Embed Size (px)
Citation preview
Valuing Individuals – Transforming Participation in Chronic Kidney Disease
Learning and Sharing Event – Cohort 1
18 November 2015

Welcome and Housekeeping
Patricia Muramatsu
NHS England

Welcome and Housekeeping #empoweredpatients
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15 | 3
Programme for the Day
| 4
09:30 Registration opens and tea/coffee and snack available 10:30 Welcome and housekeeping 10:35 Overview of Programme by Richard Fluck and Jonathon Hope 11:00 Programme Methodology by Rachel Gair 11:20 Q&A Session 11:30 Health Foundation Presentation by Helen Crisp 12:00 Learning Needs Analysis – Group Work in Renal Teams 13:05 Feedback from Group Work 13:20 Lunch 14:00 Renal Unit Plans – 30-60-90 Day Group Work 14:50 Renal Unit – ‘Buddy Up’ 15:30 30-60-90 Day Revisions 15:45 Key message feedback 16:15 Next Steps 16:30 Close
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Overview of the Transforming Participation in CKD Programme
Richard Fluck
National Clinical Director for Renal Disease, NHS England
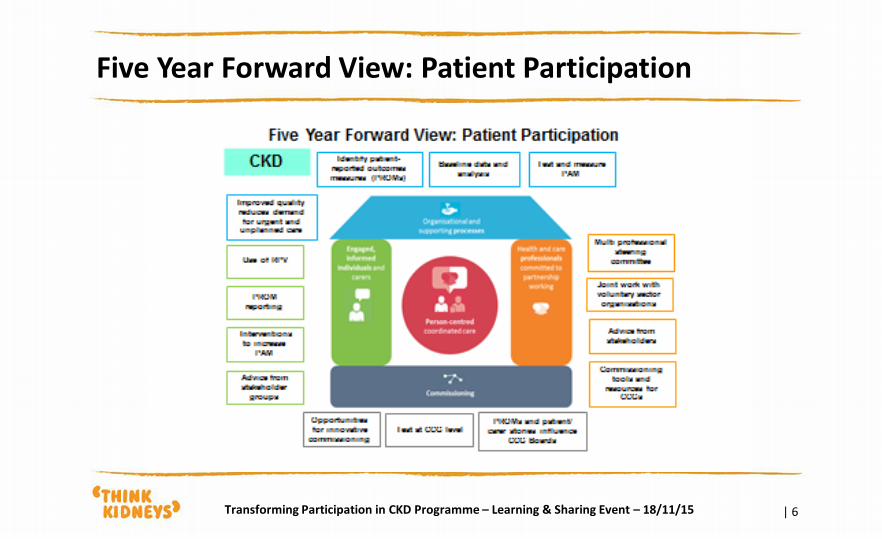
Five Year Forward View: Patient Participation
| 6 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
What is activation?
| 7
• An activated individual:
• Has the knowledge, skill and confidence to take on the role of managing their health and health care
• Informed choices
• Partner in care
• Self management/prevention
• Activation varies within age, income, education groups, even among people with low literacy skill
• Demographics tend to account for 5% to 6% of PAM score variation
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
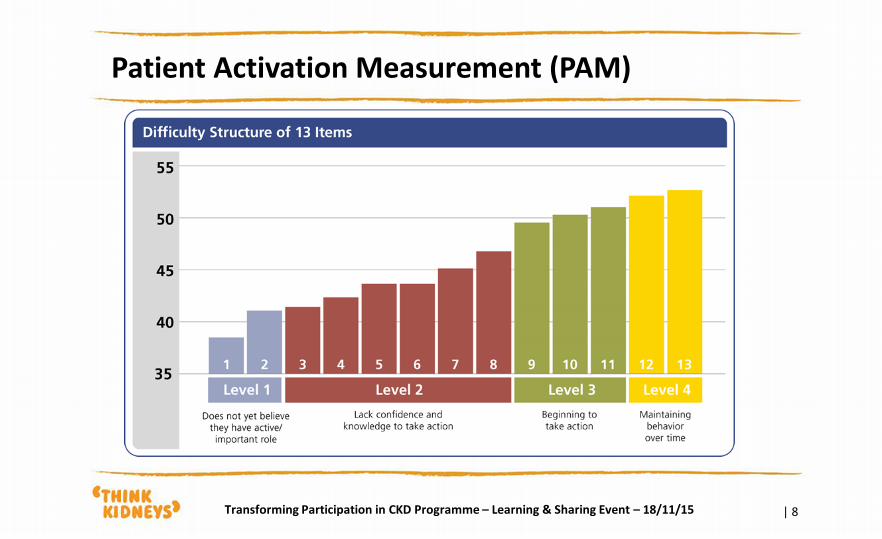
Patient Activation Measurement (PAM)
| 8 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Activation Level is Predictive of Behaviours
| 9
• Research consistently finds that those who are more activated are:
• Engaged in more preventive behaviours
• Engaged in more healthy behaviours
• Engaged in more disease specific self-management behaviours
• Engaged in more health information seeking behaviours
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Hypothesis for programme
| 10
Phase 1
• Can we gather PAM/CSPAM/PROM/PREM measures routinely?
Phase 2
• Can we bring in interventions that will increase a patient’s activation, segmented by PAM status, either directly or via effects on CSPAM?
• Are changes in PAM associated with improved outcomes across multiple dimensions?
Co-production as a core value
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
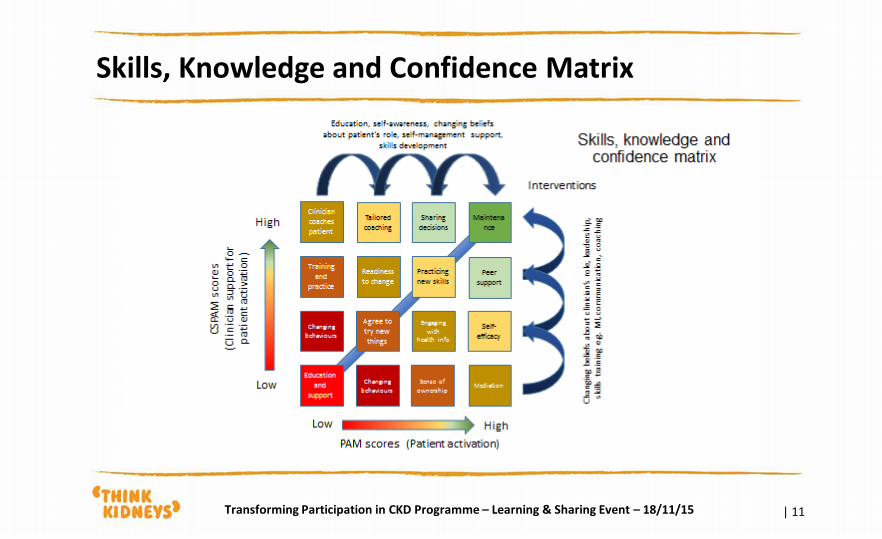
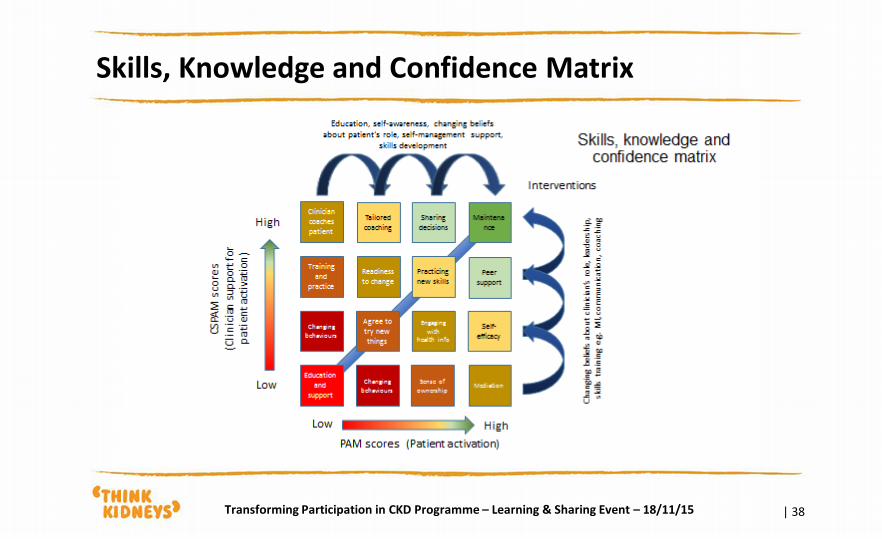
Skills, Knowledge and Confidence Matrix
| 11 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
The mission for today
| 12
How are you going to introduce patient activation measures (PAM) and Clinician support for PAM measures (CSPAM), patient reported outcome measures (PROM) and patient reported experience measures (PREM) into routine use within your departments?
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Overview of the Transforming Participation in CKD Programme
Jonathon Hope
Programme Board Co-Chair
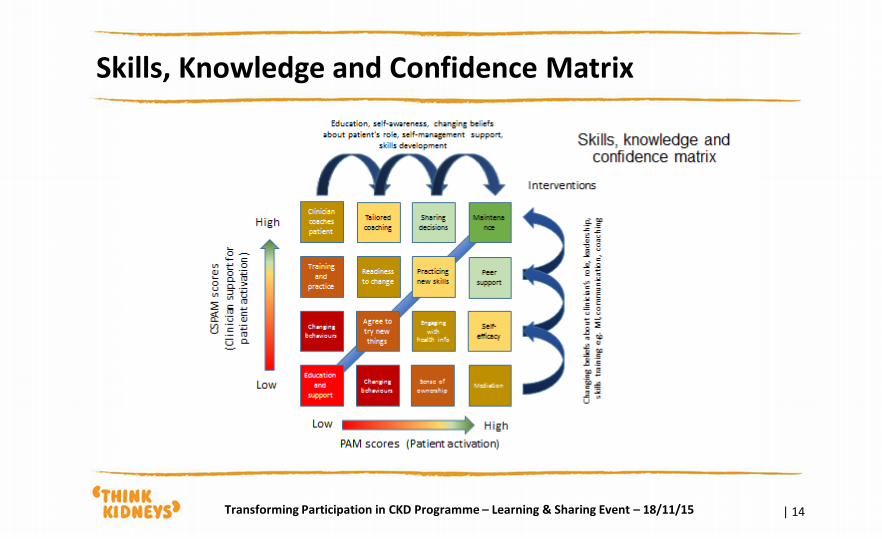
Skills, Knowledge and Confidence Matrix
| 14 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
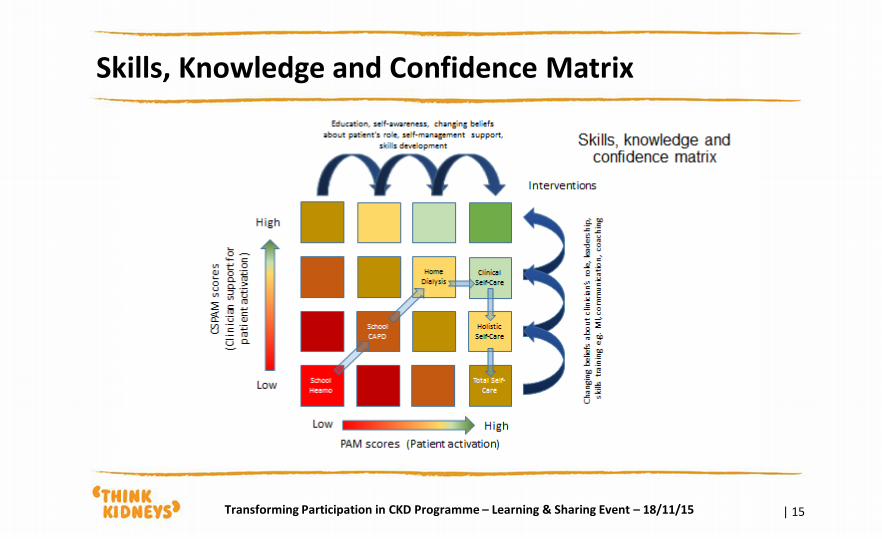
Skills, Knowledge and Confidence Matrix
| 15 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Programme Methodology
Rachel Gair
Person Centred Care Facilitator
| 17 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
To a patient centred approach…
| 18 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Person Centred Care
| 19
• Remember - Patients are ‘experts’ by their own experience
• Recognise - individuals own goals are what counts – it isn’t ‘to’ and ‘for’ but ‘with’ – Well being and independence are key outcomes of care
• Responsibility – Provision of tools and support people to take action and responsibility – action their own health & well being in partnership
• Support - to recognise and develop own strengths and abilities to enable them to live an independent and fulfilling
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Why Person Centred Care - Equality
| 20
• Challenging the concept of the ‘passive’ patient
• Replacing it with expectation on both sides of equivalently active roles in delivering a service/outcome
• Improving Skills, knowledge and confidence – patients and staff
• Recognising skills gifts and talents as well as needs
• We can’t magic up health and well being for another person – we know motivation changes outcomes
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
What are the questions the programme is asking?
| 21
• Can PAM/CS-PAM/PROM/PREM measures be collected routinely within renal units?
• Is the PAM related to PROM/PREM/Clinical Measure results?
• Can we introduce interventions that will increase a patient’s activation?
Co-production as a core value
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Patient Activation Measure – PAM?
| 22
• It is a survey of 13 questions
• It encourages the responder to think about how engaged and confident they feel in participating in health care decisions
• There is no right or wrong answer – it is individual
• The survey is ‘scored’ and used by you and the nurse/doctor to support your appointment
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
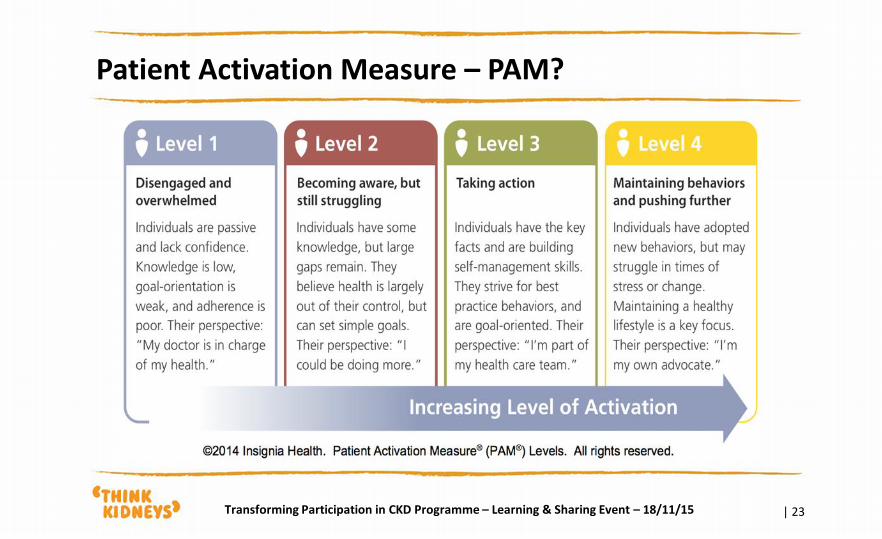
Patient Activation Measure – PAM?
| 23 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Patient Reported Outcome Measure – PROM?
| 24
• An additional 22 questions about your symptoms, how you are feeling and how you manage your everyday life.
• We want to find out about YOU as a whole person and your health and wellbeing - more than just your kidneys
• These questions will act as a prompt for you and the doctor/nurse to highlight what is important and what needs addressing – short & long term
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Patient Reported Experience Measures – PREM?
| 25
• Questions and themes about your care, the service, the environment, transport etc.
• These will be anonymous and won’t be seen by the clinical team
• They will be fed back to the team to inform service improvement
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Clinical Support – Patient Activation CS-PAM
| 26
• Do the renal teams and individuals support patient activation?
• Do they have the skills, knowledge and confidence to move to equal partners in care?
• Potential risk of conflict – activated patients but not clinical teams
• The results of the CS-PAM fed back to individuals but also provides a ‘heat map’ of the culture of the unit and what is required to gain a shift
• This is not about judgement but about Quality Improvement
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
How are you going to begin?
| 27
• Recommend the surveys are done with patients every 3 months as a minimum but may be done more regularly
• Paper to start with – develop on line Patient View access
• Start small in the 30-60-90 day plan and grow by 90 days
• Find out what works and what doesn’t work – record
• Peer Assist
• Peer Review
• Action Review
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Challenges
| 28
• Time
• Resource
• Work force
• Skills
• Other initiatives
• Not a priority
• We are already doing it
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Example 1 – haemodialysis unit
| 29
Haemodialysis patients – start small – every Wednesday/Thursday
• Handed paper questionnaire when accepted invitation to participate
• Either take it home or fill it in whilst on dialysis
• Hand it to nurse/doctor
• PREMS placed in closed post box
• PAM/PROM inform next discussion either on unit or in OPD
• Paper surveys sent by unit to UKRR
• UKRR generates feedback to patient and staff
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Example 2 - Outpatients
| 30
Pre-dialysis/Transplant – target a Monday pm clinic, a nurse led Tx clinic, individual consultant clinic
• Patients are handed surveys on attending OPD – each session
• Fill in surveys and take them into appointment
• Informs discussion - feedback
• Recorded in notes
• Surveys sent to UKRR
• PREMS posted in closed box
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Example - Patient Volunteers
| 31
• Utilise peer supporters to assist in helping with surveys on HD unit or OPD
• Utilise Trust volunteers
• Hand out patient leaflets and act as a resource for other patients
• Wear T – shirts to define role
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
What is Peer Assist?
| 32
A Peer Assist, also known as 'Learning before doing', is about a team asking for help
from their peers:
• People are invited to share their experience, insights and knowledge with the
team asking for help
• There would tend to be a spirit of reciprocity where people contributing would
be able to request help from the others to work on their own team's issues
• Check whether others have faced similar issues/ solved the problem
• Hold a problem solving/knowledge sharing session that involves the assisters
working together and presenting their recommendations and learning back to
the team after an initial briefing session
• Agree actions and any further reporting of progress
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
What is Peer Review?
| 33
• Peer review is a process used for checking the work performed by one's equals (peers) to ensure it meets specific criteria. Peer review is used because it is thought that peers can identify each other's errors quickly and easily, speeding up the time that it takes for mistakes to be identified and corrected
• Generally, the goal of all peer review processes is to verify whether the work satisfies the specifications for review, identify any deviations from the standards, and provide suggestions for improvements
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
After Action Learning
| 34
• The role of the PCC
• What did we expect to happen
• What happened
• What did we learn
• What will we do differently as a result
• Keep a log
• Regular contact with PCC to capture learning – telephone & F2F
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
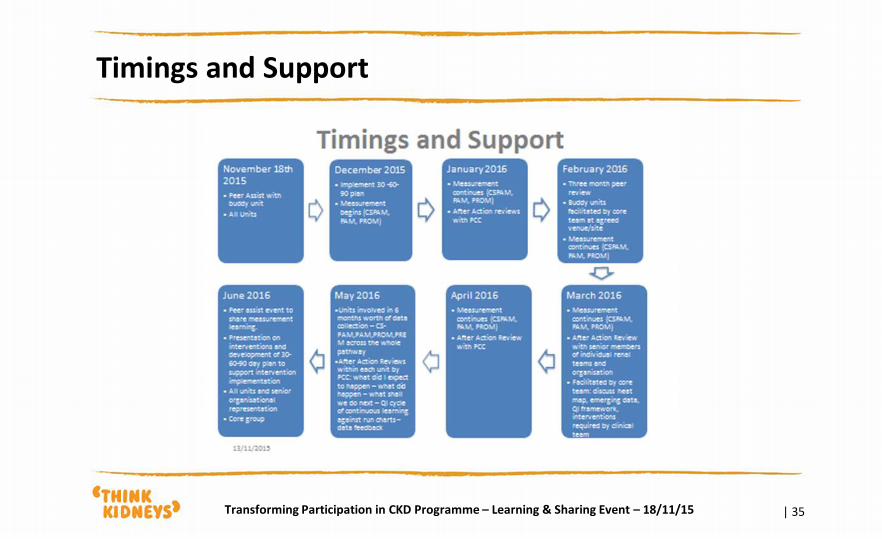
Timings and Support
| 35 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
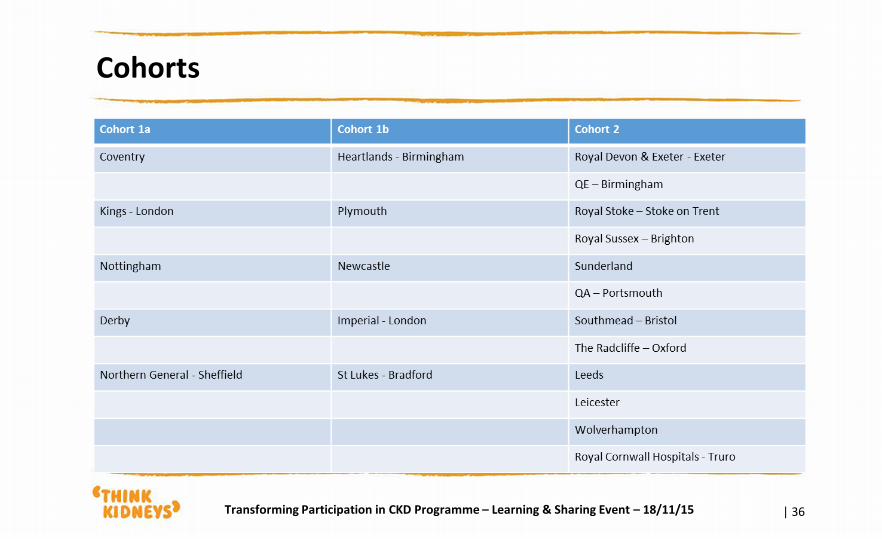
Cohorts
| 36 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Implementation – the ask!
| 37
• Begin collection of measurements across the whole pathway
• Start ‘small’ and then spread – OPD, HD, HHD, PD, TX
• Begin collection of CSPAM in each unit – building a heat map of unit
• We are looking at whether this is feasible – can this be done
• Not looking at comparing data from unit to unit – individual unit culture
• It won’t be significant or enable analysis as there will be bias/insufficient numbers
• Data is secondary – this is about improving the care that you deliver
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Skills, Knowledge and Confidence Matrix
| 38 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Karen Thomas
UK Renal Registry
Q & A Session
11.20-11.30

Helen Crisp
Health Foundation
Quality Improvement Resources
11.30-12.00
Health Foundation approaches to improvement Helen Crisp Assistant Director of Research
18th November 2015
Our mission: To improve quality of health and healthcare
1983 – Private Patients’ Plan Medical Trust established
1998 – sale of PPP to commercial insurer endows charity with £540 million
• Focus: medical research
2003 – re-launched as The Health Foundation focus on
• Improving quality of care
• Patient safety
• Person-centred care
2013 – New CEO – broader aims covering:
• Improving quality of care
• Health policy analysis
• Population health
Background to the Health Foundation:
42
What do we want?
43
Better health and health care
How does the Health Foundation help to achieve this?
44
Across the three areas of focus we:
test innovations and spread what works
build skills and knowledge
develop and share the evidence base

Research-led, theory-informed PERSON-CENTRED CARE
45
46
What are the aims for person-centred care?
47
• Better experience of care
• Better clinical outcomes
• Better use of health care resources
Our quick guide to help introduce the concepts
48
What is person centred care?
Why is person-centred care so
important?
How has person-centred care
developed?
Putting person-centred care
into practice
FAQs

What are the challenges?
49
• Perceptions of health care staff about person-centred care
We already do this

What are the challenges?
50
• Perceptions of health care staff about person-centred care
We already do this
Surveys in the NHS consistently report that over 40%
inpatients would like more involvement in decisions about
their care
What are the challenges?
51
• Perceptions of health care staff about person-centred care
• The changes require social and cultural changes more than
technical solutions
What are the challenges?
52
• Perceptions of health care staff about person-centred care
• The changes require social and cultural changes more than
technical solutions
• The evidence base is weak, contested and confusing
- Evidence review of shared decision making found 160
different definitions
- Many other studies with no definition
- ‘Same’ approaches have very different results
A research-led approach to person-centred care?
53
• Theory-based interventions using tested
methods
• Written up using SQUIRE guidelines
• Outcome measures; personal, process, clinical
• Robust evaluation using a range of innovative
methods
Why is research important for improvement?
54
To understand what we’re trying to do
To measure what we are doing and if it’s working
To report our work so others can learn
All publications available to download from:
http://www.health.org.uk/publications
Evidence Scans and Reviews
Original research
56
If you read one thing….
The Health Foundation has focussed primarily on two areas:
58
Self-management support
Shared decision making
What works?
59
Self-management support approaches
Motivational interviewing
Goal setting and action planning
Group-based educational
models Peer support
Self-management support approaches
60
Motivational interviewing
Goal setting and
action planning
Peer support
Counselling-oriented approach
to consultations
Aims to shift from medical model
to one to one support that
facilitates behaviour change
Used in Co-Creating Health to
train professionals
“ a professional life-changing event”
Training in
motivational
interviewing
described as:
Self-management
support approaches
61
Care and support planning
Goal setting and action planning
• Approach to help people
more effectively manage
long-term conditions
•Builds confidence by setting
attainable goals that matter
to the individual and step by
step plans to reach them
Key feature of Co-creating
Health
Self-management support approaches
62
Short courses for groups of people with
similar condition to support self-
management often led by an individual
who has a long term condition
“I’m happy for starting the group when I did. Learning things, pacing, helped to sort my life.”
STOP! Project in Dorset:
Group sessions to help people
live with chronic back pain
Self-management support approaches
63
Peer support
Group or one to one support from someone who lives with a
similar condition
Underpinned by key value of reciprocity
I’ll never be the same person I was before my diagnosis but peer support coaching has made me believe in a future where I can recover and develop the new me”
2Gether NHS Foundation
Trust: Coaching for recovery:
Effective shared decision making
64
• Decision aids
• evidence based
• include pros and cons of each
option
• use real-life examples
• use diagrams and visuals
“All need skills to use and attitude
trumps skill”
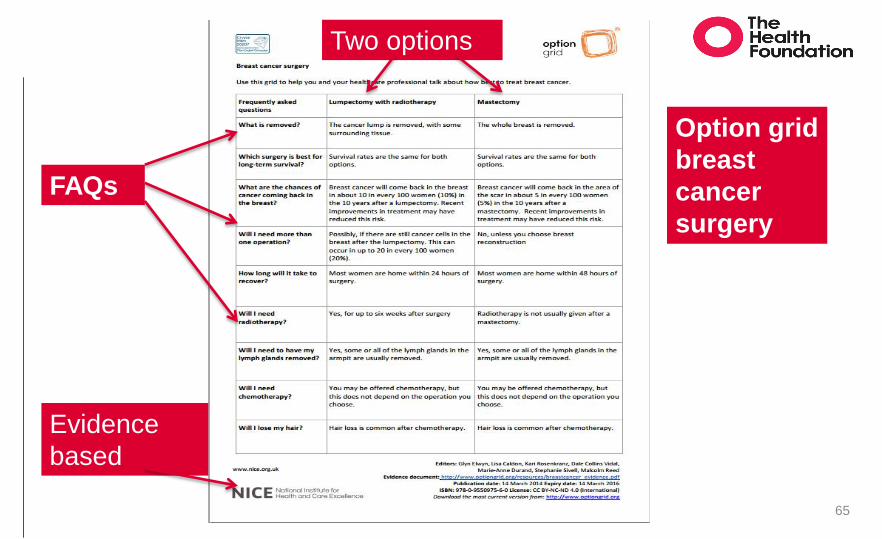
65
Evidence
based
Two options
FAQs
Option grid
breast
cancer
surgery
66
“ ‘Decision aid’ sounds very posh but it’s not ..This was about involving people in their care, and they had never been asked before”
Project lead, Newham COPD
Shine project ‘I probably… haven’t involved patients as much as I thought in the past … haven’t made them as aware of all the different options.’
GP, North Shields
MAGIC programme
Benefits to patients
67
More confidence for better day-to-day management of health
Able to make and sustain healthy lifestyle changes
Higher satisfaction with care experience
Better adherence to treatment plans and correct medicine use
Shared decision
aids
Motivational interviewing
Goal setting and
action planning
Peer support
Patient group
education
Next steps for implementation
68
Evaluating improvement interventions
69
Key evaluation question:
Did the improvement intervention fulfil its
intended objectives?
Sub-questions:
How was this achieved?
What resources did it take?
What unintended results were there?
Evaluation approaches
70
Summative
• Summarises the intervention effect at the end
Formative
• Findings shared and help to shape the intervention
Rapid cycle
• Frequent review of effectiveness of intervention
Developmental
• Intervention is still developing, all aspects reviewed and changes made in response
External evaluation
71
Often part of large scale, national or multi-site change
programmes
Independently commissioned from specialist teams
Great learning opportunity (NOT a threat!)
Share experience - the good and the challenging
More at: http://www.health.org.uk/publication/evaluation
-what-consider
72
Quick guides
73
Designed to get you
started
Sign post to other
resources
A way to introduce
new topics to patients,
staff, board members
Helping to build the evidence base
74
Better reporting of improvement work will:
Help spread successful improvement interventions
Prevent wasted effort on repeating interventions
that don’t work
Sharing and learning more
75
Reports on improvement work need not only results but also:
how the initiative was designed
the setting where it was implemented
detail on the core components
measures and data used to measure the change
challenges overcome along the way
how they were overcome
what the team would do differently in the future
Reporting bias
76
When reporting a successful intervention many improvement reports amount to:
“See, we did X!” versus “Here’s what we had to do to
achieve X”
Higher tendency to write up reports and submit papers and
abstracts when the improvement is ‘successful’
We can a lot from what didn’t work
Points to consider:
77
When do you start ‘writing up’?
How to capture the key
components of the improvement
initiative?
When barriers arise - how do you record these - and the action to overcome
them?
Some tips for writing up
78
Writing always takes longer than you
think – don’t leave it to the last few weeks
Robust data collection from the outset is
vital
Keep an ‘improvement diary’ to help
capture information as you go along,
particularly the adjustments
Involve others
79
Include different perspectives in your write up;
not just the improvement lead
other staff involved
staff not involved but affected by the change
service users
Reporting guidelines – a useful tool
80
SQUIRE guidelines
Standards for Quality Improvement Reporting Excellence
Checklist of points to consider when writing up improvement work
• Don’t leave it until you’ve completed the work
• Use guidelines to consider what data to capture as you go along
Download SQUIRE guidelines from:
http://www.squire-statement.org/
Consider the audience and where to publish
81
Core information remains but different emphasis for:
A report to the funder
Academic publication in a peer reviewed journal
Publication in a professional practice magazine
Beyond text:
Photos, videos, animations - bring the work to life
Spreading the word
82
Professionals listen to their peers
Think of a range of approaches - and use every opportunity:
Professional seminars
Conferences
E-mail bulletins and newsletters
Blogs
Communicating your work
83
Key concepts for spreading
ideas
Using comms approaches:
• planning your strategy
• engaging the right people
• sustaining interest
• celebrating and sharing
achievements

Resources to support improvement
84
For more information see: personcentredcare.health.org.uk
85
Web account
Keep in touch
87
Visit our website at www.health.org.uk
Subscribe to our monthly email newsletter at
www.health.org.uk/newsletter
Register for email alerts to be notified about our latest
work at www.health.org.uk/updates
Take part in conversation and debate about current
healthcare issues on our blog
Follow us on Twitter, Facebook or LinkedIn.
For all the latest news and developments
from the Health Foundation:
Learning Needs Analysis
Group Work by Renal Teams
Richard Fluck
UK Renal Registry
11.30-12.00
| 89
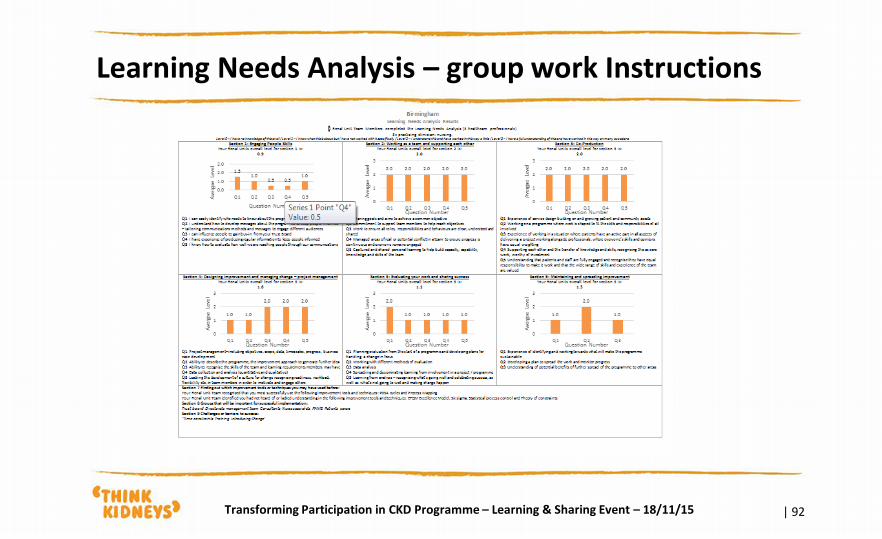
We would like your Renal team to tell us what learning support you would like in the following areas which you will recognise from the e-survey
Station 1: Engaging people
Station 2: Working as a team and supporting each other
Station 3: Co-production
Station 4: Designing improvement and managing change
Station 5: Evaluating your work and sharing success
Station 6: Maintaining and spreading improvement
Station 7: Improvement tools and techniques
Station 8: Important people for the work
Station 9: Challenges / barriers to success
Station 10: Coffee/Tea Station and Think Kidneys Website
Learning Needs Analysis – group work instructions
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis – group work instructions
| 90
• In your team start at one of the posters (the order of which your unit starts at is detailed in the instructions on your table)
• One hour is allocated for this task in which you will move round systematically from one station to the next. You will hear a “move to the next station” sound when you will move to the next station to to identify your learning needs as a team
• As you arrive at a station, locate your renal team name on the poster and provide notes and comments about the skills that are already available in the team and the additional support your renal team will need in this area
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis – group work Instructions
| 91
• You will also visit station 10 which will demonstrate the TP-CKD programme website and provide you with a much needed coffee or tea!
• As part of this task you will need to prepare your renal team’s ‘one key learning requirement’ and we will ask for this to be fed back to the wider group
• You will also find a summary of the Learning Needs identified by the pre-event survey in the instructions for your renal team. This identifies the skills you already have as a team as well as development needs
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis – group work Instructions
| 92 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis – group work instructions
| 93
• Please start at the station allocated below and work round in number ascending order
• Coventry Station 1 • Heartlands, Birmingham Station 2 • Northern General, Sheffield Station 3 • St Luke’s, Bradford Station 4 • Nottingham Station 5 • Newcastle Station 6 • Kings, London Station 7 • Plymouth Station 8 • Derby Station 9 • Imperial, West London Station 10
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis – station templates
| 94 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Learning Needs Analysis
Feedback from Group Work
Richard Fluck
NHS England
13.05-13.20
LUNCH
13.20-14.05
The mission for today
| 97
How are you going to introduce patient activation measures (PAM) and Clinician support for PAM measures (CSPAM), patient reported outcome measures (PROM) and patient reported experience measures (PREM) into routine use within your departments?
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
Renal Team Plans
30-60-90 Day Group Work by
Renal Teams
Karen Thomas
UK Renal Registry
14.00-15.45
Renal Team Plans 30-60-90 Day group work instructions
| 99
In your Renal team you have 2h 15m to discuss and agree what you would like
to achieve for your team from implementing the TP-CKD programme
To give you time to gather initial ideas, share with your partner team and make
any adjustments, the session is divided into sections
14:00 to 14:50 - renal teams discuss and agree their implementation plan (30,
60, 90 day plan) and complete the template provided
14:50 to 15:30 - buddy up with partner renal unit to start peer assist
15:30 to 15:45 - revise your plan following feedback
15:45 to 16:15 - decide on 1 key message from your plan to share with the
everyone
Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
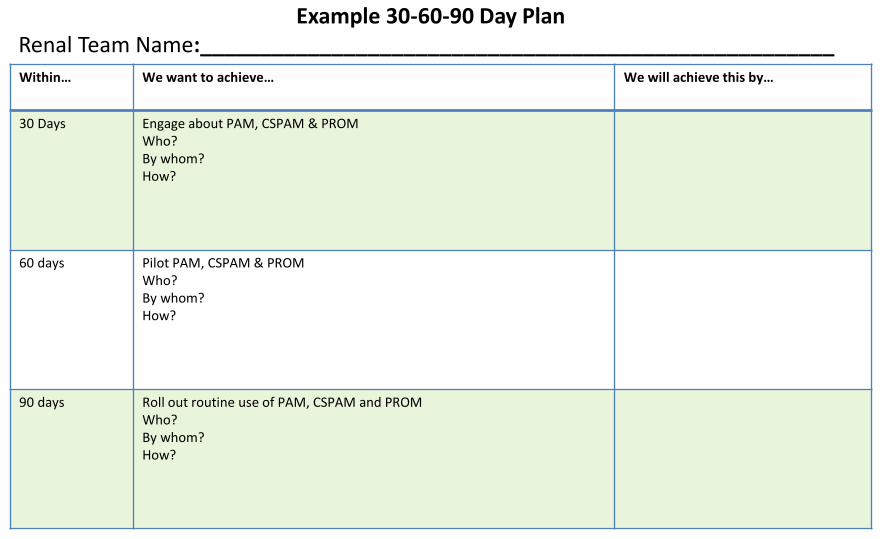
Within… We want to achieve… We will achieve this by…
30 Days
Engage about PAM, CSPAM & PROM Who? By whom? How?
60 days
Pilot PAM, CSPAM & PROM Who? By whom? How?
90 days
Roll out routine use of PAM, CSPAM and PROM Who? By whom? How?
Example 30-60-90 Day Plan Renal Team Name:_____________________________________________________
Within… We want to achieve… We will achieve this by…
30 Days
60 days
90 days
30-60-90 Day Plan Template Renal Team Name:____________________________________________________
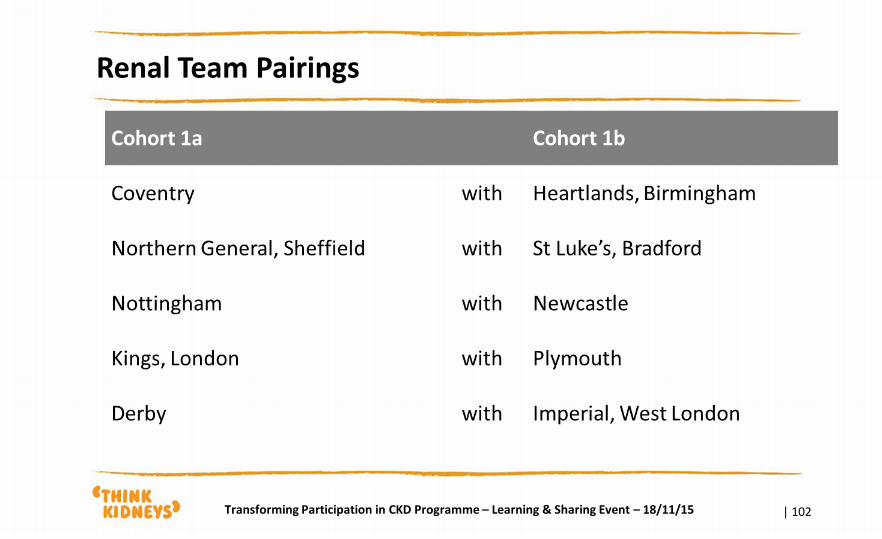
Renal Team Pairings
| 102 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15
30-60-90 Day Cycle
Feedback from Group work
Richard Fluck
NHS England
15.45-16.15

Next Steps
Richard Fluck
NHS England
16.15-16.30
Richard Fluck National Clinical Director for Renal NHS England [email protected]
Jonathon Hope TP-CKD Patient Co-Chair [email protected]
Patricia Muramatsu Senior Strategic Advisor Person Centred Care Team, NHS England [email protected]
How to find out more Karen Thomas Head of Programmes UK Renal Registry [email protected]
Sarah Evans TP-CKD Programme Coordinator UK Renal Registry [email protected] Rachel Gair Person Centred Care Facilitator UK Renal Registry [email protected] Ron Cullen CEO UK Renal Registry [email protected]
Contact Think Kidneys
www.linkedin.com/company/think-
kidneyswww.twitter.com/ThinkKidneys
www.facebook.com/thinkkidneyswww.
youtube.com/user/thinkkidneys
www.slideshare.net/ThinkKidneyswww.
thinkkidneys.nhs.uk
| 105 Transforming Participation in CKD Programme – Learning & Sharing Event – 18/11/15






![Valuing Prearranged Paired Kidney Exchanges: A Stochastic … · 2020. 9. 14. · ative merits and shortcomings of current PKE practice [11,15,16,27,36,39,40,43,45]. The Operations](https://img.pdfslide.net/doc/110x75/60da517635cc4603990f5028/valuing-prearranged-paired-kidney-exchanges-a-stochastic-2020-9-14-ative-merits.jpg)