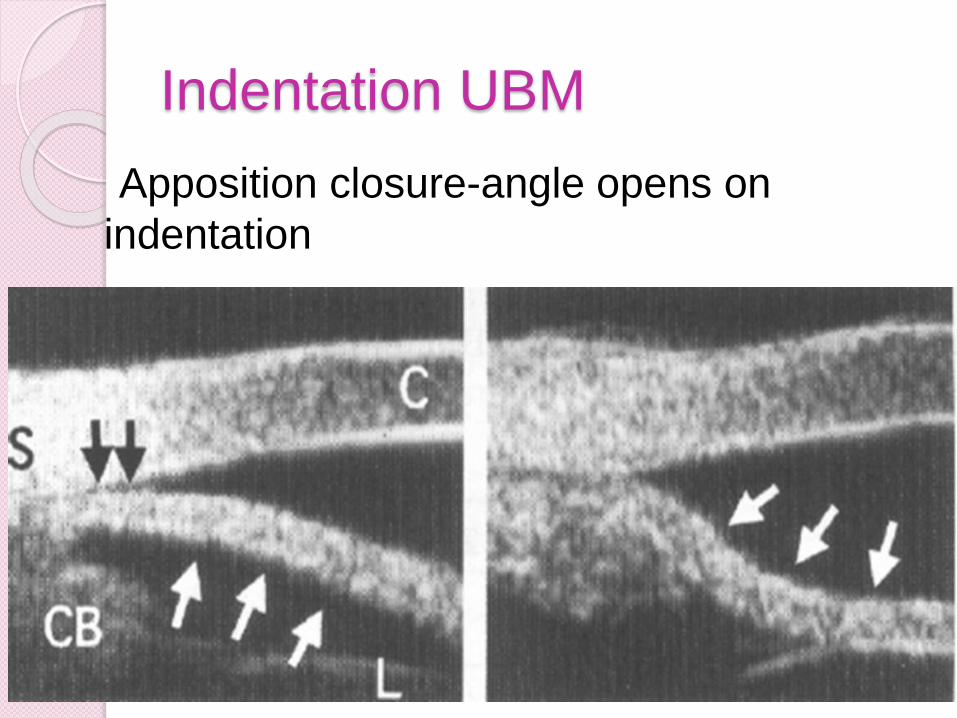
Indentation UBM
Apposition closure-angle opens on
indentation
Indentation UBM gonioscopy, new method for
assesing the angle
Angles widened with indentation.
The angle changes in eyes with relative pupillary
block were significantly greater than in eyes with
peripheral anterior synechie (PAS) or plateau iris
configuration (PIC).
Useful for diagnosing relative pupillary block, PAS,
and PIC.
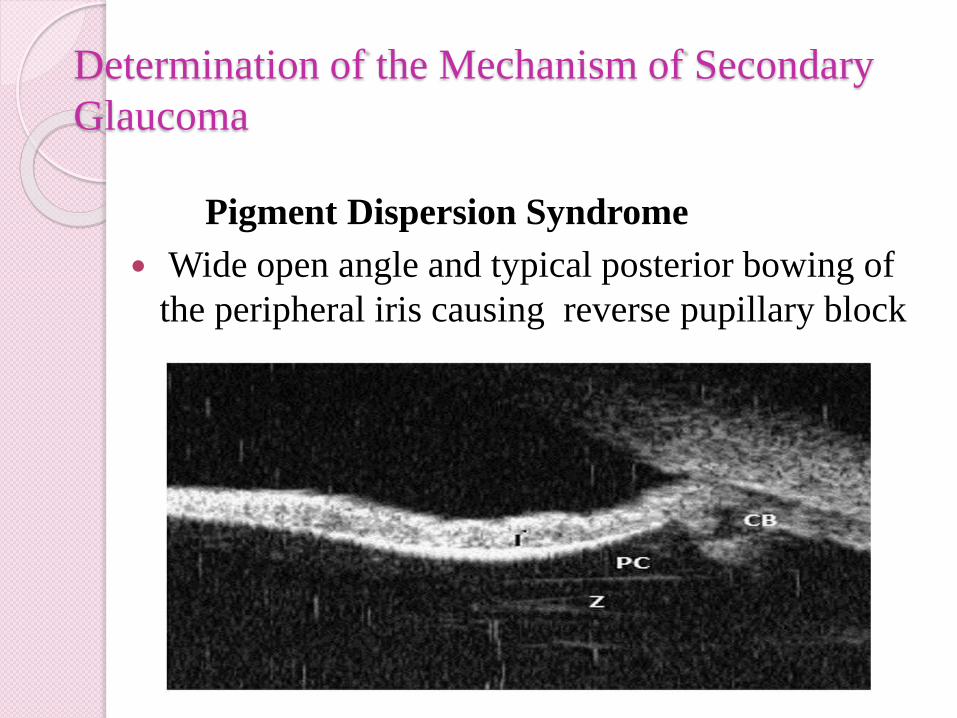
Determination of the Mechanism of Secondary
Glaucoma
Pigment Dispersion Syndrome
Wide open angle and typical posterior bowing of
the peripheral iris causing reverse pupillary block
Plateau iris syndrome
Abnormally steep anterior angulation of the peripheral iris.
Anterior insertion of the iris on to the anterior ciliary body.
Can also confirm the double hump sign by use of indentation UBM, a special technique that applies mild pressure on peripheral cornea with the skirt of the eyecup.
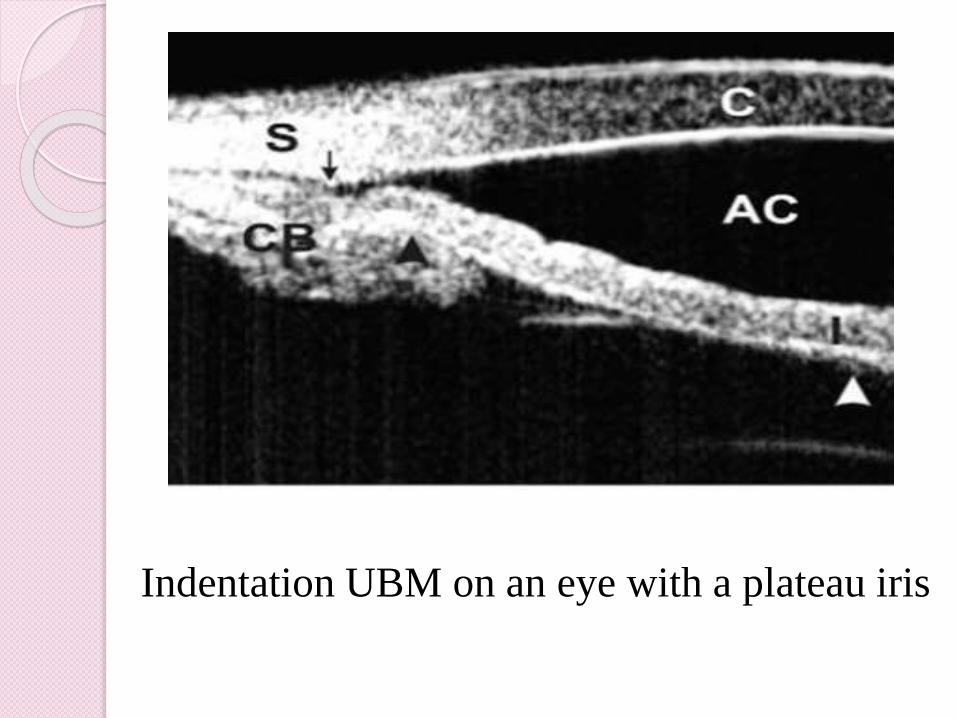
Indentation UBM on an eye with a plateau iris
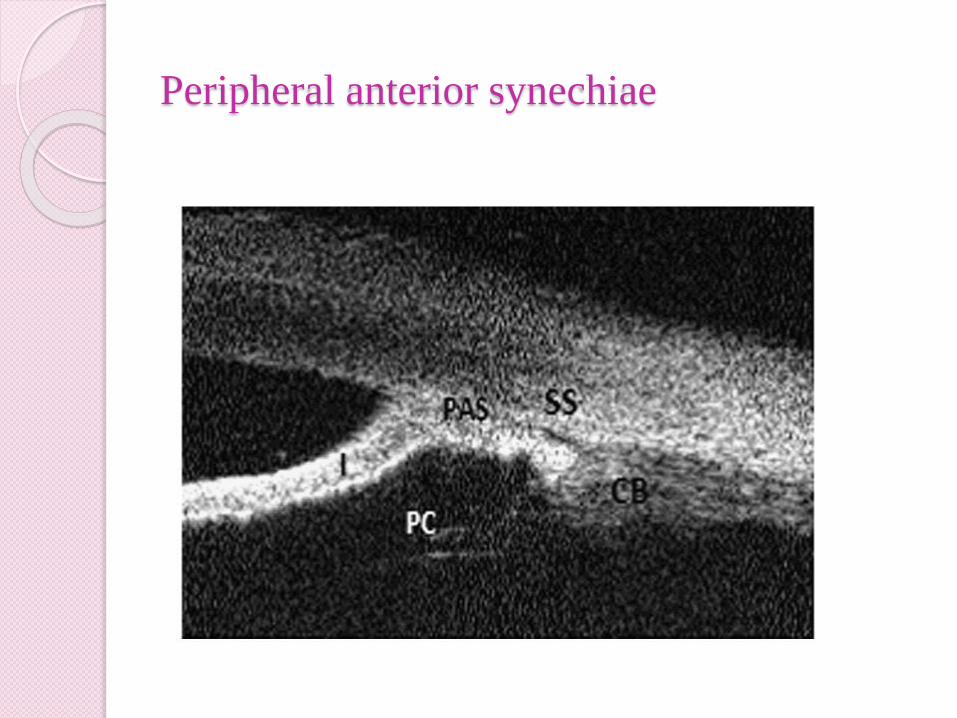
Peripheral anterior synechiae
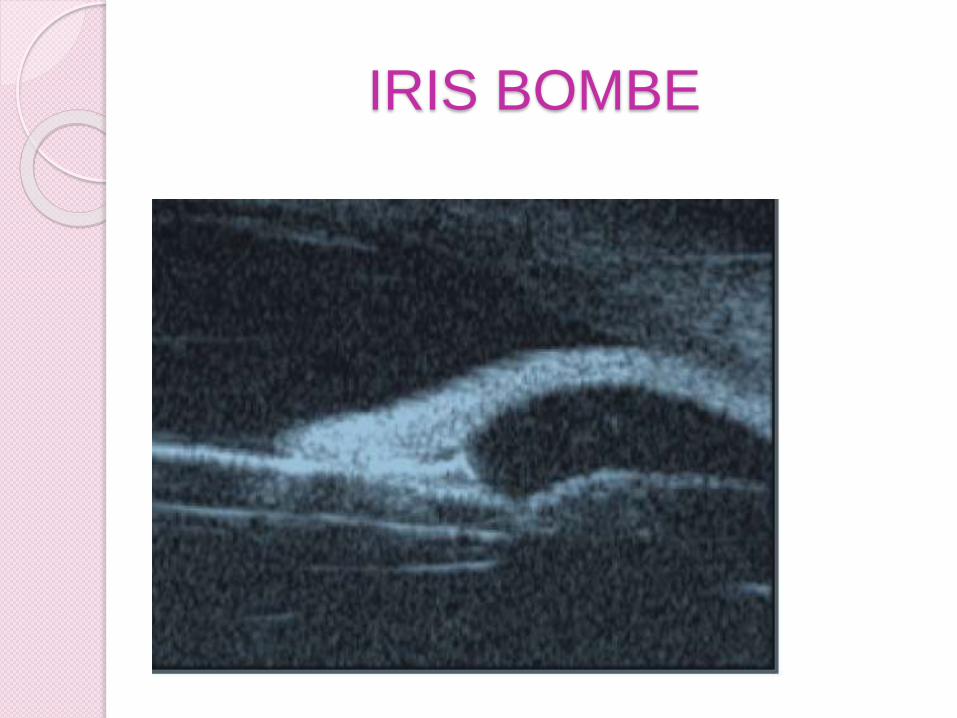
IRIS BOMBE
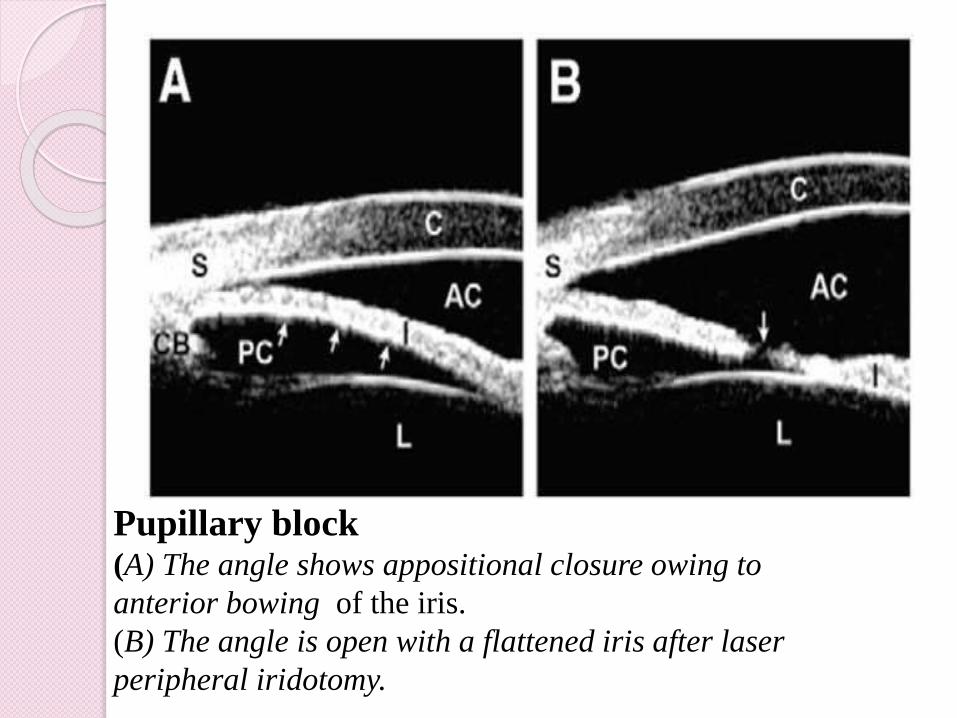
Pupillary block(A) The angle shows appositional closure owing to
anterior bowing of the iris.
(B) The angle is open with a flattened iris after laser
peripheral iridotomy.
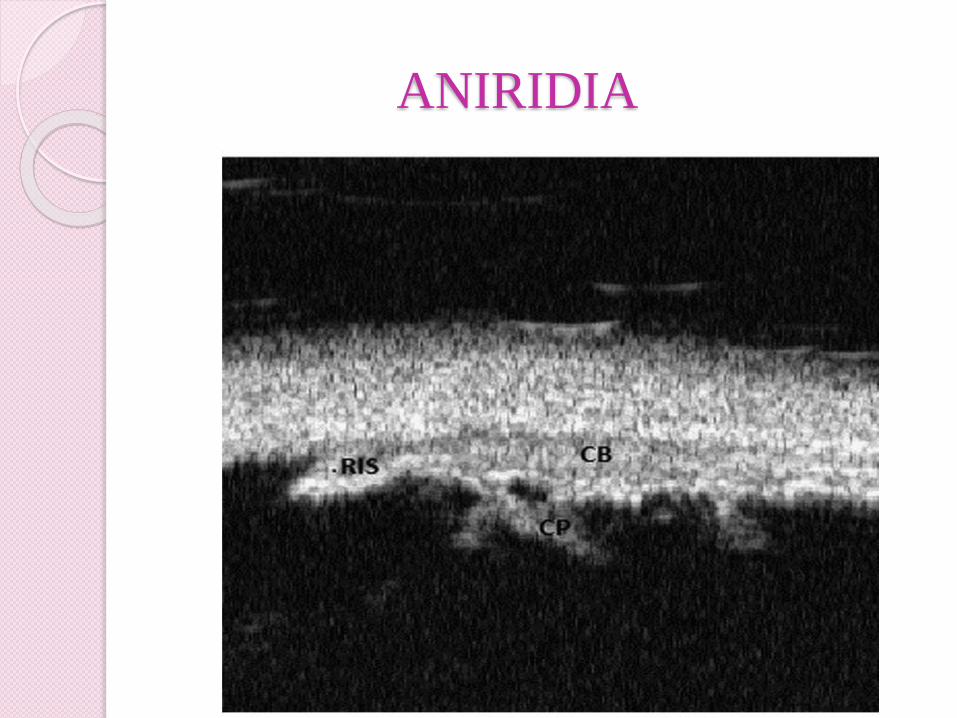
ANIRIDIA
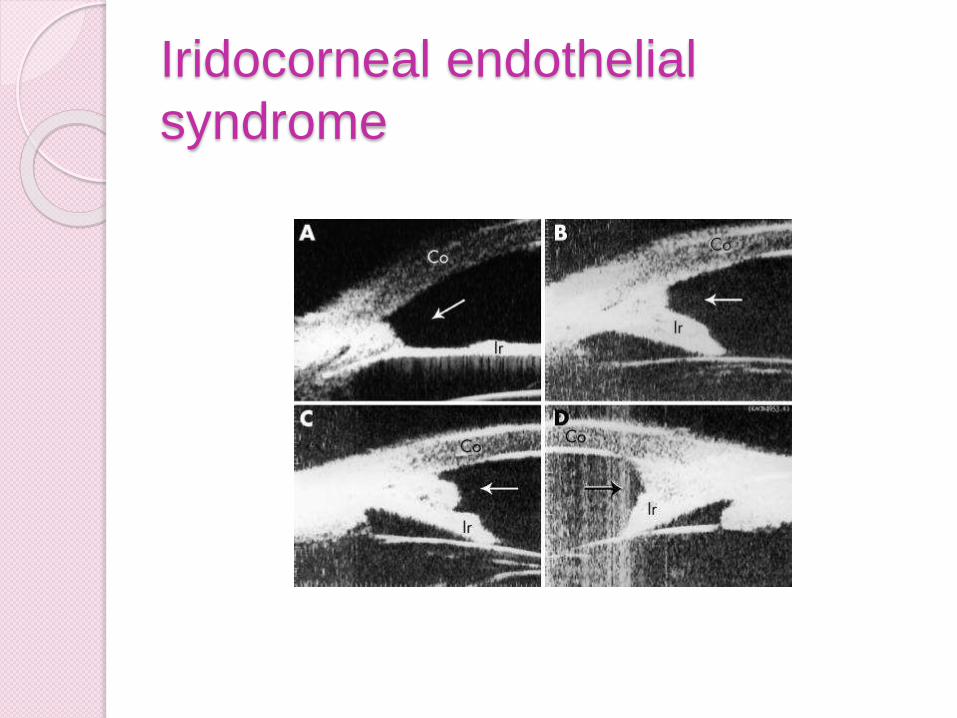
Iridocorneal endothelial
syndrome
Congenital glaucoma
Common features-
thin stretched out ciliary body,
abnormal tissue at the iridocorneal angle,
abnormal insertion of the ciliary body
In cases of cloudy cornea and unknown previous
glaucoma surgery, UBM can be used to identify
the type and localization of previous surgery in
congenital glaucoma, thus assisting surgical
planning for subsequent management
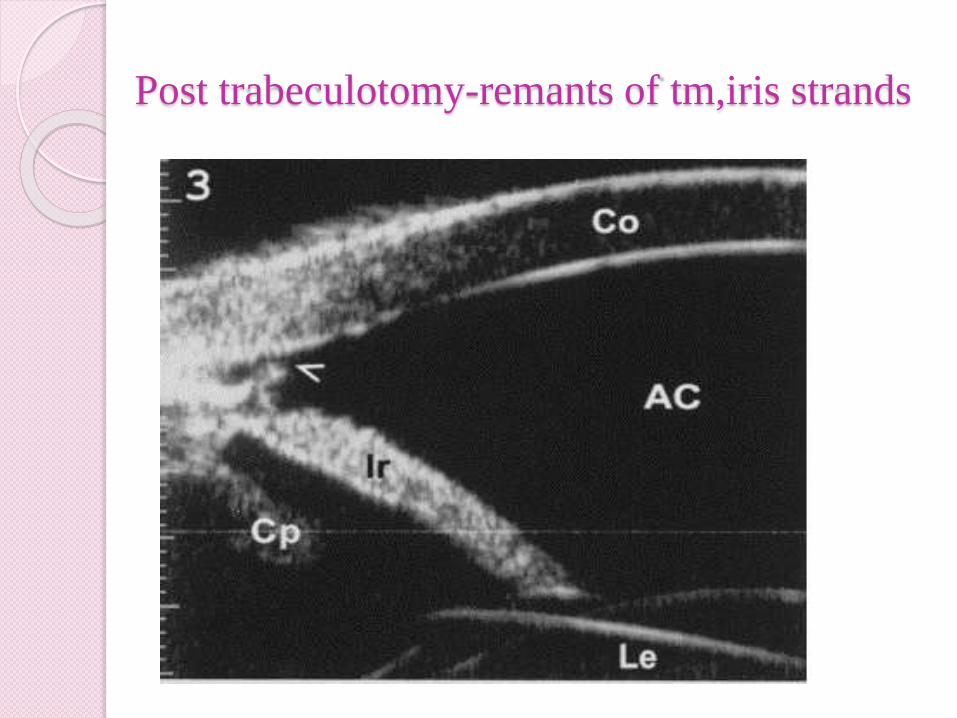
Post trabeculotomy-remants of tm,iris strands
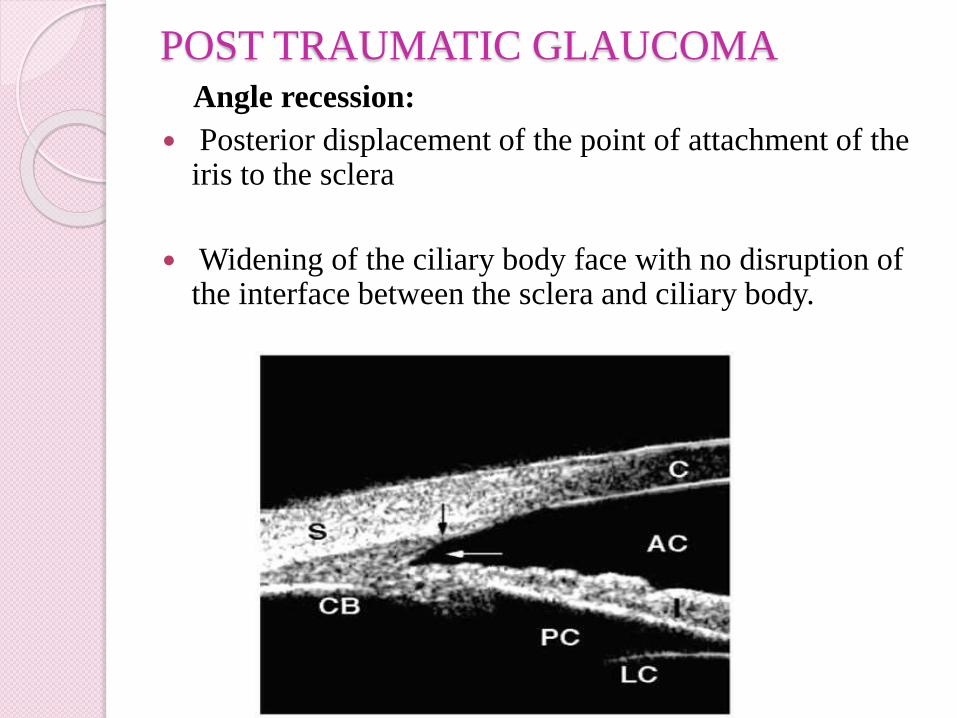
POST TRAUMATIC GLAUCOMAAngle recession:
Posterior displacement of the point of attachment of the iris to the sclera
Widening of the ciliary body face with no disruption of the interface between the sclera and ciliary body.
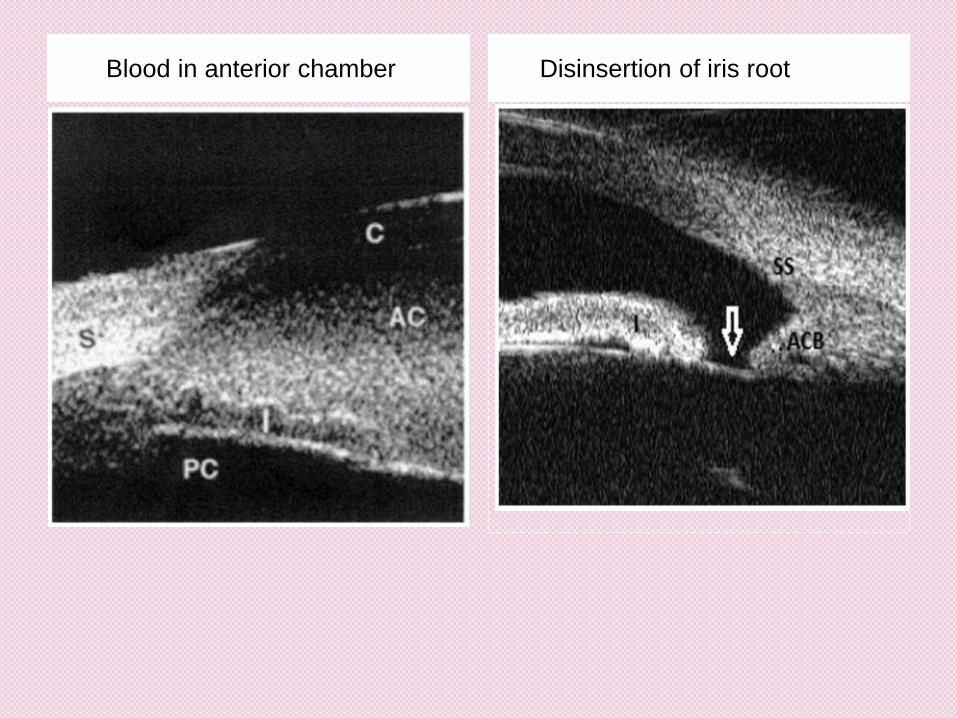
Blood in anterior chamber Disinsertion of iris root
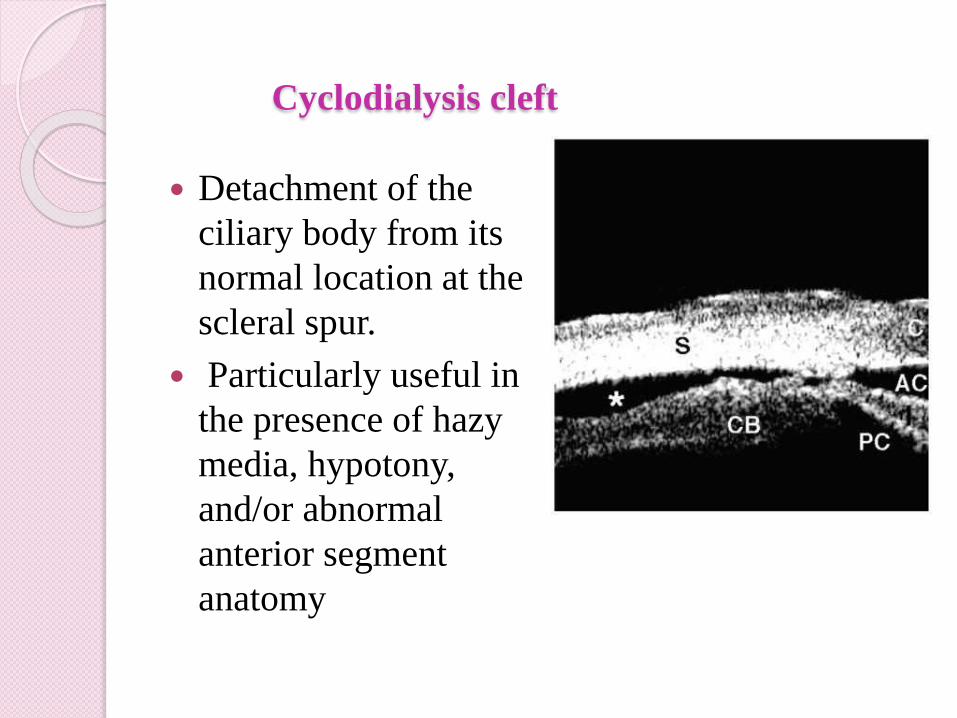
Cyclodialysis cleft
Detachment of the
ciliary body from its
normal location at the
scleral spur.
Particularly useful in
the presence of hazy
media, hypotony,
and/or abnormal
anterior segment
anatomy
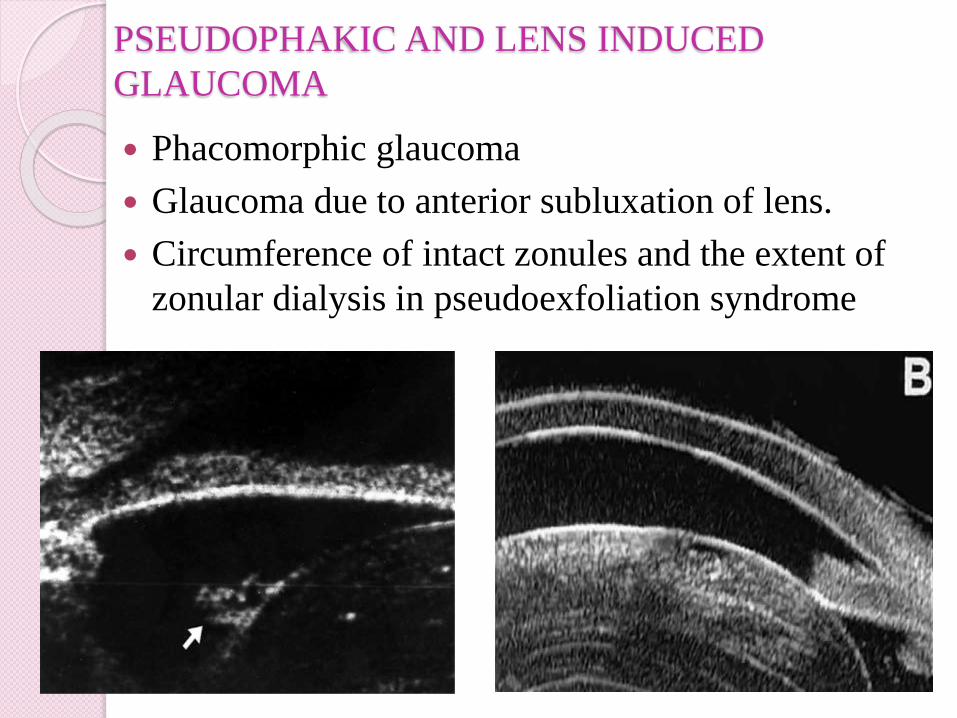
PSEUDOPHAKIC AND LENS INDUCED
GLAUCOMA
Phacomorphic glaucoma
Glaucoma due to anterior subluxation of lens.
Circumference of intact zonules and the extent of
zonular dialysis in pseudoexfoliation syndrome
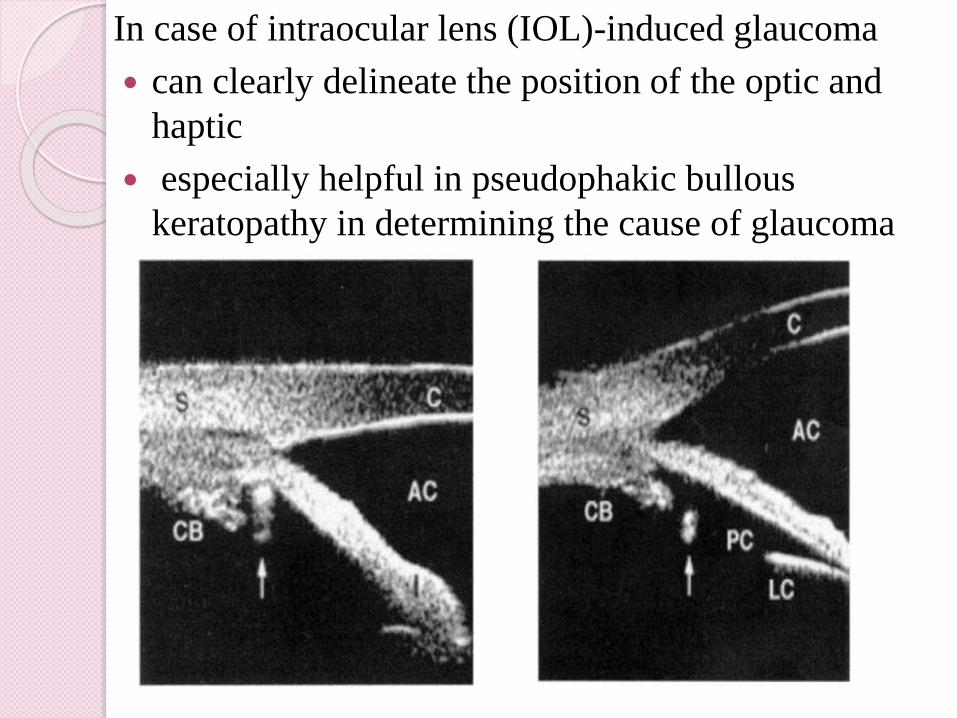
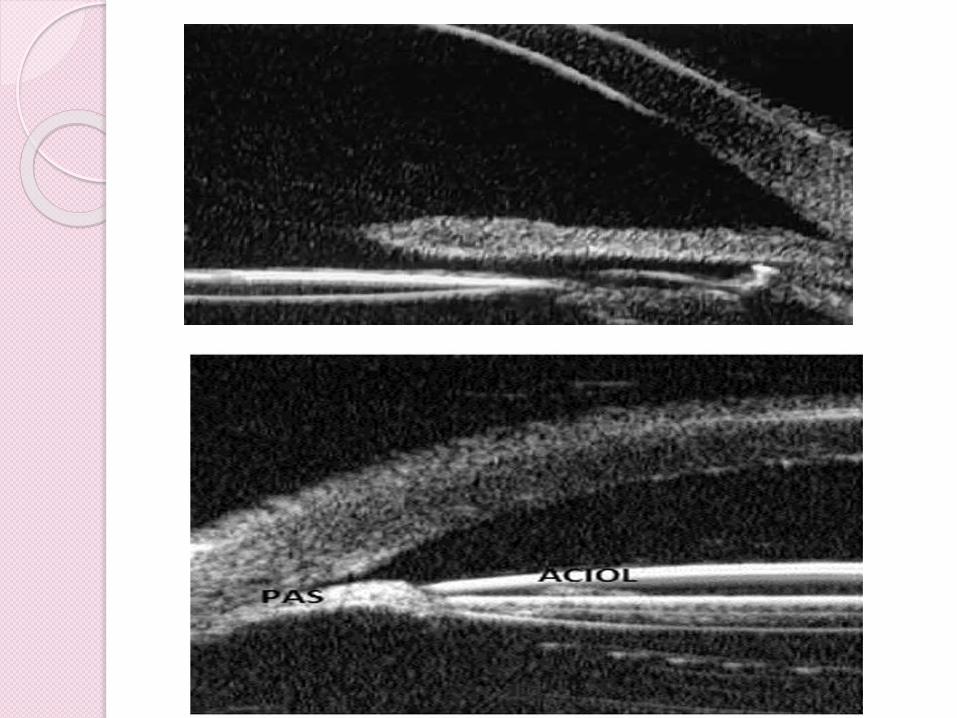
In case of intraocular lens (IOL)-induced glaucoma
can clearly delineate the position of the optic and
haptic
especially helpful in pseudophakic bullous
keratopathy in determining the cause of glaucoma
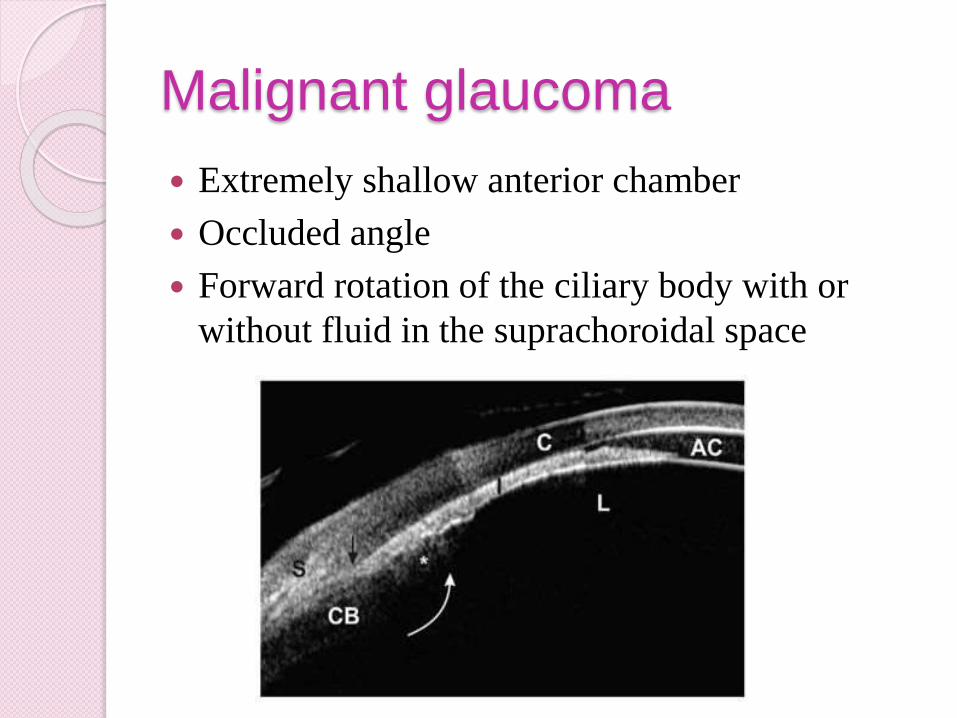
Malignant glaucoma
Extremely shallow anterior chamber
Occluded angle
Forward rotation of the ciliary body with or
without fluid in the suprachoroidal space
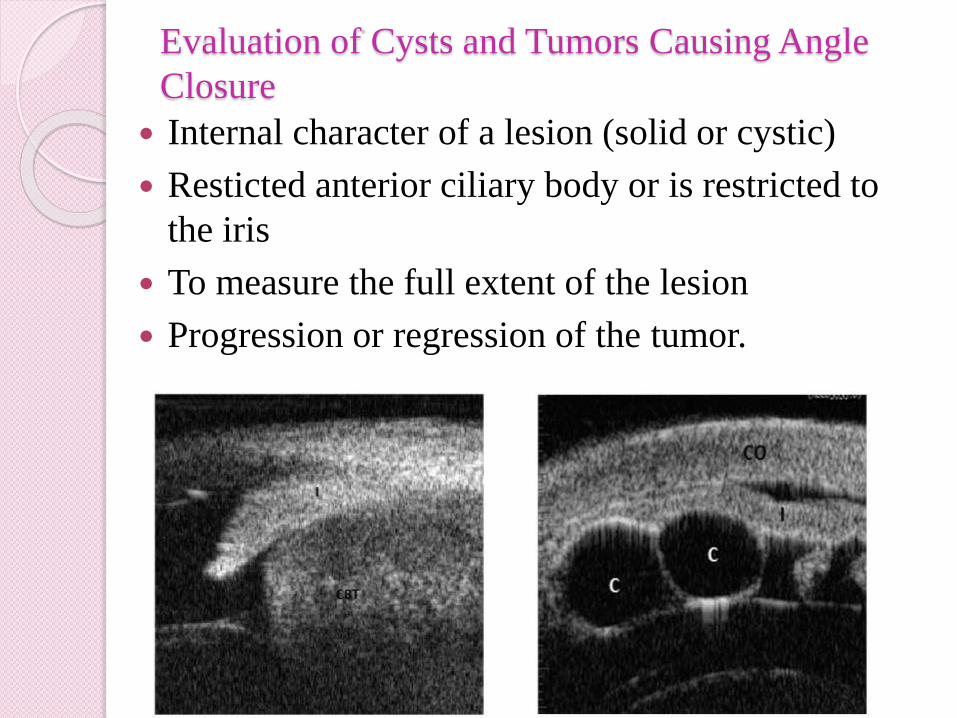
Evaluation of Cysts and Tumors Causing Angle
Closure
Internal character of a lesion (solid or cystic)
Resticted anterior ciliary body or is restricted to
the iris
To measure the full extent of the lesion
Progression or regression of the tumor.
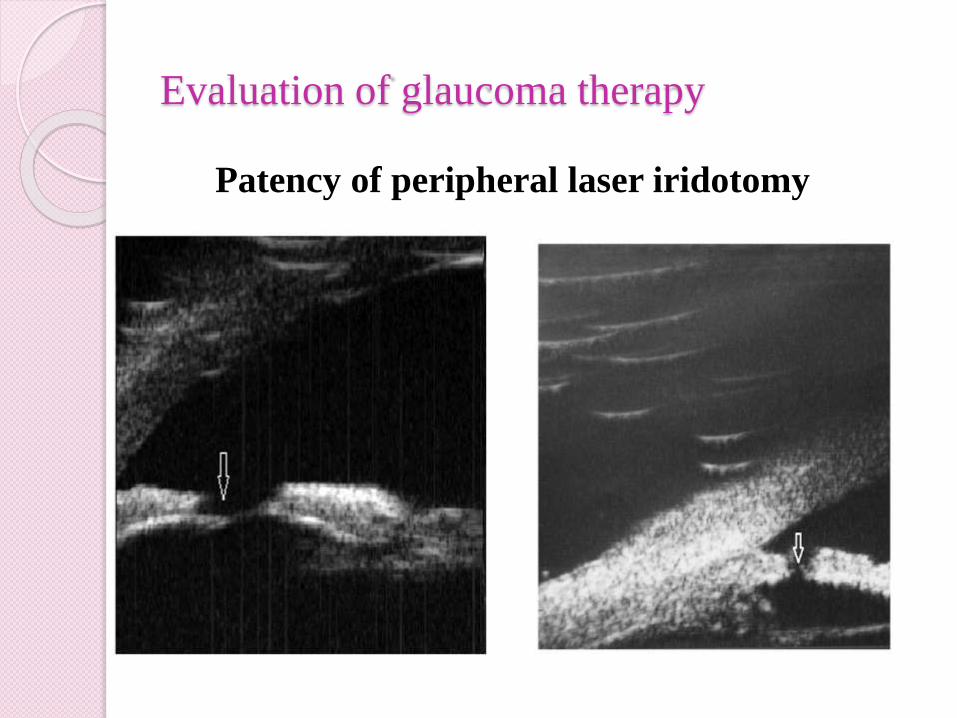
Evaluation of glaucoma therapy
Patency of peripheral laser iridotomy
Determining Functional Status of a Filtering Surgery
After trabeculectomy-
Patency of sclerostomy aperture
Patency of peripheral iridectomy
Filtering bleb - flat, shallow, or deep
The grading of the bleb is done according to
intrableb reflectivity, visibility of the route under
the scleral flap, formation of cavernous fluid filled
space, and bleb height.
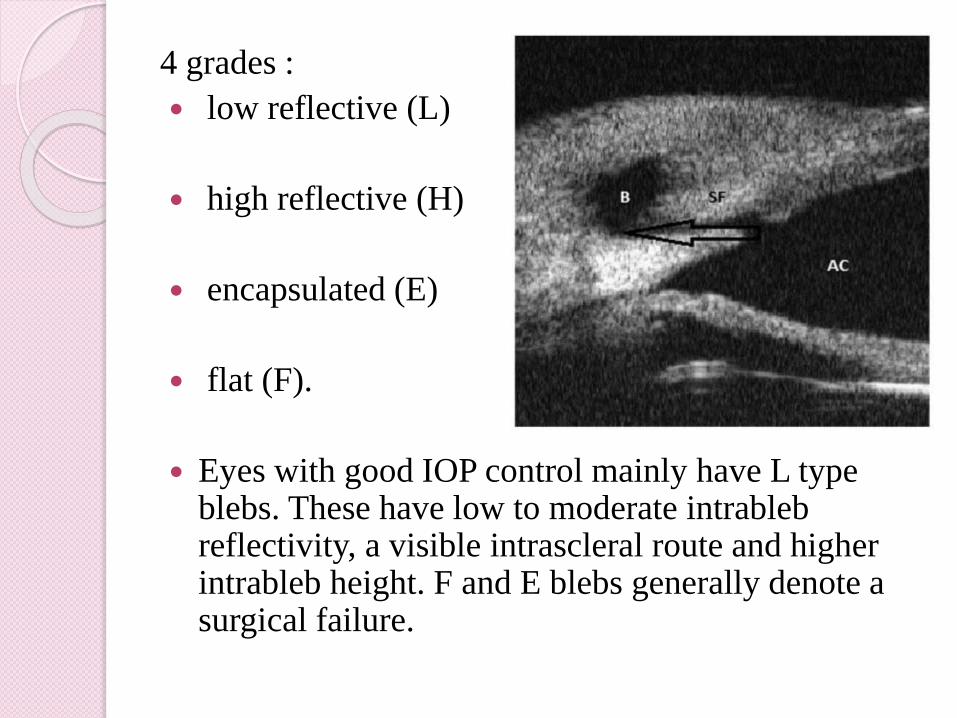
4 grades :
low reflective (L)
high reflective (H)
encapsulated (E)
flat (F).
Eyes with good IOP control mainly have L type blebs. These have low to moderate intrablebreflectivity, a visible intrascleral route and higher intrableb height. F and E blebs generally denote a surgical failure.
Non-penetrating Deep Sclerectomy
Evaluate the functional status of the surgery
Can evaluate the thickness and demonstrate a non-perforated continuous trabeculum and Descemets membrane.
UBM examination after long-term follow-up shows the presence of an intrascleral space and a filtering bleb. Collagen implants used to augment deep sclerectomy can also be visualized.
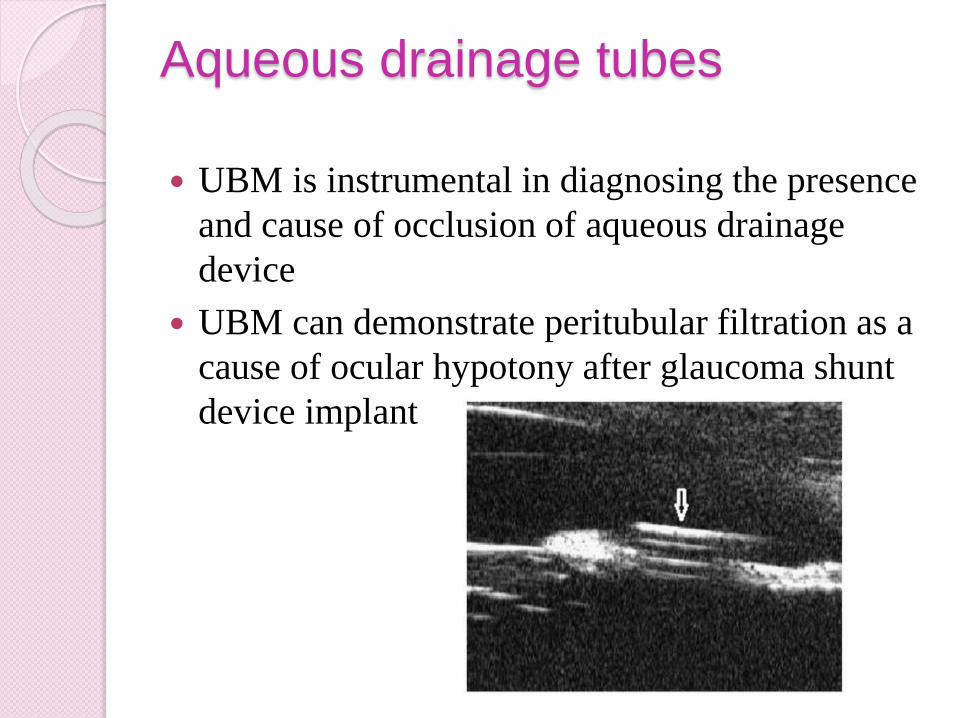
Aqueous drainage tubes
UBM is instrumental in diagnosing the presence
and cause of occlusion of aqueous drainage
device
UBM can demonstrate peritubular filtration as a
cause of ocular hypotony after glaucoma shunt
device implant
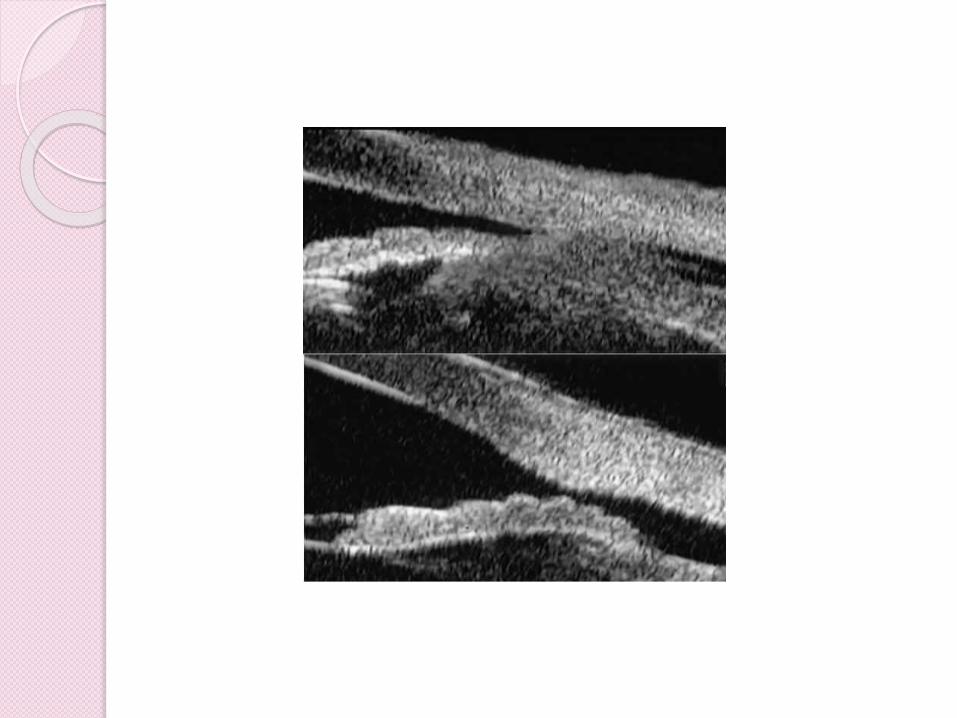
Evaluation of Postoperative Complications after
Trabeculectomy
UBM can be used to detect and evaluate the extent of
postoperative complications such as ciliochoroidal
effusion and cyclodialysis.
In ciliochoroidal effusion UBM shows the ciliary
body to be edematous and separated from the sclera
by a sonolucent collection of supraciliary fluid
UVEITIC GLAUCOMA
Uveitis, especially pars planitis, is also an
important cause of glaucoma.
Greiner et al used UBM to grade pars
planitis as follows:
grade 0 = no cells
grade 1 = mild cells
grade 2 = marked cells
grade 3 = organization of cells.
EVALUATION OF SUCCESS OF CILIO-
DESTRUCTIVE PROCEDURE
UBM has been used to image early and late
ciliary body alterations after trans scleral
cyclophotocoagulation
to establish the position of the ciliary body to
ensure correct laser probe placement
to locate ciliary body residuals for retreatment,
and to rule out scleral damage after the
procedure.
CONCLUSIONS
An indispensable tool in qualitative and
quantitative assesment of anterior segment.
an excellent view of the pathology occurring in
the anterior and posterior chambers of the eye
and thereby providing a clear insight into the
cause of aqueous obstruction.