Embed Size (px)
Citation preview

The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute
Updates on Colorectal Cancer 2015 Christina Wu, MD Division of Medical Oncology Section of Gastrointestinal Cancers
Prognostic factors KRAS/BRAF mutations in Stage III colon cancer Vitamin D levels in metastatic colorectal cancer
Therapies TAS-102 Ramucirumab SIRT and chemotherapy
New targets PD-1 inhibition in dMMR colorectal cancer HER2 targeting in colorectal cancer
Outline

Prognostic factors
3

Prognostic value of BRAFV600E and KRAS exon 2 mutations in microsatellite stable, stage III colon cancer patients treated with adjuvant FOLFOX+/-
cetuximab.
A pooled analysis of 3934 patients from the PETACC8 and N0147 trials.
Julien Taieb, Karine Le Malicot, Qian Shi, Frédérique Penault Lorca, Olivier Bouché, Stephen N. Thibodeau, Josep Tabernero, Enrico Mini, Richard M. Goldberg , Gunnar
Folprecht, Jean-Luc Van Laethem, Jean-François Emile, Daniel Sargent, Steven Alberts, Pierre Laurent-Puig, Frank A. Sinicrope
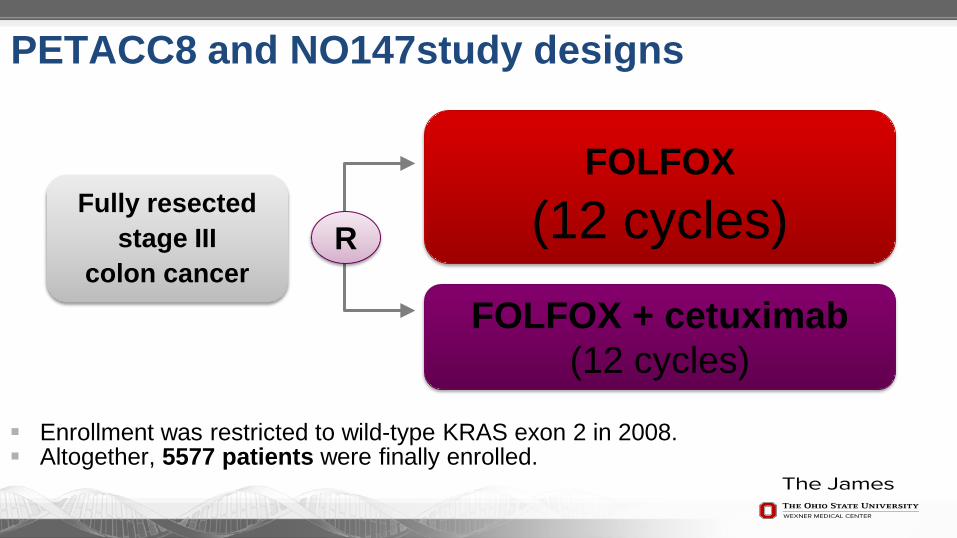
Enrollment was restricted to wild-type KRAS exon 2 in 2008. Altogether, 5577 patients were finally enrolled.
PETACC8 and NO147study designs
Fully resected stage III
colon cancer
FOLFOX (12 cycles)
FOLFOX + cetuximab (12 cycles)
R

KRAS exon 2 and BRAFV600E mutations in patients with MSS tumors (n=3934)

Time to Recurrence: KRAS exon 2 and BRAF mutational status
HR for TTR [95% CI] p-value (log-rank)
BRAF 1.49 [1.19; 1.87] 0.0005
KRAS exon 2
1.60 [1.60; 1.83] <0.0001
69%
70%
80%

Overall Survival: KRAS exon 2 and BRAF mutational status
74%
86%
91%
HR for OS [95% CI] p-value (log-rank)
BRAF 1.72 [1.33; 2.22] <0.0001
KRAS exon 2 1.52 [1.29; 1.79] <0.0001

1.0 2.09 2.57 years
Survival after recurrence regarding KRAS exon 2 and BRAF mutational status

Summary: Patients with KRAS and BRAF mutations do worse because
of BOTH earlier recurrences and worse survival after recurrence
We should probably NOT yet routinely test for these mutations in the stage 3 population No evidence “something more” is better (ie FOLFOXIRI)
However, future adjuvant trials can utilize as stratification factor
Current “high-risk” stage 3 proposal can consider both KRAS and BRAF mutation patients for inclusion

Kimmie Ng, Alan P. Venook, Kaori Sato, Chen Yuan, Bruce W. Hollis, Donna Niedzwiecki, Cynthia Ye, I-Wen Chang, Bert H. O’Neil, Federico Innocenti, Heinz-Josef Lenz, Charles D. Blanke, Robert J. Mayer, Charles S. Fuchs, Jeffrey A. Meyerhardt
Vitamin D Status and Survival of Metastatic Colorectal Cancer Patients: Results from
CALGB/SWOG 80405 (Alliance)
1Dana-Farber Cancer Institute, 2University of California San Francisco, 3Medical University of South Carolina, 4Alliance Statistics and Data Center, 5Wayne Memorial Hospital, 6Indiana University Hospital, 7University of North Carolina at Chapel Hill,
8University of Southern California, 9Oregon Health and Science University

CALGB/SWOG 80405: Original Design
n = 1140 1° Endpoint: Overall Survival
Chemo + Cetuximab
Chemo + Bevacizumab
mCRC 1st-line
KRAS wild type (codons 12,13)
Strata:
•FOLFOX/FOLFIRI •Prior adjuvant chemo •Prior XRT
FOLFIRI or
FOLFOX
MD choice Chemo + Bevacizumab and
Cetuximab
2334

Study Cohort Randomized
(n=2,334)
Bevacizumab (n=899)
Cetuximab (n=902)
Both (n=533)
RAS WT (n=256)
RAS mutant (n=167)
Unknown (n=476)
Plasma 25(OH)D Available (n=1,043)
n=172 n=126 n=123
RAS WT (n=270)
RAS mutant (n=180)
Unknown (n=452)
n=173 n=121 n=124
RAS WT (n=0)
RAS mutant (n=124)
Unknown (n=409)
n=0 n=62 n=142

Higher Vitamin D Levels Associated with Better Survival
417 328 227 117 56 27 5 1 418 332 237 125 64 34 11 2 208 171 137 76 41 22 1
Quintiles 1 & 2 Quintiles 3 & 4
Quintile 5
No. at Risk
0
0.0
0.2
0.4
0.6
0.8
1.0
0 1 2 3 4 5 6 7 Time (years)
Ove
rall
Surv
ival
Pro
babi
lity
Log-rank P = 0.01
Quintile
5
3 2
mOS (months)
30.0 28.4
32.6
1 24.5
95% CI
21.7-28.6
4 27.2
25.8-32.2 24.2-31.0 25.0-31.5 27.7-36.9

Multivariate Hazard Ratios: Overall Survival
1.0 0.83
[0.66 – 1.03] 0.81
[0.65 – 1.02]
0.65 [0.51 – 0.83]
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1
2.2 – 10.8 10.9 – 15.4 15.5 – 19.2 > 24.1
Haz
ard
Rat
io fo
r Dea
th
P trend = 0.001
Plasma 25(OH)D (ng/mL)
Pa ti e n ts w i th th e h i g h e s t l e v e l s o f v i ta m i n D h a v e
a 3 5 % i m p r o v e m e n t in overall survival
19.3 – 24.0
0.79 [0.63 – 1.00]

Multivariate Hazard Ratios: PFS
1.0 0.99 [0.80 – 1.23]
0.84 [0.67 – 1.05] 0.79
[0.63 – 0.99]
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1
2.2 – 10.8 10.9 – 15.4 15.5 – 19.2 > 24.1
Haz
ard
Rat
io fo
r Pro
gres
sion
or D
eath
P trend = 0.01
Plasma 25(OH)D (ng/mL)
Pa ti e n ts w i th th e h i g h e s t l e v e l s o f v i ta m i n D h a v e
a 2 1 % i m p r o v e m e n t i n PF S
19.3 – 24.0
0.83 [0.67– 1.04]

Randomized Double-Blind Phase II Trial of Vitamin D in Metastatic CRC
Participating Sites: DFCI MGH BIDMC DF/HCC satellites DF/HCC affiliates Northwestern Vanderbilt MSTI (Boise, ID)

“Easy to do” Can be readily modified Many PCPs already doing this Our patients will ask!
Should we be checking Vitamin D levels?
PRO CON If only a prognostic factor,
is it worth knowing? Will modifying it be helpful?

New therapies
19

SIRFLOX: Randomized phase III trial comparing first-line mFOLFOX6 (+bevacizumab) versus mFOLFOX6
(+bevacizumab) + selective internal radiation therapy (SIRT) in patients with metastatic colorectal cancer
Peter Gibbs, Volker Heinemann, Navesh K. Sharma, Michael P. N. Findlay, Jens Ricke, Val Gebski,
Mark Van Buskirk, Guy A. Van Hazel, on behalf of the SIRFLOX Study Group
The Royal Melbourne Hospital, Melbourne, Australia
*SIRT= radioembolization

Study Design
SIRT
Design: Prospective open-label RCT Primary endpoint: Progression-Free Survival Survival
Stratified by •Presence of extra- hepatic metastases •Degree of liver involvement •Intended use of bevacizumab •Institution
Randomized 1:1
n = 530
mFOLFOX6 (+ bevacizumab) (1)
SIRT
n = 263 enrolled
n = 267 enrolled
Eligible Patients •Non-resectable liver-only or liver-dominant mCRC •No prior chemo for advanced disease •WHO performance status 0–1
ANZ: 280 (53%) EME: 191 (36%) US: 59 (11%)
1. Bevacizumab allowed at investigator’s discretion, per institutional practice
mFOLFOX6 (+ bevacizumab) (1)
ANZ: Australia, New Zealand; AP: Asia Pacific; EME: Europe & Middle East; US: United States
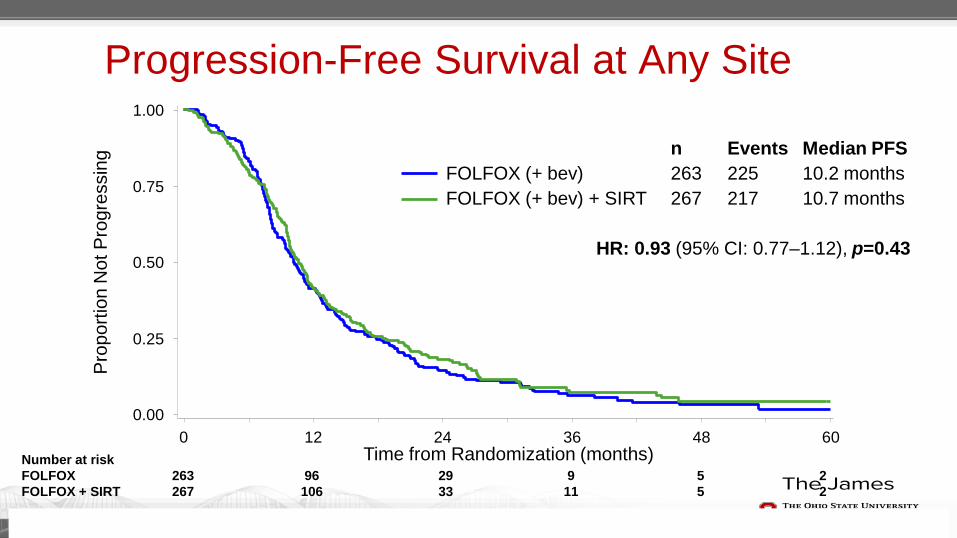
Progression-Free Survival at Any Site
Number at risk FOLFOX 263 96 29 9 5 2 FOLFOX + SIRT 267 106 33 11 5 2
n Events Median PFS FOLFOX (+ bev) 263 225 10.2 months FOLFOX (+ bev) + SIRT 267 217 10.7 months HR: 0.93 (95% CI: 0.77–1.12), p=0.43
0.00
0.25
0.50
0.75
1.00
0 12 24 36 48 60
Pro
porti
on N
ot P
rogr
essi
ng
Time from Randomization (months)

PFS in the Liver: Competing Risk Analysis
Number at risk FOLFOX 263 96 29 9 FOLFOX + SIRT 267 106 33 11
Pro
babi
lity
of H
epat
ic P
rogr
essi
on
0 12 24 36 48 60 0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
n Events Median FOLFOX (+ bev) 263 215 12.6 months FOLFOX (+ bev) + SIRT 267 215 20.5 months HR: 0.69 (95% CI: 0.55–0.90); p=0.002 †
Time from Randomization (months)

Site of First Progression Liver-Only Metastases at Baseline Extra-Hepatic Metastases at Baseline
FOLFOX (+ bev)
FOLFOX (+ bev) + SIRT
Prop
ortio
n w
ith
Prog
ress
ion
Site of First Progression
What has limited medical oncologists’ use of SIRT for mCRC?
Availability Concerns for toxicity Early and late in patients who will live 2-3 years Thus has relegated to “nth”-line when typically used In SIRFLOX, incidence of liver-injury quite low
Unclear efficacy benefit No survival data reported in SIRFLOX No PFS benefit Liver PFS benefit
May translate to overall survival benefit if patients destined to die of liver failure from mCRC are selected (40% in SIRFLOX with extrahepatic disease)

For the clinic SIRT has been variably used Intriguing initial report of the first LARGE, randomized trial Improvement in liver PFS intriguing
?perhaps best in liver-only patients Probably not the time to begin using routinely with front-line
chemotherapy However, may have particular niche for liver-only patients in whom
“aggressive” therapy is desirable If planned analyses with other trials shows survival benefit in a
subpopulation…may have much greater impact!

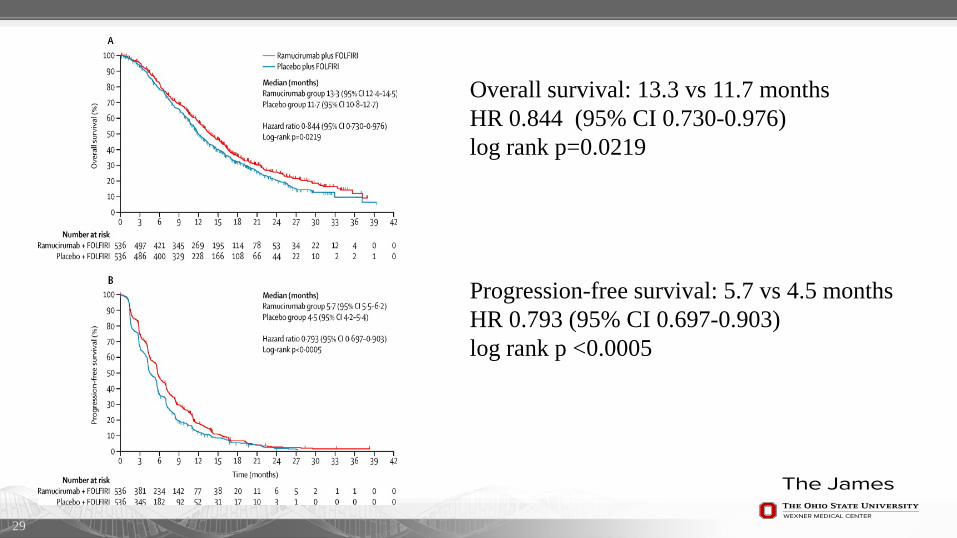
Ramucirumab versus placebo in combination with second-line FOLFIRI in patients with metastatic colorectal
carcinoma that progressed during or after first-line therapy with bevacizumab, oxaliplatin, and a fluoropyrimidine
(RAISE): a randomised, double-blind, multi-centre, phase 3 study.
27
Josep Tabernero, Takayuki Yoshino, Allen Lee Cohn, Radka Obermannova, Gyorgy Bodoky, Rocio Garcia-Carbonero, Tudor-Eliade Ciuleanu, David C Portnoy, Eric Van Cutsem, Axel
Grothey, Jana Prausova, Pilar Garcia-Alfonso, Kentaro Yamazaki, Philip R Clingan, Sara Lonardi, Tae Won Kim, Lorinda Simms, Shao-Chun Chang, Frederico Nasroulah, and the RAISE Study
Investigators

Study design
Tabernero et al, Lancet Oncol 2015;16:499-508.
1072 mCRC patients Progressed on 1st line
therapy with FOLFOX +
bevacizumab
FOLFIRI + placebo
FOLFIRI + ramucirumab (8mg/kg)
1:1
29
Overall survival: 13.3 vs 11.7 months HR 0.844 (95% CI 0.730-0.976) log rank p=0.0219 Progression-free survival: 5.7 vs 4.5 months HR 0.793 (95% CI 0.697-0.903) log rank p <0.0005
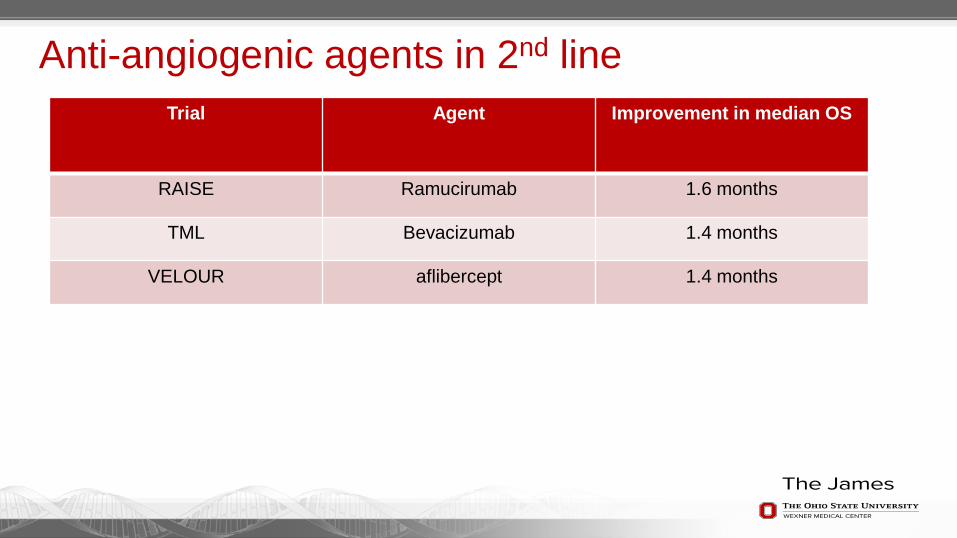
Anti-angiogenic agents in 2nd line Trial Agent Improvement in median OS
RAISE Ramucirumab 1.6 months
TML Bevacizumab 1.4 months
VELOUR aflibercept 1.4 months

Randomized Trial of TAS-102 for Refractory Metastatic Colorectal Cancer
Robert J Mayer, Eric Van Cutsem, Alfredo Falcone, Takayuki Yoshino, Rocio Garcia Carbonero, Nobuyuki Mizunuma, Kentaro Yamazaki, Yasuhiro Shimada, Josep
Tabernero, Yoshito Komatsu, Alberto Sobrero, Eveline Boucher, Marc Peeters, Ben Tran, Heinz-Josef Lenz, Alberto Zaniboni, Howard Hochster, James M Cleary, Lukas
Makris, Masanobu Ito, and Atsushi Ohtsu for the RECOURSE study Group
Mayer RJ et al. N Engl J Med 2015;372-1909-19.

F3dTMP (inactive form) TPI
TPase
F3dTDP
FTD incorporation into DNA
F3dTTP
F3dThd (FTD) Thymidine-based nucleoside analogue
DNA dysfunction
Inhibition of tumor growth
FTD:Trifluridine TPI:Tipiracil-HCl
TAS-102; Mechanism of Action
FTD TPI
TAS-102 (Oral Combination Drug)
Molar ratio = 1 : 0.5
FTY

TS
5-FU FdUM
P
dUMP dTMP
dTTP
Differentiation between 5-FU and TAS-102
FTD Thymidine(T)
T
T
Inhibit
FTD
F3dTDP F3dTTP
F3dTMP Phosphorylation
DNA duplication
DNA damage
5-FU
Incorporation into DNA
TAS-102
Inhibit DNA duplication

Global Randomized Phase III study RECOURSE: Refractory Colorectal Cancer Study (NCT01607957)
• Stratification: KRAS status, time from diagnosis of metastatic disease, geographical region • Sites: 13 countries, 114 sites • Enrollment: June 2012 to October 2013
R A N D O M I Z A T I O N
Metastatic colorectal cancer (mCRC) • 2 or more prior regimens • Refractory / Intolerable
– fluoropyrimidine – irinotecan – oxaliplatin – bevacizumab – anti-EGFR if wild-type KRAS
• ECOG PS 0-1 • Age ≥ 18 (target sample size: 800)
TAS-102 + BSC (n = 534)
35 mg/m2 b.i.d. p.o. d1-5, 8-12 q4wks
Placebo + BSC (n = 266)
d1-5, 8-12 q4wks
Endpoints Primary: OS Secondary: PFS, Safety,
Tolerability, TTF, ORR, DCR, DoR, Subgroup by KRAS (OS
and PFS)
2:1

Overall Survival TAS-102 N=534
Placebo N=266
Events # (%) 364 (68) 210 (79) HR (95% CI) 0.68 (0.58-0.81)
Stratified Log-rank test p<0.0001 Median OS, months 7.1 5.3
Median follow-up (censored pts): 8.3 months
Alive at, %
6 months 58 44 12 months 27 18
TAS-102 534 459 294 137 64 23 7 Placebo 266 198 107 47 24 9 3
N at Risk: Months from Randomization
0 3 6 9 12 15 18
Surv
ival
Dis
trib
utio
n fu
nctio
n
0
10
20
30
40
50
60
70
80
90
100

Progression-free Survival TAS-102 N=534
Placebo N=266
Events # (%) 472 (88) 251 (94) HR (95% CI) 0.48 (0.41-0.57)
Stratified Log-rank test p<0.0001 Median PFS, months 2.0 1.7
Tumor assessments performed every 8 weeks
TAS-102 534 238 121 66 30 18 5 4 2 Placebo 266 51 10 2 2 2 1 1 0
N at Risk: Months from Randomization 0 2 4 6 8 10 12 14 16
Prog
ress
ion-
free
Dis
trib
utio
n fu
nctio
n
0
10
20
30
40
50
60
70
80
90
100

Non-Hematologic Adverse Events Occurring in >10% of Patients (as-treated population)
Non-Hema Adverse events, % TAS-102 (N=533) Placebo (N=265) All Gr. Gr. 3 Gr. 4 All Gr. Gr. 3 Gr. 4
Nausea 48.4 1.9 0 23.8 1.1 0 Decreased appetite 39.0 3.6 0 29.4 4.9 0 Fatigue 35.3 3.9 0 23.4 5.7 0 Diarrhea 31.9 2.8 0.2 12.5 0.4 0 Vomiting 27.8 2.1 0 14.3 0.4 0 Pyrexia 18.4 0.9 0.2 14.0 0.4 0 Asthenia 18.2 3.4 0 11.3 3.0 0 Constipation 15.2 0.2 0 15.1 1.1 0 Abdominal pain 14.8 2.1 0 13.6 3.4 0 Cough 10.7 0.4 0 11.3 0.8 0 Dyspnoea 10.5 2.1 0.4 12.8 2.3 0 Oedema peripheral 9.9 0.2 0 10.2 0.8 0 Weight decreased 7.7 0 0 10.2 0 0
One treatment-related death was observed in TAS-102

Adverse Events of Special Interest (as-treated population)
Adverse events, % TAS-102 (N=533) Placebo (N=265) All Gr. Gr. 3 Gr. 4 All Gr. Gr. 3 Gr. 4
Febrile neutropenia 3.8 2.8 0.9 0 0 0 Stomatitis 7.9 0.4 0 6.0 0 0 Hand-foot syndrome 2.3 0 0 2.3 0 0 Alopecia 6.8 0 0 1.1 0 0 Proteinurea 4.1 0 0 1.9 0 0
Cardiac ischaemia events, % 0.4 0.2 0 0.4 0 0.4 Thromboembolic events, % 3.9 1.7 0.2 2.3 1.1 0.4
Pulmonary embolism 1.7 1.3 0.2 0 0 0
• SAEs were observed 29.6% in TAS-102 and 33.6% in placebo • Primary reason for discontinuation due to AE was 3.6% in TAS-102 and 1.5%
in placebo

New targets
39

PD-1 Blockade in Tumors with Mismatch Repair Deficiency
Dung Le, Jennifer Uram, Hao Wang, Bjarne Bartlett, Holly Kemberling, Aleksandra Eyring, Andrew Skora, Brandon Luber, Nilofer Azad, Daniel Laheru, Barbara Biedrzycki, Ross
Donehower, Atif Zaheer, George Fisher, Todd Crocenzi, Steven Duffy, James Lee, Richard Goldberg, Albert de la Chapelle, Minori Koshiji, Feriyl Bhaijee, Thomas Huebner,
Ralph Hruban, Laura Wood, Nathan Cuka, Drew Pardoll, Nickolas Papadopoulas, Kenneth Kinzler, Shibin Zhou, Toby Cornish, Janis Taube, James Eshleman, Robert Anders, Bert
Vogelstein and Luis Diaz Jr.
Le, D et al. NEJM May 2015

Proficient mismatch repair (pMMR) = microsatellite stable (MSS) Deficient mismatch repair (dMMR) = microsatellite instable (MSI)
Detected by: IHC- missing mismatch repair proteins PCR- microsatellite instable
Present clinical use: Lynch syndrome Determine whether to offer adjuvant chemotherapy for
Stage II colon cancer patients
Mismatch repair deficiency
41

Chromosomal instability (CIN): Proficient DNA Mismatch Repair (pMMR)
and Microsatellite stable (MSS)
Microsatellite instability (MSI): Deficient Mismatch Repair (dMMR)
85% 15%
Familial cases Lynch syndrome
germline mutation: (MLH1, MSH2, MSH6, PMS2)
BRAFV600E
mutation ≈50% Sporadic cases
Epigenetic MLH1 inactivation (MLH1 promoter methylation)
Two different pathways of carcinogenesis
2/3 1/3
Sinicrope FA, Nat. Rev. Clin. Oncol. 7:174-177, 2010
No BRAFV600E
mutation

Mutations per tumor
0 500 1000 1500 2000
Mismatch repair tumors
Mutagen Associated tumors
Sporadic Adult Solid Tumors
Pediatric Tumors
Liquid Tumors
Mutations per tumor
Sporadic colon cancers
Mismatch-repair deficient colon cancers

Objective Responses MMR-deficient CRC MMR-proficient CRC MMR-deficient
non-CRC N 13 25 10
Objective Response Rate 62% 0% 60%
Disease Control Rate 92% 16% 70%
-1 0 0
-5 0
0
5 0
1 0 0M M R -p ro fic ie n t C R C
M M R -d e fic ie n t C R C
M M R -d e fic ie n t n o n -C R C
% C
han
ge
fro
m B
asel
ine
SL
D

Progression-Free Survival All Cohorts CRC Cohorts
Mismatch-repair proficient Mismatch-repair proficient
Mismatch-repair deficient Mismatch-repair deficient

Related Adverse Events
Up through Jan 2015
All Grades Grade 3 or 4Event-no. (%) N=41 N=41
Any 21 (51) 4 (10)
Generalized SymptomsFatigue 1 (2) 0
Myalgias 1 (2) 0Arthralgias 1 (2) 0
Pancreatitis/Amylasemia 1 4 (10) 3 (7)
Pneumonitis 1 (2) 0
Endocrine DisordersThyroiditis/hypothyroidism 4 (10) 0
Hypophysitis 1 (2) 0
Rash/pruritus 7 (17) 0
Thrombocytopenia 1 (2) 1 (2)

For the clinic
Although few dMMR patients, survival and response rates
are greatly improved with pembrolizumab therapy. MMR is already routinely tested in clinic Clinical trial is open and still enrolling.
1Beamer et al. J Clin Oncol 30:1058-1063, 2012.

Therapeutic Dual Inhibition of HER2 Pathway in Metastatic Colorectal Cancer
The HERACLES Trial * S. Siena1, A. Sartore-Bianchi1, L. Trusolino2,5, C. Martino2, E. Valtorta1,
S. Lonardi3, F. Leone2,5, V. Zagonel3, A. Bertotti2,5, K. Bencardino1, G. Siravegna2,5, Amatu1, A. Vanzulli1, D. Regge2, S. Ghezzi1, F. Ciardiello4, S. Veronese1,
P. M. Comoglio2,5, A.Bardelli2,5, and S. Marsoni2
1 Niguarda Cancer Center, Ospedale Niguarda Ca’ Granda, Milano, Italy; 2 Istituto di Candiolo, Fondazione Piemonte Oncologia-IRCCS, Candiolo, Italy;
3 Oncologia Medica 1, Istituto Oncologico Veneto-IRCCS, Padova, Italy; 4 Seconda Università di Napoli, Napoli; and 5 Università di Torino, Torino, Italy
* HER2 Amplification for Colo-RectaL Cancer Enhanced Stratification
EUDRACT # 2012-002128-33

lapatinib and trastuzumab
lapatinib
trastuzumab vehicle
Bertotti A. et al, Cancer Discovery 2011; Trusolino L. data on file
HER2-amplified mCRC PDX are sensitive to dual HER2-blockade with lapatinib and trastuzumab but not to single agent

Screen for HER2+ mCRC
HERACLES cohort A Trastuzumab + Lapatinib
Phase 2 with sequential cohorts design
HERACLES cohort B Trastuzumab + Pertuzumab
Define HER2 positivity in CRC (archival study + expert consensus panel) HERACLES DIAGNOSTIC CRITERIA*
HER2+ mCRC cases IHC 2+/3+ > 50% cellularity and
FISH positive
End points
• Primary: ORR by RECIST 1.1 (centralized imaging)
• Secondary: TTP, Safety
• Translational: HER2 ctDNA in plasma, HER2 ectodomain in serum, tissue and plasma NGS in de novo resistant patients and upon PD
Statistics
• Design: two sequential cohorts, phase 2 trials, A’Hern single stage for each cohort (A and B)
• Assumptions: ORR H0 10%; H1 >30%; α= 0.05; β=0.85
• Sample size: in each cohort 6 responses out of 27 to declare the study positive
HERACLES Trial Design
*Valtorta E., et al; Modern Pathology 2015 in press
Chan
ge in
targ
et le
sion
from
bas
elin
e (%
)
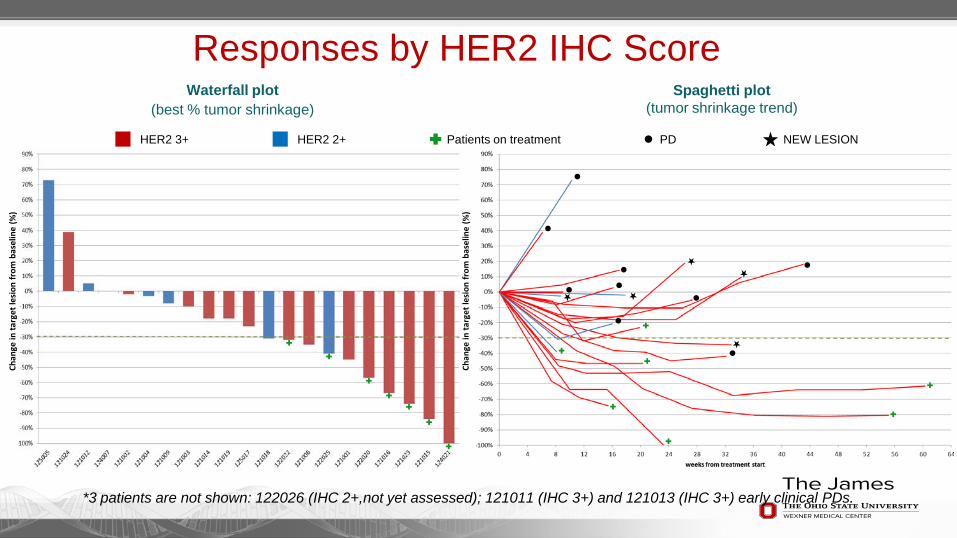
HER2 3+ HER2 2+ Patients on treatment PD NEW LESION
*3 patients are not shown: 122026 (IHC 2+,not yet assessed); 121011 (IHC 3+) and 121013 (IHC 3+) early clinical PDs.
Waterfall plot (best % tumor shrinkage)
Spaghetti plot (tumor shrinkage trend)
Chan
ge in
targ
et le
sion
from
bas
elin
e (%
)
Responses by HER2 IHC Score

HER2 overexpression in colorectal cancer Rate of protein overexpression or gene amplication ~6% in
recent study in mCRC
Lower rate in earlier stage disease, with suggestion that expression relates to outcome
Prior clinical trials limited by low frequency, although evidence of clinical activity
1Seo et al. PLoS One. 2014 May 30;9(5):e98528.² Ingold Heppner B et al. Br J Cancer. 2014 Nov 11;111(10):1977-84. ³ Ramanathan RK et al. Cancer Invest. 2004;22(6):858-65.

In summary KRAS/BRAF mutations are indicative of worse prognosis in Stage III colon
cancers
Vitamin D levels are prognostic in mCRC.
Radioembolization and chemotherapy in first-line setting for mCRC with liver only metastasis may be an option.
FOLFIRI + ramucirumab in 2nd line setting for mCRC has similar activity to prior anti-VEGF therapies
TAS-102 may soon be a new therapy for refractory mCRC
Targeted therapies for dMMR and HER2+ tumors are underway in clinical trials

Thank you!