Embed Size (px)
Citation preview
Use of Modelling and Simulation to Assess and Manage Individualized Risk of Drug-Drug InteractionHelen Humphries, Senior Research Scientist at Simcyp
© Copyright 2015 Certara, L.P. All rights reserved.
M&S to Assess and Manage Individualized Risk of DDI
• Importance of fm to risk of DDI
• Simcyp Approach
• Tablet and Smartphone App
– Static DDI and Population Representative
• Simcyp simulator
– Dynamic simulations and inter-individual variability
• The future – Virtual twin..
2

© Copyright 2015 Certara, L.P. All rights reserved.
• Systemic Clearance (L/h) = Metabolic Clearance (CLmet) + Renal Clearance (CLR)
• fm = fraction of the systemic clearance metabolised via enzyme
• fm is THE most important parameter contributing to inter-individual variability in the extent of DDI
Importance of fm to Risk of DDI
30% CYP3A4
29% CLR
41% CYP2C8
North European Caucasian PopulationMean of 1000 individuals
Inhibitor of CYP2C8
e.g., VICTIM DRUG X
© Copyright 2015 Certara, L.P. All rights reserved.
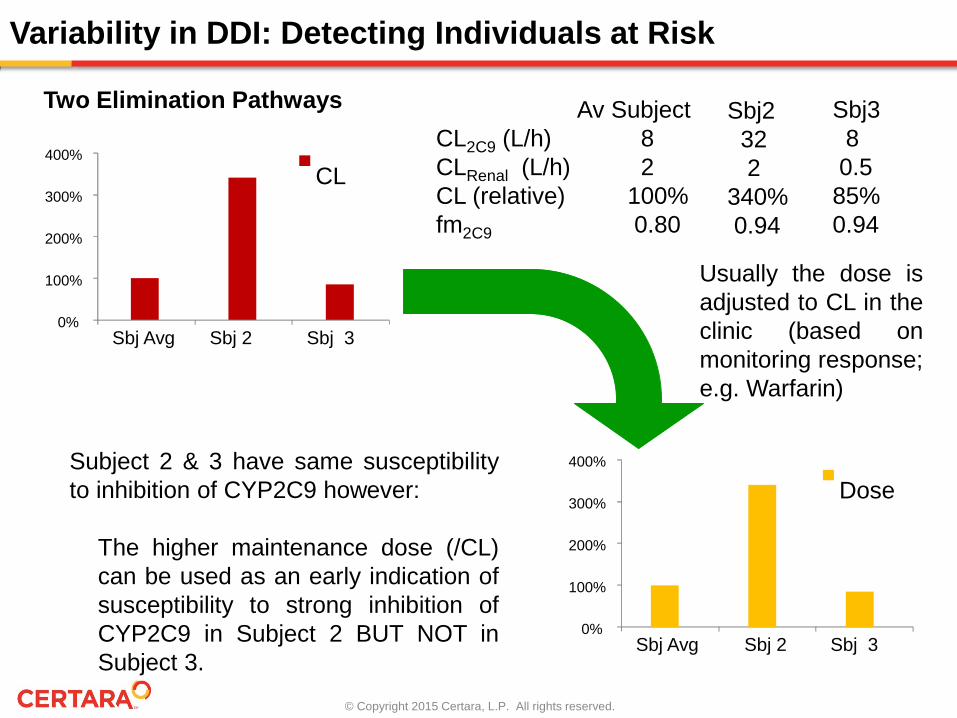
Variability in DDI: Detecting Individuals at Risk
Av SubjectCL2C9 (L/h) 8CLRenal (L/h) 2CL (relative) 100%fm2C9 0.80
Two Elimination Pathways
0%
100%
200%
300%
400%
Sbj Avg Sbj 2 Sbj 3
CL
Sbj232 2
340%0.94
Sbj380.5
85%0.94
0%
100%
200%
300%
400%
Sbj Avg Sbj 2 Sbj 3
Dose
Usually the dose isadjusted to CL in theclinic (based onmonitoring response;e.g. Warfarin)
Subject 2 & 3 have same susceptibilityto inhibition of CYP2C9 however:
The higher maintenance dose (/CL)can be used as an early indication ofsusceptibility to strong inhibition ofCYP2C9 in Subject 2 BUT NOT inSubject 3.
© Copyright 2015 Certara, L.P. All rights reserved.
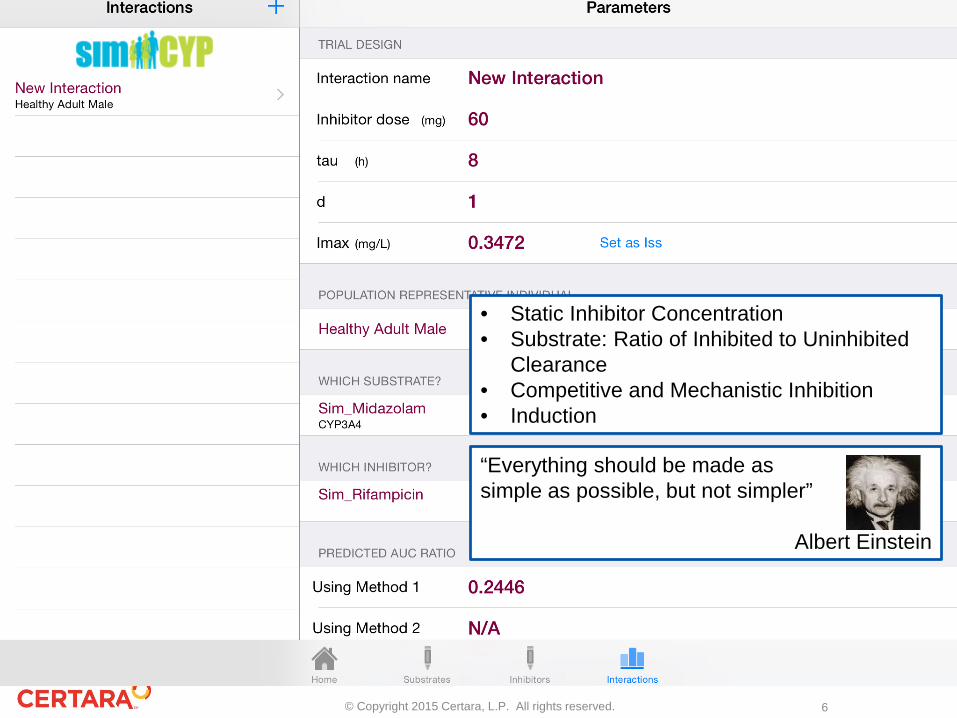
Apps for Tablets and Smartphones
5
© Copyright 2015 Certara, L.P. All rights reserved.
• Static Inhibitor Concentration• Substrate: Ratio of Inhibited to Uninhibited
Clearance• Competitive and Mechanistic Inhibition• Induction
“Everything should be made as simple as possible, but not simpler”
Albert Einstein
6
© Copyright 2015 Certara, L.P. All rights reserved.
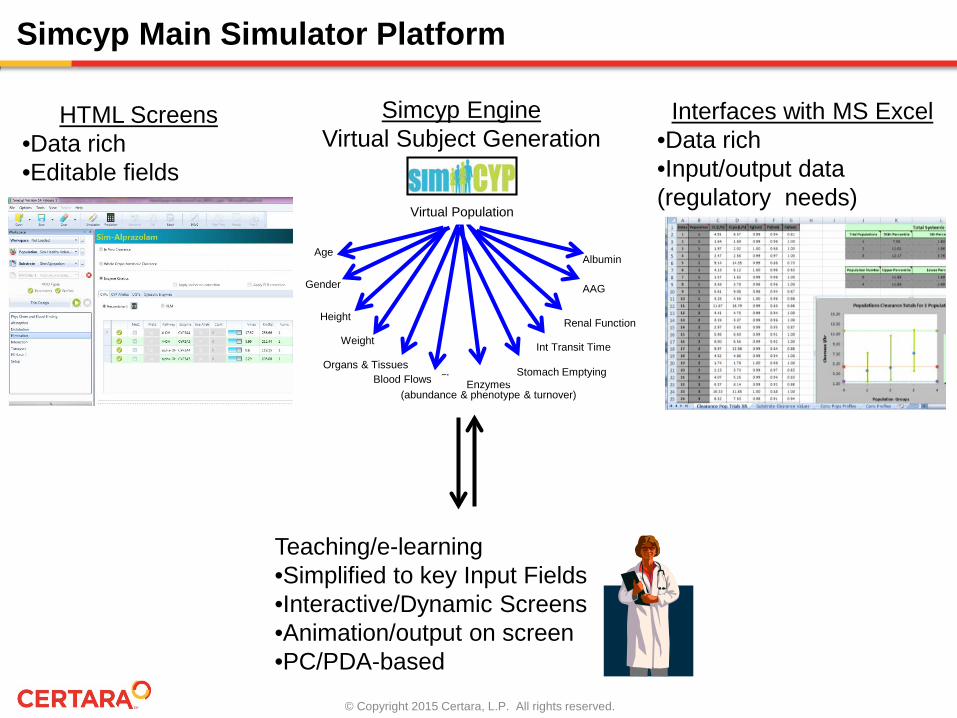
Simcyp Main Simulator Platform
HTML Screens•Data rich•Editable fields
Interfaces with MS Excel•Data rich•Input/output data (regulatory needs)
Teaching/e-learning•Simplified to key Input Fields•Interactive/Dynamic Screens•Animation/output on screen•PC/PDA-based
Simcyp EngineVirtual Subject Generation
Age
Gender
Blood FlowsOrgans & Tissues
Weight
Height
Albumin
AAG
Enzymes(abundance & phenotype & turnover)
Stomach Emptying
Int Transit Time
Renal Function
Virtual Population
Blood Flows
© Copyright 2015 Certara, L.P. All rights reserved.
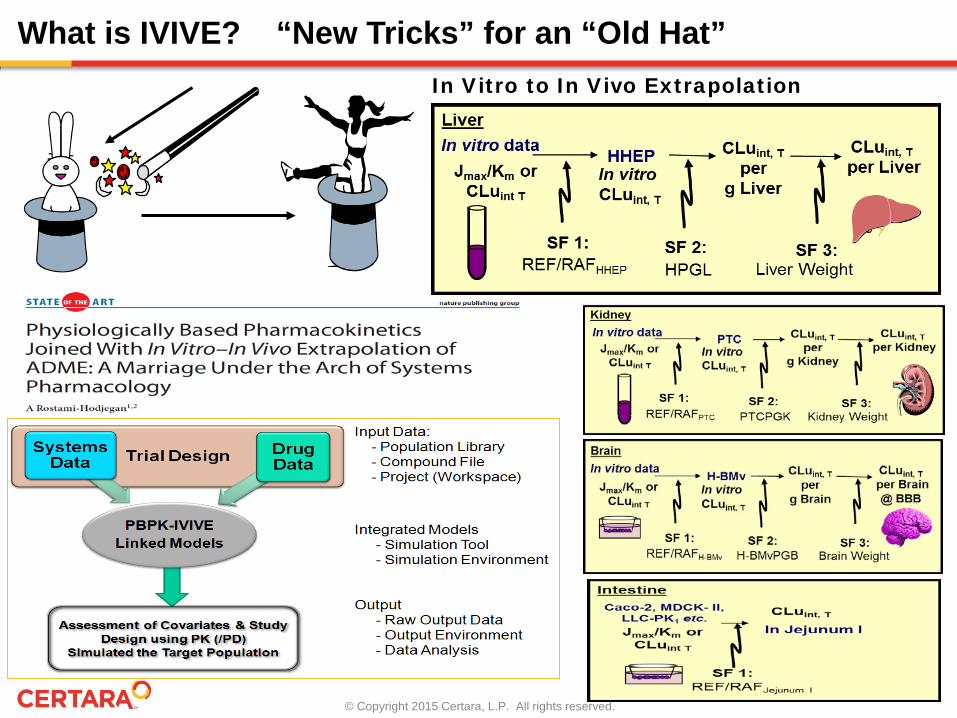
What is IVIVE? “New Tricks” for an “Old Hat” In Vitro to In Vivo Extrapolation
© Copyright 2015 Certara, L.P. All rights reserved.
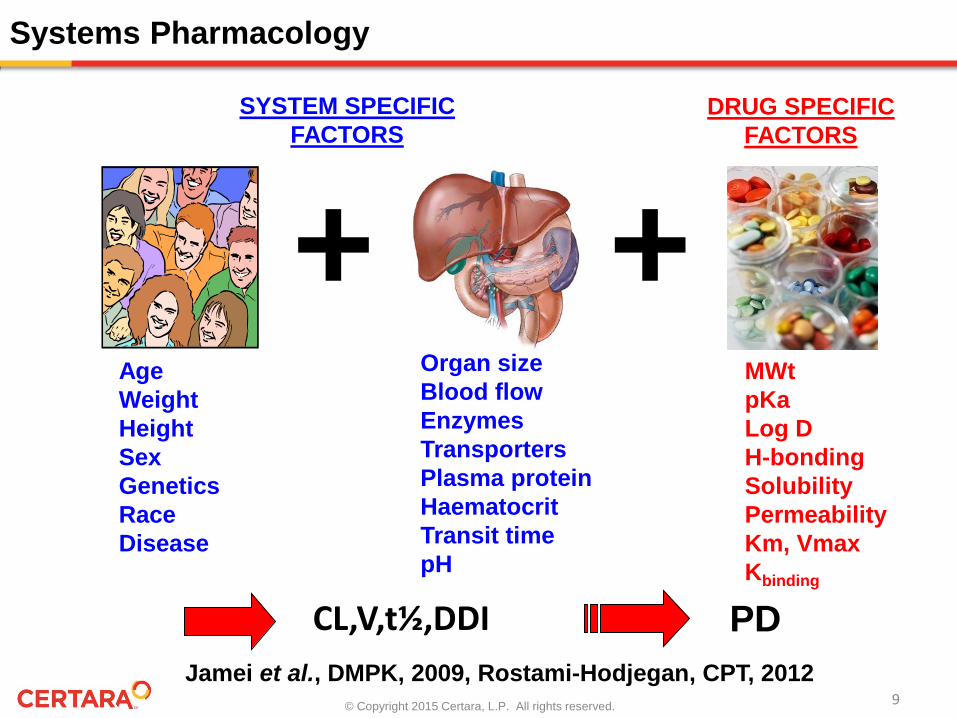
Jamei et al., DMPK, 2009, Rostami-Hodjegan, CPT, 2012
Systems Pharmacology
AgeWeightHeightSexGeneticsRaceDisease
Organ sizeBlood flowEnzymesTransportersPlasma proteinHaematocritTransit timepH
MWtpKaLog DH-bondingSolubilityPermeabilityKm, VmaxKbinding
SYSTEM SPECIFICFACTORS
DRUG SPECIFICFACTORS
++
CL,V,t½,DDI PD
9

© Copyright 2015 Certara, L.P. All rights reserved.
Physiologically-Based Pharmacokinetic Modelling (PBPK)
Rowland, Peck & Tucker – Physiologically-based pharmacokinetics in drugdevelopment and regulatory science – Ann Rev Pharmacol Toxicol 51: 45-73 (2011)
© Copyright 2015 Certara, L.P. All rights reserved.
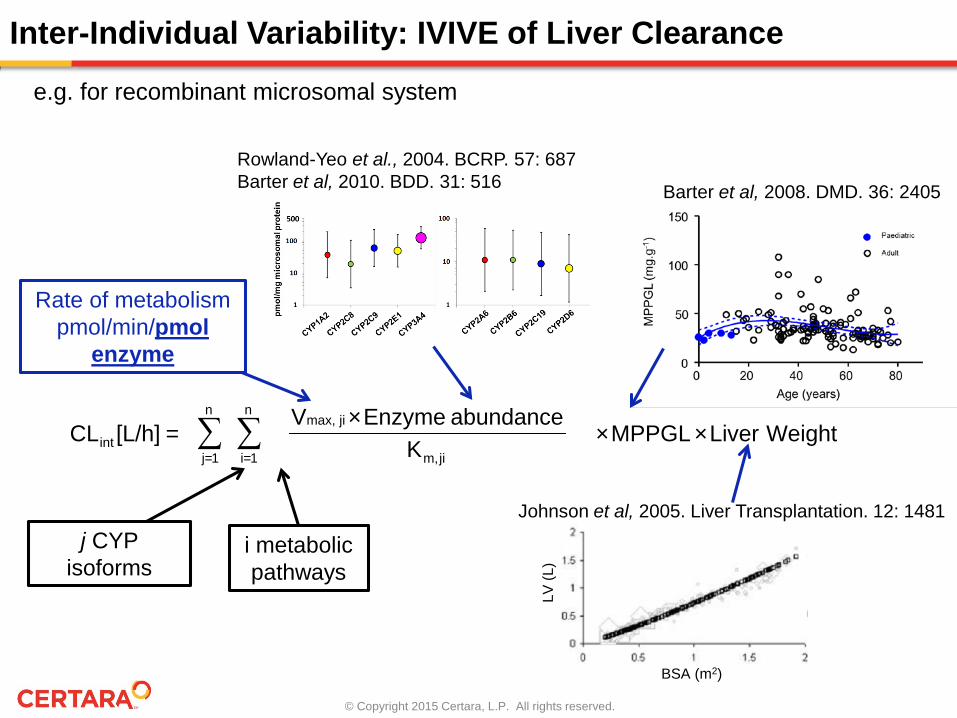
Inter-Individual Variability: IVIVE of Liver Clearance
WeightLiver×MPPGL×K
abundance Enzyme×V =[L/h]CL
n
1=j
n
1=i jim,
jimax,
int ∑ ∑
j CYP isoforms
i metabolic pathways
Rate of metabolismpmol/min/pmol
enzyme
e.g. for recombinant microsomal system
BSA (m2)
LV (L
)
Johnson et al, 2005. Liver Transplantation. 12: 1481
Rowland-Yeo et al., 2004. BCRP. 57: 687Barter et al, 2010. BDD. 31: 516 Barter et al, 2008. DMD. 36: 2405
© Copyright 2015 Certara, L.P. All rights reserved.
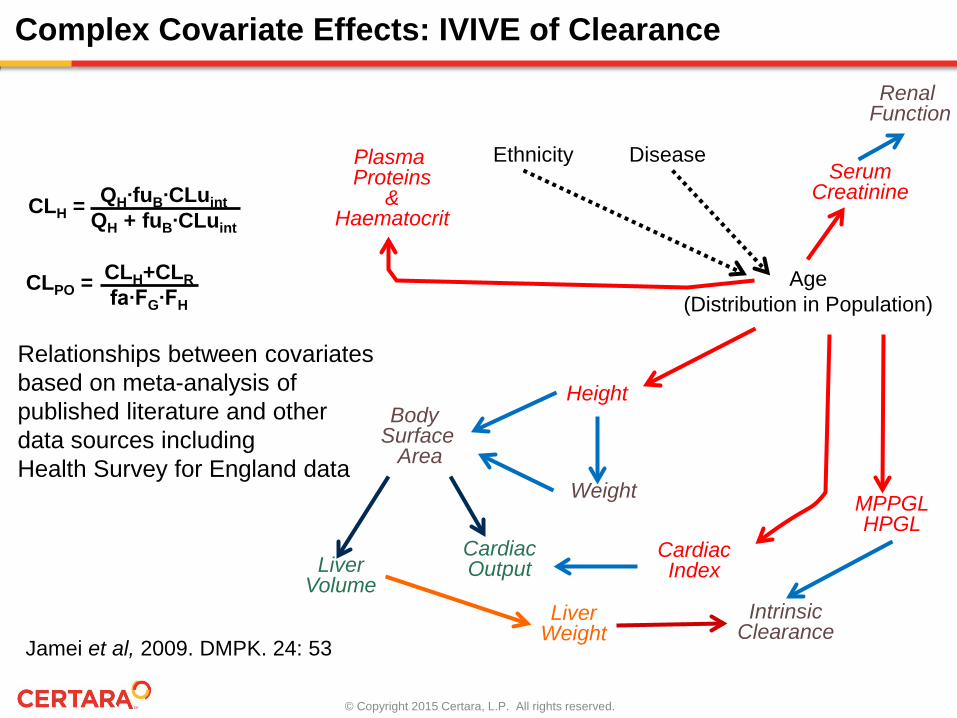
Age(Distribution in Population)
Ethnicity Disease
Height
CardiacIndex
MPPGLHPGL
Plasma Proteins
&Haematocrit
SerumCreatinine
Body Surface
AreaWeight
LiverVolume
CardiacOutput
IntrinsicClearance
Renal Function
LiverWeight
Complex Covariate Effects: IVIVE of Clearance
QH∙fuB∙CLuintQH + fuB∙CLuint
CLH =
CLH+CLRfa∙FG∙FH
CLPO =
Jamei et al, 2009. DMPK. 24: 53
Relationships between covariatesbased on meta-analysis of published literature and otherdata sources includingHealth Survey for England data
© Copyright 2015 Certara, L.P. All rights reserved.
Importance of fm to Risk of DDI
• Factors contributing to inter-individual variability in the extent of DDI do so through the impact on fm
• Cirrhosis Chalon et al., 2003. Johnson et al., 2010• Japanese Inoue et al., 2006• Chinese Barter et al., 2013• Obesity Ghobadi et al., 2011• Pregnancy Lu et al., 2012. Ke et al., 2012• Paediatric Salem et al., 2013 and 2014• Smoking Plowchalk & Rowland Yeo, 2012• Geriatric• Renal Impairment
– Tortorici et al., 2014. Rowland Yeo et al., 2011– Key PBPK parameters related to kidney disease
• Renal function, Cardiac output, CYP and transporter abundance, Gastric emptying, Albumin and Haematocrit
© Copyright 2015 Certara, L.P. All rights reserved.
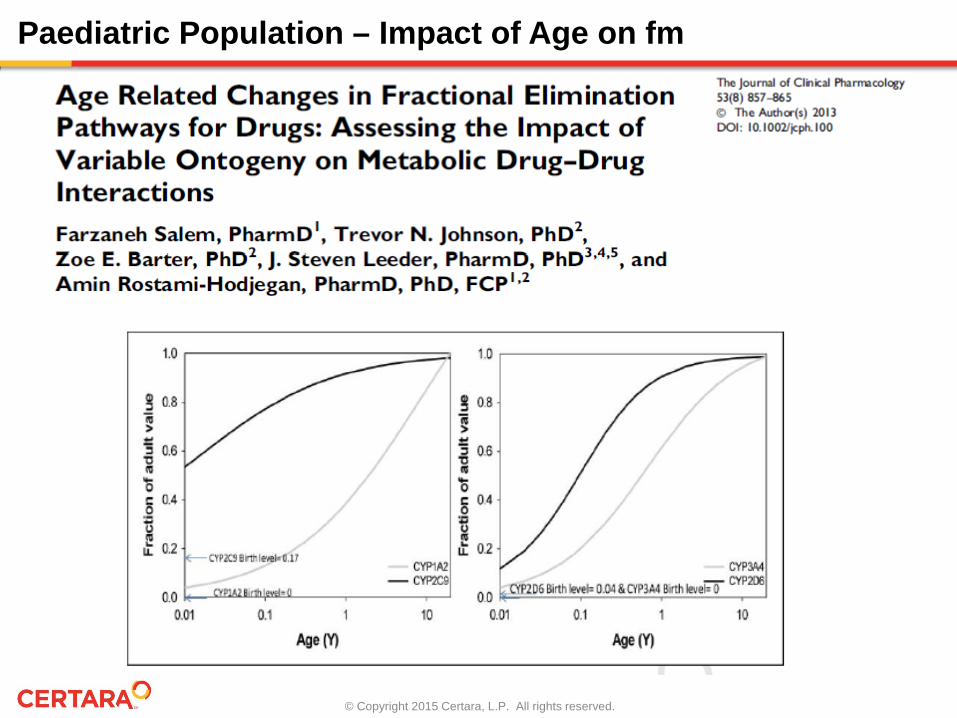
Paediatric Population – Impact of Age on fm
© Copyright 2015 Certara, L.P. All rights reserved.
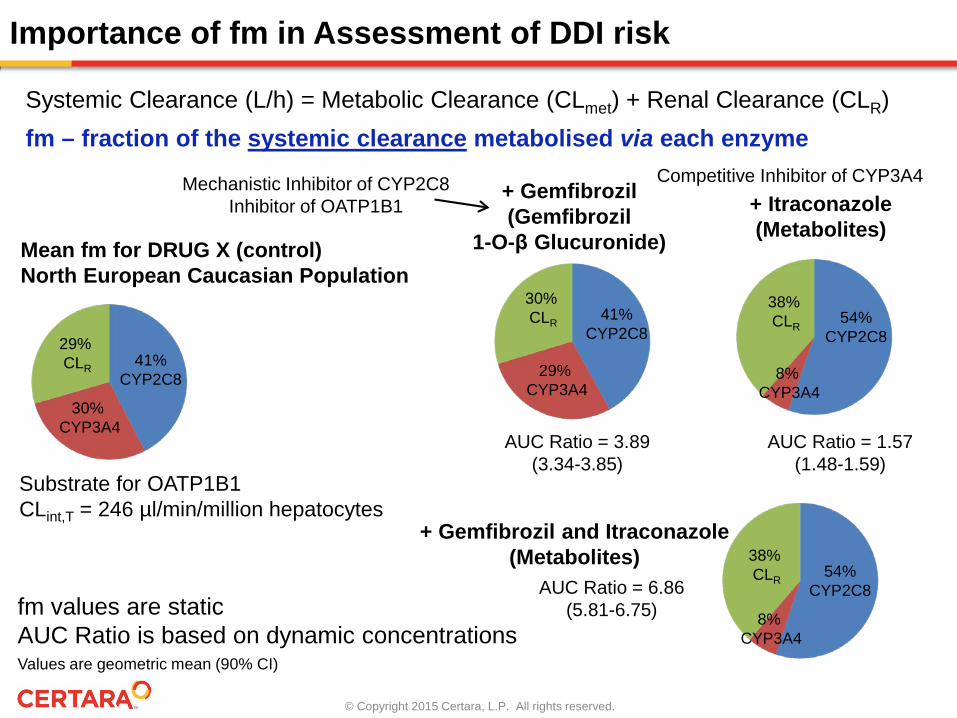
Importance of fm in Assessment of DDI risk
Systemic Clearance (L/h) = Metabolic Clearance (CLmet) + Renal Clearance (CLR)fm – fraction of the systemic clearance metabolised via each enzyme
30% CYP3A4
29% CLR 41%
CYP2C8
Mean fm for DRUG X (control)North European Caucasian Population
+ Gemfibrozil and Itraconazole(Metabolites)
AUC Ratio = 6.86 (5.81-6.75) 8%
CYP3A4
38% CLR 54%
CYP2C8
Values are geometric mean (90% CI)
Substrate for OATP1B1CLint,T = 246 µl/min/million hepatocytes
+ Itraconazole(Metabolites)
Competitive Inhibitor of CYP3A4
8% CYP3A4
38% CLR
54% CYP2C8
AUC Ratio = 1.57 (1.48-1.59)
+ Gemfibrozil(Gemfibrozil
1-O-β Glucuronide)
Mechanistic Inhibitor of CYP2C8Inhibitor of OATP1B1
29% CYP3A4
30% CLR 41%
CYP2C8
AUC Ratio = 3.89 (3.34-3.85)
fm values are staticAUC Ratio is based on dynamic concentrations
© Copyright 2015 Certara, L.P. All rights reserved.
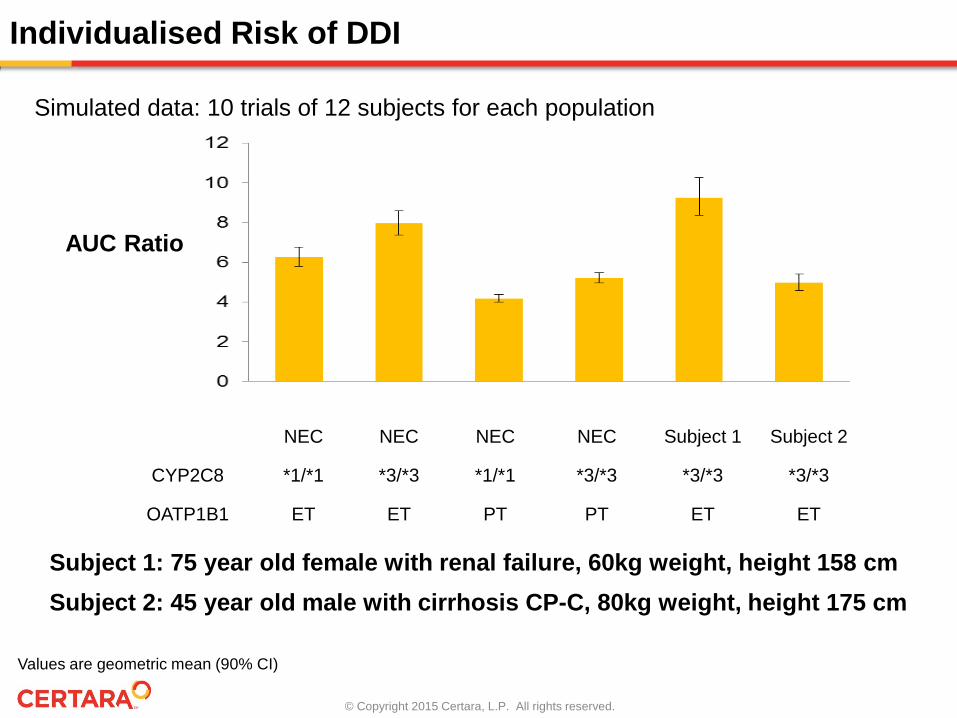
Individualised Risk of DDI
NEC NEC NEC NEC Subject 1 Subject 2
CYP2C8 *1/*1 *3/*3 *1/*1 *3/*3 *3/*3 *3/*3
OATP1B1 ET ET PT PT ET ET
Subject 1: 75 year old female with renal failure, 60kg weight, height 158 cmSubject 2: 45 year old male with cirrhosis CP-C, 80kg weight, height 175 cm
AUC Ratio
Simulated data: 10 trials of 12 subjects for each population
Values are geometric mean (90% CI)
© Copyright 2015 Certara, L.P. All rights reserved.
The U.S. Food and Drug Administration (FDA) has seen a recent increase in the application of physiologically-based pharmacokinetic (PBPK) modeling towards assessing the potential of drug-drug interactions (DDI) in clinically relevant scenarios. To continue our assessment of such approaches, the predictive performance of PBPK modeling in predicting CYP-mediated DDI was evaluated.
In 21/26 (81%) and 20/26 (78%) cases, respectively, AUC and Cmax ratios were within a pre-defined threshold of 1.25-fold.
These results suggest that, for submissions to the FDA to date, there is a high degree of concordance between PBPK-predicted and observed effects of CYP inhibitors on the exposure of drug substrates.
Experience on DDI - Possibility to Take a Position
© Copyright 2015 Certara, L.P. All rights reserved.
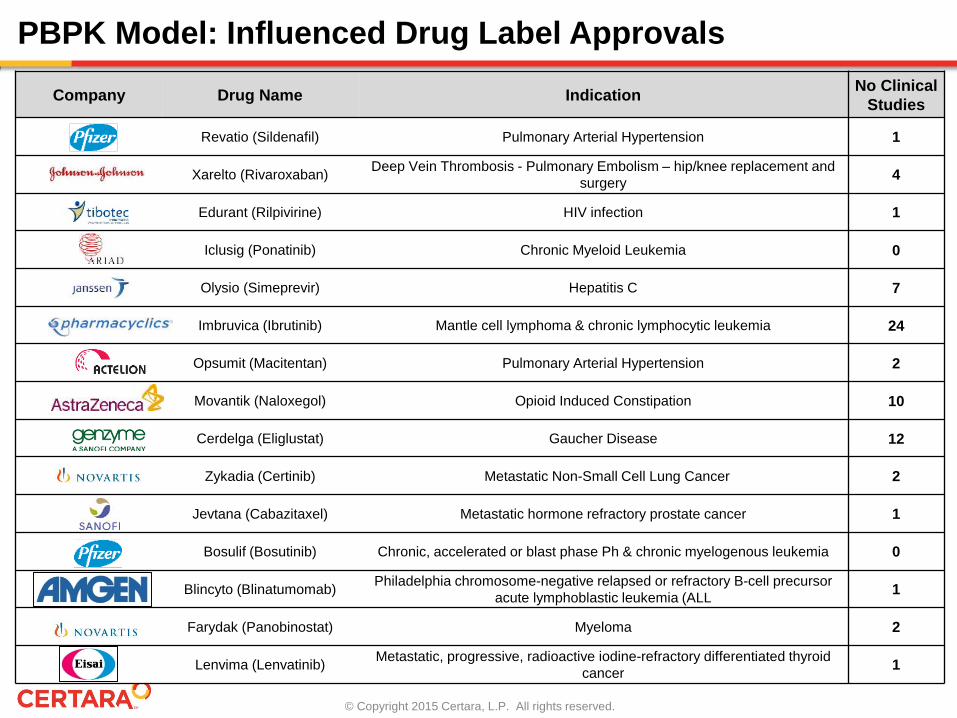
PBPK Model: Influenced Drug Label Approvals
Company Drug Name Indication No Clinical Studies
Revatio (Sildenafil) Pulmonary Arterial Hypertension 1
Xarelto (Rivaroxaban) Deep Vein Thrombosis - Pulmonary Embolism – hip/knee replacement and surgery 4
Edurant (Rilpivirine) HIV infection 1
Iclusig (Ponatinib) Chronic Myeloid Leukemia 0
Olysio (Simeprevir) Hepatitis C 7
Imbruvica (Ibrutinib) Mantle cell lymphoma & chronic lymphocytic leukemia 24
Opsumit (Macitentan) Pulmonary Arterial Hypertension 2
Movantik (Naloxegol) Opioid Induced Constipation 10
Cerdelga (Eliglustat) Gaucher Disease 12
Zykadia (Certinib) Metastatic Non-Small Cell Lung Cancer 2
Jevtana (Cabazitaxel) Metastatic hormone refractory prostate cancer 1
Bosulif (Bosutinib) Chronic, accelerated or blast phase Ph & chronic myelogenous leukemia 0
Blincyto (Blinatumomab) Philadelphia chromosome-negative relapsed or refractory B-cell precursor acute lymphoblastic leukemia (ALL 1
Farydak (Panobinostat) Myeloma 2
Lenvima (Lenvatinib) Metastatic, progressive, radioactive iodine-refractory differentiated thyroid cancer 1
© Copyright 2015 Certara, L.P. All rights reserved.
• Match characteristics of a real patient with his or her virtual twin – Age, Weight, Height, Sex, Race– Current drug dosage, Comedications– Activity of metabolic enzymes and transporters
• Genotype• Biomarkers
• Exploration of likely impact of co-medication and changes in organ function
• Management of drug dosage
• Important step on the way to truly ‘personalised/stratified’ medicine
The Future – The Virtual Twin
19
© Copyright 2015 Certara, L.P. All rights reserved.
• Global profiling of ADME proteins (enzymes and transporters) in different organs (individual fingerprint)
• LC-MS/MS Methods for proteomics– AQUA, QconCAT, PSAQ and Label-Free– Achour et al., 2014. Russell et al., 2013. Al Feteisi et al., 2015– Harwood et al., 2013 and 2014
The Future of Proteomics-PBPK
• Use of enzyme expression patterns in blood cells as a surrogate for organ levels (e.g., liver)
• Use of blood circulating mRNA and microRNA as a biomarker for disease (e.g., hepatitis in Zhang et al., PLOS One, 2014)
20
© Copyright 2015 Certara, L.P. All rights reserved.
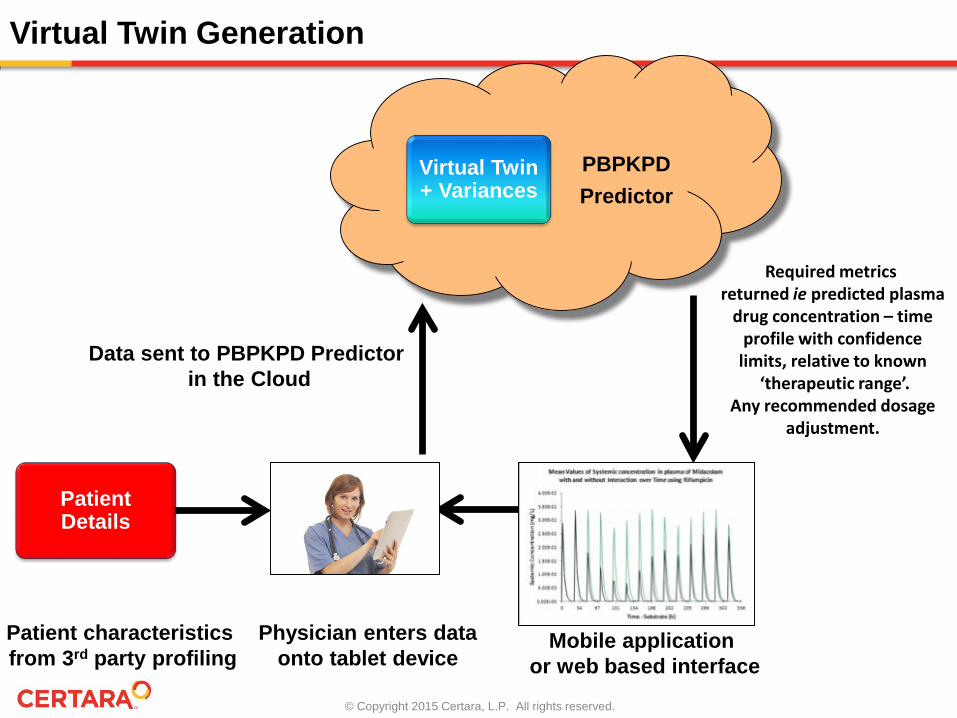
Mobile application or web based interface
Physician enters dataonto tablet device
Patient Details
Virtual Twin + Variances
PBPKPDPredictor
Virtual Twin Generation
Patient characteristics from 3rd party profiling
Data sent to PBPKPD Predictor in the Cloud
Required metrics returned ie predicted plasma
drug concentration – timeprofile with confidence
limits, relative to known‘therapeutic range’.
Any recommended dosageadjustment.





























